Early Childhood Care and Development (ECCD) Policy Review in the Philippines
DRAFT FINAL REPORT
Prudenciano U. Gordoncillo Merlyne M. Paunlagui Ma. Theresa Talavera Resa J. de Jesus Deanie Lyn Ocampo Nelly C. Miranda
January 2008
EXECUTIVE SUMMARY
1.0 Introduction
The United Nations Education, Scientific and Cultural Organization (UNESCO) and the United Nations International Children’s Education Fund (UNICEF) aim to support Asia- Pacific countries in meeting the first goal of Education for All (EFA) through an assessment of the state of policy and implementation of early childhood development. Hence, said organizations launched, in September 2006, the Regional Early Childhood Care and Development Policy Review Project across nine countries including the Philippines.
In general, the review process aimed to support and assist the Philippine Government in meeting the goals of the ECCD Program by identifying, documenting, and sharing good practices as well as constraints in the policy development and implementation of early childhood care and development, which are aligned with other national sectoral plans as well as with the international commitments to the Millennium Development Goals (MDG), World Fit for Children (WFC), and Education for All.
Specifically, the objectives of the review included the following: 1) to determine the level of access to the basic ECCD services; 2) to identify the factors affecting the level of access; 3) to assess the quality of the ECCD services; 4) to characterize the nature of integration and convergence of ECCD services; and 5) to assess the feedback mechanisms and structure established for the program.
The conceptual framework for this Program review was drawn from the original ECCD framework adapted from Brofenbrenner (1988) in the baseline survey as well as in the evaluation study.
To establish the review in proper perspective, it is necessary to understand the interaction among the stakeholders of the ECCD Program across various levels – from an individual perspective, household, community, local government unit (LGU) level, and up to the national level. These interactions that influence the overall development of the child involves resources, events, values, and communications. The review will also be guided by the principle that intervention in early childhood development should be holistic and that the critical role of the primary care givers and the parents should be considered. Further, ECCD interventions should provide for the inclusion of vulnerable children, smooth transition from home-to-center-to-school, and gender sensitivity.
The specific areas of concerns or themes that the review process focused on include access, quality and the level of integration, and convergence of ECCD services. In terms of access, the following specific questions were addressed: What were the causes of low participation?; Was it a problem of availability, accessibility, affordability, awareness, or attitudinal?; and Who were the disadvantaged and the advantaged and how were the gaps generated?
The process of assessing the quality of service focused on the appropriateness of the intervention, content, standards, the mode of delivery, and the capacity and level of commitment among the service providers. Similarly, the review looked at the adequacy and appropriateness of ECCD infrastructures, facilities, and material support. It also assessed the sensitivity of the services to the cultural and social character of the communities.
ii
One of the guiding principles advocated for an ECCD intervention is that the approach should be holistic and integrated. Hence, the fundamental question addressed in the review process was in terms of the mode and extent of integration of the various ECCD services.
There were also cross-cutting issues that the review dealt with, particularly in terms of resources, governance and effectiveness of the delivery system. Source and mode of financing were also critical. In most developing countries, allocations of resources are often guided by political interest. Thus, there is a need to address the issues concerning the mechanisms instituted to insulate the program from political interventions as well as the structures established to define and delineate accountabilities. At the current phase of ECCD implementation in the Philippines, effectiveness was assessed through established mechanisms to operationalize the monitoring and evaluation component of the program.
To assess the mode and extent of integration of ECCD services, one needs to look at the household as the basic and focal unit. In a status quo, the state of the child development is determined primarily by the resources available at the household level. However, attitudes and values also play a critical role in the physiological and psycho- social development of the child. It is the interplay of these factors that basically determines the development of the child.
Therefore, any attempt to intervene towards the development of children in terms of health and nutrition, psycho-social and early education as well as social protection in an integrative manner will have to be focused at the household level, in general, and to the child, in particular.
2.0 Methodology
The cases were conducted in five provinces where the ECCD were already implemented. Two study sites each were selected from Luzon and Mindanao and one from the Visayas. The provinces of Cagayan and Zambales represented the island of Luzon; Leyte for Visayas; and Davao Oriental and Misamis Occidental for Mindanao.
The review used both qualitative and quantitative data. The process included three phases, namely: secondary data review, primary data collection, and analysis.
The secondary data included existing policies promulgated to effect child development, and a situational analysis based on published reports and statistical bulletins. The analysis situated the country’s current ECCD status in relation to the regional patterns and in relation to the country’s commitment to the MDG, WFC and EFA.
Primary data were collected through participatory rapid appraisal (PRA). This technique of data collection required the establishment of experts from various disciplines who conducted field visits within a period of four to five days. The team was composed of experts from the fields of health, nutrition, child development/early childhood education, development economics, sociology and social protection.
In every field visit, courtesy calls were made with the Provincial Social Welfare Office, Office of the Governor, and Office of the Mayor. Focus group discussions (FGDs) were conducted with the Provincial Early Childhood Care and Development Committee (PECCDC), Municipal Early Childhood Care and Development Committee (MECCDC), and the Barangay Early Childhood Care and Development Committee (BECCDC). In
iii
addition, the Provincial and Municipal ECCD Action Officer, Municipal Nutrition Action Officer, Social Development Worker, Rural Health Midwife, Grade 1 teacher, Kinder/Pre- elementary Teacher, and Day Care Worker served as key informants.
Secondary data were collected from the Provincial and Municipal Planning Development Office (P/MPDO), Provincial and Municipal Nutrition Office (P/MNO), Provincial/Municipal Social Welfare and Development Office (P/MSWDO) and Barangay. The secondary data provided relevant information about the province, municipality, and barangay.
3.0 Main Findings
While efforts have been made, malnutrition remains to be a problem in the country. Malnutrition exists primarily because it is highly linked with economic development. Developing countries like the Philippines have low income capacity which is a major cause for the inability to secure food. At present, the identified nutritional problems among preschool children are: 1) protein-energy malnutrition, 2) obesity, and 3) micronutrient deficiencies, i.e. vitamin A, iron, iodine and zinc.
There are, however, some encouraging signs of improvement. Given the declining trends in the prevalence of undernutrition in both preschool and school children, the interventions as embodied in the MTPPAN are apparently effective. Notable among these interventions are supplementary feeding; nutrition education including the promotion of breastfeeding and infant young child feeding; and essential child care services which includes immunization, growth monitoring, micronutrient supplementation, and integrated management of childhood illnesses. A major boost in the implementation of interventions is the Accelerated Hunger Mitigation Program (AHMP).
The general health status of Filipino children zero to six years old has been improving for the past decade. However, there is an apparent disparity in the health status of children among the different regions in the Philippines. This is demonstrated by the infant mortality rate wherein the national infant mortality rate has declined rapidly in the past eight years while a wide range of values was observed among regions. Furthermore, efforts to improve the health status do not seem to be sustained as evidenced in the decrease in the rate of decline in the maternal mortality rate in recent years. The same observations were noted in service delivery. For instance, there is disparity in the rate of fully immunized children and in NBS coverage among regions. Immunization rates for individual vaccines have not consistently improved through the years. Thus, there is a need for an integrative approach that will provide a more sustained improvement in health status and a more equitable delivery of services nationwide.
The preschool education services in the country are primarily provided by the government. As of December 2006, if the benchmark is one day care center per Barangay, then the country still needs about 9,208 centers nationwide. Moreover, about 10 percent of the DCCs do not have a Day Care Worker. Because of the limited availability of data for the preschoolers, the review focused on some of the studies conducted on the subject, which has established that the participation rate of children aged zero to six in preschool services has been relatively low because of the economic cost.
The statistics indicated that there is an urgent need to address child protection issues. It was estimated that there are about 50,000 street children and based on a sample, about eight percent were between two to five years old. Moreover, one of five children
iv
between zero to six have some form of disability. This would have significant implications to the Education for All goals.
The review has established that there are more than enough legislations designed to promote early childhood care and development. Before the year 2000, various statutes were promulgated to cater to sectoral concerns in ECCD including nutrition, health early education, and child protection. The promulgation of the ECCD Law (RA 8980), is again a very significant positive step towards achieving the ideal mechanisms for early child development. However, there is an apparent need to reconcile some of conceptual basis of the previous laws in relation to the provisions of the ECCD Law and to the visions of early child development.
The main ECCD interventions that were seen in the field across the study sites were reflections of the usual programs implemented under the various statutes promulgated before the ECCD Law. The fact that there is a prospect of funding support from ECCD generated the enthusiasm and commitment from various stakeholders at the field level. In spite of the difficulties encountered, the commitment of the members of the coordinating committees and service providers to provide service kept them going. The implementation of the ECCD program made them realize the importance of their role in caring for children 0 to 6 years old. The support of the local government also helped them in the implementation of the ECCD program. As a result of the ECCD implementation, there had been some expansion of the regular ECCD services, rehabilitation of existing facilities, upgrading of ECE materials and capacity building among the various service providers and stakeholders of the ECCD program.
Access to basic ECCD services is limited mainly due to inadequate resources including manpower and delayed release of ECCD funds. Moreover, the location of the health center or the day care center to some of the households in the barangay may prohibit their access to the ECCD services.
In terms of the quality of ECCD services, there is a need to improve them at the level of inputs (manpower and resources), process, and results. Manpower was found to be insufficient in terms of number (MNAO, BNS, midwife) and capacity to perform the tasks expected of them due to inadequate training. Moreover, the materials and facilities were found to be limited mainly due to the delay in the release of funds. In terms of process, there is a need to strictly follow the protocol and guidelines issued for the implementation of some ECCD services, e.g. conducting a supplementary feeding activity should be 90- 120 days; use of the eight-week curriculum for the new Grade 1 pupils so as to uphold the standards in all ECCD areas and for the full realization of the effect of the services. As to the quality of results, evaluation of the ECCD services is needed to be able to determine their effectiveness.
Integration and convergence are concepts that are not yet internalized at all levels including the household. In fact, the implementation of ECCD services as one integrated program needs to be promoted at the barangay and household levels. Thus, there is a need for new strategies and activities to which these concepts can be elevated from awareness to understanding level at household, barangay, municipal, and provincial levels. Moreover, there is a need to improve the feedback mechanism from the household up to the national level.
The critical challenge of the ECCD implementation is the operationalization of the mandate to provide a system based on multi-sectoral and inter-agency collaboration in the delivery of a comprehensive, integrative, and sustainable ECCD services at various levels from the national to the local levels of implementation.
v
4.0 ISSUES
While significant and notable improvements were observed across the various case study sites, there is a need to input the insights generated in the review process to allow for the modification of existing policies and processes in order to promote a more efficient implementation, enhance, and sustain the gains as a result of program interventions.
4.1 Alignment of Previous Laws on Children with RA 8980
While the ECCD Law is a very significant positive step to provide the mechanisms to integrate and harmonize prior ECCD initiatives, there are apparent issues relating to the consistency and alignment of previous laws with the ECCD Law. In terms of scope, most previous laws have mandates covering a broader age group for children. However, the ECCD law was very specific in its intention to cover only children between zero to six years old. This would have very critical implications, particularly in terms of coordination, jurisdiction and monitoring. For instance, in most child protection laws, the scope covers children beyond six years old. Hence, in terms of monitoring, the current system does not allow for an easy decomposition of the clients and their needs in terms of a structured age-group.
The passage of the local government code also has significant implications to the implementation of ECCD. Under the devolution, basic services such as ECE were delegated down to the smallest political administrative unit of the government: the Barangay. As a consequence, the data for ECE had been scanty particularly at the provincial, regional and national levels. This is partly due to the fact that LGUs do not see either the need or the obligation to provide ECE information beyond their immediate level of jurisdiction and mainly due to lack of mechanism to integrate the information beyond the municipal level. In most cases, the level of data aggregation is only up to the municipal level.
4.2 Less Emphasis on Child Protection
In the declaration of policy, the ECCD Law was very explicit in saying that “… promote the rights of children to survival, development and special protection with full recognition of the nature of childhood and its special needs….Section 2”. Further, in the identification of the duties of the Barangay Council for the Protection of Children, child protection was explicitly mentioned. However, in the implementation, most of the services provided for under ECCD were mainstream ECCD programs such as nutrition, health and ECE. Protection and special needs issues are seldom incorporated. For instance, the team has never encountered special learning sessions for disabled children.
Further, the notion of “Protection” as operationalized by BCPC under P.D. 603 has assumed a legalistic character and practice. Children are generally being provided services by government institutions/agencies, when such children become victims of abuse, neglect, and abandonment by parents or guardians. This unbalanced emphasis on the legalistic practice appears rather reactive rather than proactive, in the sense that no prevention strategies have been designed to counter the rising incidence of children in need of special protection.
vi
4.3 Cost-Sharing (Equity) Scheme
As a matter of policy, funding for ECCD interventions is supposed to be done under a cost-sharing scheme. Feedback from the focus group discussions indicated that the sharing was about 70:30, that is, 70 percent of the cost will be funded under the program and the remaining 30 percent will be funded as equity by the LGU. Some local government executives forwarded the argument that the 30 percent equity is very high, particularly for a 5th class municipality. In fact, one of the barangay officials indicated that the barangay may only be able to raise the required equity for a specific ECCD project in three years time.
4.4 Sustainability of ECCD-Hired PECCD Coordinator
In one of the case sites, it was noted that the provincial ECCD coordinating officer was directly hired from the ECCD program management. As a result of the financial incentive, the level of effort of the hired ECCD officer was relatively high. The coordination effort was very good which resulted in the substantive participation of the various agencies involved in ECCD implementation, particularly in the planning stage at the provincial level. However, the sustainability of a directly hired officer under the ECCD framework may be put into the test as soon as funding for the program is terminated.
4.5. The Role of Parents in the Day Care Center Sessions
During the site visits, it was observed that majority of the parents stayed with their children at the premises of the day-care centers during session hours. In one of the sites, about five mothers were with their children inside the day care centers to monitor their children; while the majority of the parents were just outside waiting for the session to end. The fact the parents stayed with their children during the entire course of the day care center sessions defeats the very purpose of the center, which was intended to cater to the need of the working parents. The fact since most of the enrollees now of the day care centers are non-working parents (by virtue of their willingness to stay with the child in the center) may indicate the real targets of the centers, which are the working parents, may have been disenfranchised by the non-working parents.
The other relevant issue associated with the role of the parents in the day care centers was the interest of the parents for their children to acquire added skills that would prepare their children for the formal elementary education. This attitude would not be in
4.6 Transition from Day Care Centers to Grade One
In the preceding section, it was noted that parents stayed with their children during the sessions at the day care centers. As a consequence, children were unable to get used to being independent in the class.
The field visits revealed that many parents stayed within the school premises to wait for their new Grade 1 children. This issue was highlighted in one case where a child cried and refused to enter the Grade 1 classroom fearing that her mother would eventually leave her behind as soon as she enters the class room. Hence, the inability of the children to develop independence at the early education stage is carried over during the transition to grade one.
vii
4.7 Inappropriateness and Inadequacy of Instruction Materials for the Eight- Week Curriculum
Grade 1 teachers (GOT) are required to attend the training for the implementation of the eight-week curriculum for GOTs. However, there were no provisions for instruction materials. Thus, GOTs either prepare or buy visual aids which may not conform to the prescribed ones. This was observed in one of the field visits where the Grade 1 teacher used materials with inappropriate examples. Further, while the ECCD law was explicit in the promotion of location-specific learning materials, this has not been operationalized yet at the barangay level. In fact, in one of the sites visited, the learning materials found in the DCC were still learning materials from the developed countries like the United States, United Kingdom, and Australia, among others.
4.8 Insufficient Manpower
Day care activities at the day care center vary from playing to feeding, to other developmental activities. Thus, a day care worker is burdened with many activities especially in the administration of the daily day care learning sessions. A class of about 20 children will be very difficult for a single day care worker.
4.9 Sectioning of the School-Ready and Not School Ready Pupils
In some instances, the number of identified non school-ready pupils was considerably low. To mitigate this situation, the non-ready pupils were separated into another section which was to be handled by another teacher. However, there is no curriculum for the non-school ready pupils. As such, the head teacher simply made the instruction to the teacher-in-charge of the non-school ready to tone down the level of treatment. This was compounded by the fact that the teacher-in-charge of the non-school ready did not attend the training program for the eight-week curriculum. The problem became more complex in cases where there is only one classroom for the new Grade 1 entrants, which would be expected in most of the communities under the ECCD program.
4.10 ECCD Monitoring System
One of the key elements to an effective delivery of ECCD services is an efficient monitoring system. During the field visits, effective monitoring system seemed absent particularly at the barangay level.
To dramatize the point, in one of the sites visited, there was very minimal nutrition intervention because the Barangay Nutrition Scholar declared that the incidence of malnutrition was insignificant. However, the extent of malnutrition among new school entrants in the same community was relatively high. In fact, the incidence was about 33 percent. This is an anomaly because malnutrition can not just happen overnight. If the extent of malnutrition among zero to six children was practically insignificant, where would the malnourished children among the new Grade 1 entrants be coming from?
4.11 Misconceptions on ECCD Integration
In the true sense of the word, the ECCD services at the time of this review are not yet integrated. The providers and stakeholders view that the services are
viii
already integrated because the centers are offering the various ECCD services and that, the process entailed the participation of various agencies of government and NGOs. However, it is argued here that the true essence of an integrated ECCD services can be characterized by convergence. For ECCD services to be more meaningful and effective, such interventions must converge to a specific household which covers both the parents and the children. An ECCD facility can readily report excellent statistics of increased level of reach in PES, IMCI, EPI, OPT, and feeding, among others. But it is not very effective if PES goes to one of the parents in one household, IMCI goes to the first child in another household, feeding to the third child in yet another household, and so on.
4.12 ECCD Visibility and Advocacy
While ECCD has been going on for quite sometime in most of the study sites, the household level discussions revealed that the extent of awareness about ECCD as a Program has been very low. In fact, some of the mothers interviewed never heard of ECCD. In one of the study sites visited, there was not even a single signage that would show the presence of the ECCD program in the community.
4.13 Multi- Tiered Schemes (ToTs)
To deliver the human resource development (HRD) component through training activities, the implementation strategy was to employ the Training of Trainors (ToT) concept. Feedback from the field visits indicated that there has been a significant departure from the standards of the acquired knowledge and skill by the local stakeholders through the ToT concept.
4.14 Overburdened BCPC
The Barangay Council for the Protection of Children was organized as the implementing body at the local level as provided for in P.D. 603. This council is basically composed of the BC, School Head, Barangay Midwife, BHW, BNS, DCW, SK Chairman, and a representative from the NGO.
Most of these personalities also constitute the Barangay Agrarian Reform Committee, which is also the implementing arm of one the most significant and controversial rural development programs in the country - the Comprehensive Agrarian Reform Program (CARP). The BCPC was also tasked as the implementer of the programs under RA 9344 or the Comprehensive Juvenile Justice and Welfare Act of 2006.
And now, with ECCD, the same personalities are again tasked with the implementation of yet again another significant development intervention of the government. It is agued here that these personalities are now overburdened with the responsibilities of implementing these various significant development programs of the government. Further, the BCPC was conceptualized to operate under the concept of voluntarism; hence, it has been difficult to recruit more competent members to the committee.
Furthermore, at the national, provincial, and municipal levels, the ECCD coordinating committees are supported by an ECCD secretariat. This was not made explicit under the law. Hence, at the Barangay level, there is a coordinating committee but without an ECCD secretariat.
ix
4.15 Sense of Project Ownership at the Community (Barangay) Level
One of the key informants in the study mentioned that while it would have been preferred that the level of authority be lowered down to the Barangay level, the fact that project disbursements are done at the municipal was accepted as a convenient excuse to avoid the accountability associated with fund disbursement. As a consequence, there was a feeling of alienation on the part of the local government unit.
5. RECOMMENDATIONS
5.1 Alignment of the Existing Statutes with ECCD
Prior to the ECCD Law, there were various statutes promulgated to effect the delivery of ECCD services. The problem is such laws had scopes much broader than ECCD, which mainly focused on children zero to six years old. It is suggested that explicit policies should be promulgated to develop a framework within those respective laws so that the implementation can be structured based on the specific needs of children stratified according to a rational age grouping. For instance, the law providing for the protection of children is concerned with child labor. For all practical purposes and intent, this concern may not be very relevant to ECCD. Also, the child-centered development mechanism envisioned for LCPCs and local ECCDCCs is lacking. As a consequence, there was no comprehensive set of data regarding the situation of children aged 0-6 years and their families in Calamba. Whatever available data were not presented according to age ranges and developmental stages so it was not clear which pertained to ECCD and non-ECCD.
To operationalize this, the existing ECD programs under various existing laws can be structured by concerns according to age categories. It should not be very difficult to embrace the idea that there could be health, nutrition, education and social protection concerns according to various life stages from early childhood to young adulthood. For instance, the Child 21 framework for child development should be emphasized to LGUs. This framework uses a life cycle approach in planning, thus, stratifying needs, programs/services, outputs according to age groups—Mother and the unborn child; infancy (0-less than 1); early childhood (1-6); middle childhood (7-11); and adolescence (12-17).
5.2 Establish a Sub-Committee under the BCPC
As argued earlier, the BCPC is also involved in most of the major development programs in the barangay, wherein the scopes are much broader than that of the ECCD. To avoid the problem of delineating the ECCD concerns within the mandate of the previous statutes where the BCPC is also involved, a smaller sub- committee under Barangay Committee on Child Protection can be instituted. This could still be chaired by the “kagawad” (councilor) sitting in the Barangay Health Committee.
To run parallel with the structures from the national down to the municipal level, a secretariat at the barangay level must also be created. This can be headed by the DCW. The other members could be the parent representative and the NGO representative. Two other members of the secretariat can be drawn from the
x
community at large chosen by the BCPC sub-committee on ECCD upon endorsement of the parent representative.
Finally, there is the need to reconsider the concept of voluntarism in the implementation of ECCD programs at the barangay level. It is suggested here that an explicit policy on incentive schemes should be provided in order to enhance the level of effort and commitment among the service providers.
5.3. Apply a Modified ToT
The ToT concept can be best utilized when the trainees themselves are already capable trainors. The essence is to orient the trainor-trainees the perspective on the new subject matter. If the ToT concept is applied to stakeholders who were never trainors themselves, then there are so many avenues for knowledge gaps and effectivity of knowledge transmission. It is recommended that the training should be made directly to the local stakeholders at the Barangay level. If there are logistical constraints, then capable trainors from locally based (Regional/Provincial) academic institutions and NGOs can be tapped as the direct trainors for the local service providers. If necessary, then the trainors from locally based institutions can be the recipient of a ToT for ECCD in their respective areas and must be tasked to train the ECCD service providers.
5.4 School Readiness at Entry to Grade One
The high dropout rate prevalent in Grades 1-2 in our country (Heaver and Hunt, 1995), plus the very low national achievement results of children in the early grades prompted the Bureau of Elementary Education to explore various ways to better prepare children for school. This has also been cause for the emphasis on school readiness, transition from home to school, and keeping children in school. Initially, there was the Summer Preschool Program, which aimed to develop the socialization and “readiness” skills of children aged 6.5 to 7 years entering Grade 1 in the coming school year. The entry age requirement then was 7 years. Overall, this pilot program met with mixed success. However, the drop out rate in the early grades of children who were preschoolers in the program was only 1% compared to the 15% for children who did not have the summer pre-school experience. Complementarily, in 1994-1995, the official age for entry into primary school was dropped to 6 years of age. DepEd justified this policy through a research that showed there was hardly any difference in the competencies of the 6- and 7-year- olds.
Furthermore, majority of children entered school then “at a definite disadvantage” because they have not had the opportunity to go to preschools or avail of the DCS at the least). So in a typical Grade 1 class in the public schools, majority of the students did not have prior ECE experiences and were, thus, unprepared for formal education. Hence, in order to mitigate the problem of school readiness upon entry to Grade 1, the following measures are suggested: Orientation and continuing education of DepEd teachers on ECCD, preschool education/teaching strategies and production of teaching devices are called for. District supervisors and coordinators of specialized areas reiterate the same need; Develop and implement developmentally-appropriate curriculum, learning materials and creative activities for Grade 1; The development of Standards for Learning Competencies in ECCD must consider that majority of our children do not access ECE programs prior to entering primary school (despite the delivery of DCS and of the new National Preschool Education program). Therefore, the learning competencies of the
xi
national ECCDCC sets for the 6 year olds must provide more time for them to acquire such in Grade 1. Many Grade 1 teachers are still apprehensive that the 8- week curriculum would infringe on their budget of time to work on the present Grade 1 curriculum. They often mention the “No read, no move” policy for Grade 1 children; and the total development of children, not preparation for elementary schooling alone, is the imperative of all early education programs, including Early Childhood Experiences in Grade 1.
5.5 Promote a Policy of Child Weaning at the ECE Stage
Field observations revealed that most of the parents stayed with their children during the entire session of the DCCs. As a consequence, children are unable to develop the sense on independence and confidence to do the ECE activities without the presence of their parents. This attitude hampers the smooth transition of the children’s learning process from ECE to Grade 1. It is suggested here that parent should be discouraged from staying within the premises of the Day Care Centers during session hours.
5.6 Technologically Appropriate Monitoring System
For a monitoring system to work efficiently for ECCD, there are three basic elements to be considered: the data requirements; the repository; and the system of processing and retrieval.
For the data requirements, it is critical to structure the data set by the critical age group. Again, the nutrition case can be cited to drive the point. It was established that the initial report of low malnutrition was based on a statistical report of all children between zero to six. It is argued here that aggregating children from zero to six years old would distort that true picture of the children’s nutritional status. The incidence of malnutrition among infants would be very low. This, in effect distorts the true picture by pulling the central tendency measures downwards. This is the reason why the report indicated a low incidence of malnutrition. It is suggested here that the data system should be stratified according to a more reasonable age grouping so as not to distort the general character of the population.
The other is the repository of the data. Since the crucial integration and convergence of ECCD services is at the barangay level, then the barangay ECCD committee should have a handle of the data sets at their level. Hence, a system must be instituted at the barangay level which could be designed for aggregation at the municipal, provincial, and national level.
However, an ECCD implementor must know that a typical rural barangay would be at least five years away from maintaining a computer that could be host to an ECCD monitoring system on a day-to-day basis. Further, the system would need the presence of a qualified staff with functional knowledge on basic database computer applications. A barangay should have the internal capacity to maintain a computer system. Computers made available to remote barangays would have a life-span of about six months. Hence, it is suggested that at an early stage, it may not be necessary or appropriate for a barangay to set up an electronic data system. At the barangay level, an index card system could work. The level of aggregation in electronic form can be done at the municipal level.
xii
Furthermore a monitoring system should encompass indicators to measure both performance and impact. For the former, the data capture instruments should be simple enough to allow for easy and systematic encoding, storage, processing and analysis. For the latter, the system should built-in benchmark indicators that are generated on a longitudinal perspective.
5.7 Tap parents to assist Day Care Workers
It was observed that many parents stay with their children during day care sessions. This pool of manpower resources can be tapped to assist in the day care activities. However, to be consistent with the concept of developing an independent child, the parents can be involved in specific tasks in the day care sessions on a staggered schedule so that only about two to three parents can be involved in any given day care activities.
5.8 Convergence of ECCD Services
One of the critical added values of ECCD relative to the prior ECCD laws is its mandate to affect the convergence of ECCD services. However, at this point, the concept of convergence is still not internalized. Hence, there is no convergence in the implementation of the services.
It is suggested that in the short run, there is a need for a massive reorientation of the service providers and stakeholders on the concept of convergence particularly in relation to and its difference from an integrated ECCD services. There is also a need, in the short run, to organize a referral system so that the ECCD services can converge to a certain child or better still to a specific household. In the long run, a better approach to allow for the convergence of ECCD services is to have an inventory and needs assessment at the household level so that ECCD services can be tailored to fit and converge to a specific household. Also, in facility development, convergence of services can be enhanced if a one-stop ECCD shop can be the basis for the development of ECCD facilities
5.9 Flexible Equity Policy
As with the other programs of the government, the equity of the LGU should be based on its capacity to pay. Most often, high incidence of malnutrition and infant and under-five mortality is high in municipalities belonging to 5th and 6th class municipalities, thus, these are the ones in need of assistance. For them to be able to participate there is a need to either waive or adjust the equity requirement.
5.10 Tapping Alternative Fund Conduits at the Community Level
To instill a sense of ownership to the program by the local stakeholders, there is a need to engage the community in the identification and implementation of ECCD including the “power of the purse”. However, this has to be done in a way so as not to allow for the political factors to dominate in the decision making process. The “KALAHI” experience can be replicated under ECCD, where peoples’ organizations were established and were utilized as conduits of the interventions under the program.
xiii
5. 11 Advocacy program for ECCD
There is a need to enhance the information, communication and education activities of the ECCD. This can be done through posting of signage in strategic areas in ECCD communities; development of IEC materials; and holding of slogan, logo, and essay writing contests.
5.12 Provision of Adequate and Development of Appropriate Learning Material
The ECCD law is explicit in its provision that the medium of instruction should be based on the local dialects. Further, the law stipulates that learning materials should be develop based on local situations. It is argued here that while adequacy of learning materials is necessary, it is not sufficient to address the learning constraints. The learning process can be facilitated if the learning competencies and values are embedded into materials based on local anecdotes and folklores.
5.13 Research Agenda
One of the most fundamental issues that was abstracted in the review was the apparent tension between the original guiding principle of the Day Care Center, which was to cater to the needs of the working parents vis a vis the trend in the demand of the non-working parents of day care children to use the center as the transition towards elementary education. This must be investigated systematically in order to draw more precise policy prescriptions.
xiv
TABLE OF CONTENTS
Page
1.0 INTRODUCTION 1 1.1 Objectives 1
2.0 METHODOLOGY 1 2.1 Conceptual Framework 1 2.2 Analytical Framework 2 2.3 The Case Study Sites 3 2.4 Data Collection and Analytical Techniques 3
3.0 RESULTS AND DISCUSSION 5 3.1 Situational Analysis 5 3.1.1 Nutrition 5 3.1.2 Health 9 3.1.3 Early Childhood Education 15 3.1.4 Social Protection 22
3.2 National Policies on Early Childhood Care and Development 24 3.2.1 Nutrition Policies 24 3.2.2 Health Policies 25 3.2.3 Early Childhood Education Policies 27 3.2.4 Social Protection Policies 31 3.2.5 The ECCD Law (RA 8980) 32
4.0 THE CASE STUDIES 33 4.1 Province of Zambales 33 4.1.1 Profile 33 4.1.2 ECCD Structure and Management 34 4.1.3 Accessibility/Quality of ECCD Services 37 4.1.4 Integration and Convergence 41 4.1.5 Monitoring System 41
4.2 Province of Leyte 42 4.2.1 Profile 42 4.2.2 ECCD Structure and Management 42 4.2.3 ECCD Accessibility/Quality of Services 49 4.2.4 Integration and Convergence 54 4.2.5 Monitoring System 57
xv
Number Title Page 4.3 Province of Davao Oriental 58 4.3.1 Profile 58 4.3.2 ECCD Structure and Management 59 4.3.3 Accessibility/Quality of ECCD Services 61 4.3.4 ECCD Partner 69 4.3.5 Integration and Convergence 70 4.3.6 Monitoring System 73
4.4 Province of Cagayan Valley 74 4.4.1 Profile 74 4.4.2 ECCD Structure and Management 75 4.4.3 Accessibility/Quality of ECCD Programs/Services 78 4.4.4 Integration and Convergence 81 4.4.5 Monitoring System 82 4.4.6 Facilitating and Hindering factors 83
4.5 Province of Misamis Occidental 83 4.5.1 Profile 83 4.5.2 ECCD Structure and Management 84 4.5.3 Accessibility/Quality of ECCD Services 87 4.5.4 Service Providers 88 4.5.5 Integration and Convergence 91 4.5.6 Monitoring and Evaluation 94
5.0 CONCLUSIONS 95 6.0 ISSUES 97
7.0 RECOMMENDATIONS 101
8.0 REFERENCES 106
xvi
LIST OF TABLES
Number Title Page
2.4 Key informants by LGU level: 2007 5 Population of preschool children by single age group, 3.1 Philippines: 2000-2007 (in millions) 5 Percent distribution of preschool children (0 to 5 years) by 3.1.1.1.1 nutritional status, Philippines: 1989-2005 6 Proportion of 0-5 year old children by nutritional status and by 3.1.1.1.2 age 7 3.1.1.2 Prevalence of anemia among preschool children by age group 7 Prevalence of deficient and low levels of vitamin A among 3.1.1.3 preschool children 8 3.1.1.5 Zinc deficiency by age and by gender (in percent 8 3.1.2.1 Selected health indicators, 1993 to 2006 10 Ten leading causes of child mortality (1-4 years old), number 3.1.2.2 and rate/100,000 population Philippines, 2000 10 Maternal mortality rate, Philippines: 1993 to 2006 (per 100,000 3.1.2.3.1 live births) 11 Maternal mortality by main cause, number rate per 1000 3.1.2.3.2 livebirths and percentage distribution, Philippines, 2003 11 3.1.2.4.1 Number of deaths <5 and total deaths 12 Reported cases of vaccine preventable diseases, Philippines: 3.1.2.4.2 2000 12 Mortality among immunizable diseases by age group, 3.1.2.4.3 Philippines, 2000 (Rate per 100,000 population) 13 3.1.2.4.4 Vaccination rate by type of vaccine, Philippines: 2005 & 2006 13 3.1.3.1.1 Children’s participation in various ECCD programs 15 Percentage of barangays with day care centers, Regions VI, VII 3.1.3.1.2 and XII, Philippines: 2000-2006 16 Participation rate of children aged 36-71 months, Regions VI, 3.1.3.1.3 VII and XII, Philippines: 2000-2004 16 3.1.3.3.1 Typical expenditure items for one day care center (in pesos) 19 3.1.3.3.2 Costs paid by a family with one child in public day care 19 Participation rate of children aged 0-71 months in Supervised Neighborhood Play, Regions VI, VII and XII, Philippines: 2000- 3.1.3.4 2004 21 Participation rate of children aged 0-71 months in preschool services (DepEd and Private), Regions VI, VII and XII, 3.1.3.5 Philippines: 2000-2004 24 3.2.1 List of some nutrition and related laws 32 3.2.4 Legislations related to child protection 34 4.1.4 Knowledge and attitude of service providers 41 4.2.2.4.5 Knowledge and attitudes of service providers 49 4.2.3.1 Summary of accomplishment in the two pilot areas as of 2007 49
xvii
4.2.3.2 Summary of activities included in the ECCD plan in Sta. Fe 50 OPT among preschool children and weighing results among 4.2.3.3 grade 1 pupils, Milagrosa 54 4.2.4.1 List of responsibilities of mother and father 56 4.2.4.2 Knowledge and attitudes of service providers 57 4.3.3.1 Support service delivery, Governor Generoso, Davao Oriental 62 Components of system establishment and institutionalization, 4.3.3.2 Gov.Generoso, Davao Oriental 63 Capability building for service providers and provision of 4.3.3.3 livelihood activities to beneficiaries 63 4.3.3.4 Programs for day care centers 64 4.3.3.5 Planning and management programs 64 Rehabilitation of rural health station by municipality, Davao 4.3.3.6.1 Oriental 65 4.3.3.6.2.1 Comparison between hot meal and choco milk 66 Percent change in the nutritional status of children by age, 4.3.3.6.2.2 Barangay Nangan: First quarter 2005 and 2006 (in mos.) 67 List of rehabilitated day care centers , Municipality of Governor 4.3.3.6.4 Generoso. 2006 68 Demographic profile of service providers, Barangay Nangan, 4.3.4.1 Governor Generoso: 2007 69 Knowledge, attitude and perceptions of service providers, 4.3.4.2 Barangay Nangan, Governor Generoso: 2007. 70 Service providers and those providing assistance in the delivery of services for children: Barangay Nangan, Governor 4.3.4.1 Generoso: 2007 71 Service providers and those providing assistance in the delivery of services for children: Barangay Nangan, Governor 4.3.4.2 Generoso: 2007 71 Remuneration by type of service provider, Barangay Capatan, 4.4.3.1 Tuguegarao City 80 4.4.3.2 Knowledge and attitudes of service providers 81 Report submitted by type, whom submitted and frequency by the Barangay Nutrition Scholar, Barangay Capatan, Tuguegarao 4.4.5 City 83 4.5.2.2 ECCP funds released to pilot municipalities. 86 Activities performed by the six committees of the BCPC, Siloy, 4.5.3.1 Calamba, Misamis Occidental 87 Status of the health-related service provided by the RHM, Siloy, 4.5.4.1 Calamba, Misamis Occidental 88 4.5.4.2 DCW’s tasks, Siloy, Calamba, Misamis Occidental 89 Training activities attended by the DCW’s, Siloy, Calamba, 4.5.4.3 Misamis Occidental 90 4.5.4.4 ECCD projects in Calamba 90 Services provided by the Grade 1 teacher, Siloy, Calamba, 4.5.4.5 Misamis Occidental 91 4.5.4.1.6 Reports prepared by the Grade 1 teacher 92 4.5.5.1.4 ECCD services available in Siloy 94
xviii
LIST OF FIGURES
Number Title Page
2.1 The child’s environment 2 Schematic diagram indicating the link between ECCD 2.2 services and child development. 3 2.3 Case study sites 4 3.1.2.6 Number of newborns screened, 1996-2006 14 4.3.2.3 Provincial ECCD Coordinating Committee 61 Nutritional Status of pre-school children, Barangay 4.3.3.6.2.1 Nangan: 2005 and 2006 67 Percent change in the nutritional status of children by age, Barangay Nangan, 1st quarter 2005 and 2006 (in 4.3.3.6.2.2 months) 67 KAP on children’s rights, maternal and child health and cognitive development of mother, Barangay Nangan, 4.3.4 Governor Generoso: 2007 70
xix
LIST OF ACRONYMS
AHMP Accelerated Hunger Mitigation Program APECCDO Assistant Provincial ECCD Officer BC Barangay Captain BECCDIT Barangay ECCD Implementing Team BHW Barangay Health Worker BNAP Barangay Nutrition Action Plan BNL Below normal low BNS Barangay Nutrition Scholar BNVL Below normal very low CARP Comprehensive Agrarian Reform Program COA Commission on Audit CSEZFP Cagayan Special Economic Zone and Free Port CSWO City Social Welfare Office CWC Council for the Welfare of Children DA Department of Agriculture DCC Day Care Center DCS Day Care Services DCW Day Care Worker DepEd Department of Education DILG Department of Interior and Local Government DOH Department of Health DOST Department of Science and Technology DSWD Department of Social and Welfare Development ECD Early childhood development ECE Early childhood education ECEP Early Childhood Enrichment Project EFA Education for All EPI Expanded Program of Immunization FGD Focus Group Discussion FHSIS Field Health Service Information System FNRI Food and Nutrition Institute GOT Grade One Teacher HRD human resource development IDD iodine deficiency disorder IEC information, communication and education ILO International Labor Organization IMCI Integrated Management of Childhood Illnesses IP indigenous people IRA Internal Revenue Allocation IRR Implementing Rules and Regulations IRS International Reference Standard IUD Intrauterine Device KAMPI Kapisanan ng may Kapansanan Inc. KAP knowledge, attitude and perception
xx
Local/Provincial/City/Municipal/Barangay Council for L/P/C/M/BCPC the Protection of Children LCE local chief executives LDPC Local Development Plan for Children LGC Local Government Code LGU local government unit M/BECCDCC Municipal ECCD Coordinating Council MBN Minimum Basic Needs MCPC Municipal Council for the Protection of Children MDG Millennium Development Goals MIS management information system MOA Memorandum of Agreement MPDC Municipal Planning and Development Council NBS newborn screening NDHS National Demographic and Health Survey NEDA National Economic and Development Authority NGA national government agencies NGO non-government organization NNC National Nutrition Council NNS national nutrition survey NSCB National Statistical Coordination Board NSO National Statistics Office OSY out-of-school youth Provincial/Municipal/Barangay Early Childhood Care P/M/B/ECCDC and Development Committee P/M/BHO Provincial/Municipal/Barangay Health Office P/MNAO Provincial/Municipal Nutrition Action Office P/MNO Provincial and Municipal Nutrition Office Provincial and Municipal Planning Development P/MPDO Office Provincial/Municipal Social Welfare and P/MSWDO Development Office PD Presidential Decree PECCDO Provincial ECCD Officer PES Parent Effectiveness Services PhilHealth Philippine Health Insurance PHO Provincial Health Office PHS Philippine Health Statistics PNP Philippine National Police PPAN Philippine Plan of Action on Nutrition PRA participatory rapid appraisal PTCA Parent-Teacher Community Association PTWG Provincial Technical Working Group Regional/Provincial Sub-committee for the Welfare of R/PSCWC Children RA Republic Act RHMW Rural Health Midwife
xxi
RHU Regional Health Unit SK Sangguniang Kabataan SNP Supervised Neighborhood Play SRA School Readiness Assessment SRAT School Readiness Assessment Test SSS Social Security System STAC Stimulation and Therapeutic Activity Center strengths, weaknesses, opportunities, and SWOC constraints ToT Training of Trainors TRICAP Tribal Community Association of the Philippines TWG Technical Working Group UNCRC United Nation’s Convention on the Rights of the Child United Nations Education, Scientific and Cultural UNESCO Organization United Nations International Children’s Education UNICEF Fund VAD Vitamin A deficient VAWC Violence Against Women and Children WFC World Fit for Children WFP Work and Financial Plan WHO World Health Organization
xxii EARLY CHILDHOOD CARE AND DEVELOPMENT (ECCD) POLICY REVIEW IN THE PHILIPPINES
DRAFT FINAL REPORT
1.0 INTRODUCTION
The United Nations Education, Scientific and Cultural Organization (UNESCO) and the United Nations International Children’s Education Fund (UNICEF) aim to support Asia- Pacific countries in meeting the first goal of Education for All (EFA) through an assessment of the state of policy and implementation of early childhood development. Hence, said organizations launched, in September 2006, the Regional Early Childhood Care and Development Policy Review Project across nine countries including the Philippines.
1.1 Objectives
In general, the review process aimed to support and assist the Philippine Government in meeting the goals of the ECCD Program by identifying, documenting, and sharing good practices as well as constraints in the policy development and implementation of early childhood care and development, which are aligned with other national sectoral plans as well as with the international commitments to the Millennium Development Goals (MDG), World Fit for Children (WFC), and Education for All.
Specifically, the objectives of the review included the following:
to determine the level of access to the basic ECCD services; to identify the factors affecting the level of access; to assess the quality of the ECCD services; to characterize the nature of integration and convergence of ECCD services; and to assess the feedback mechanisms and structure established for the program.
2.0 METHODOLOGY
2.1 Conceptual Framework
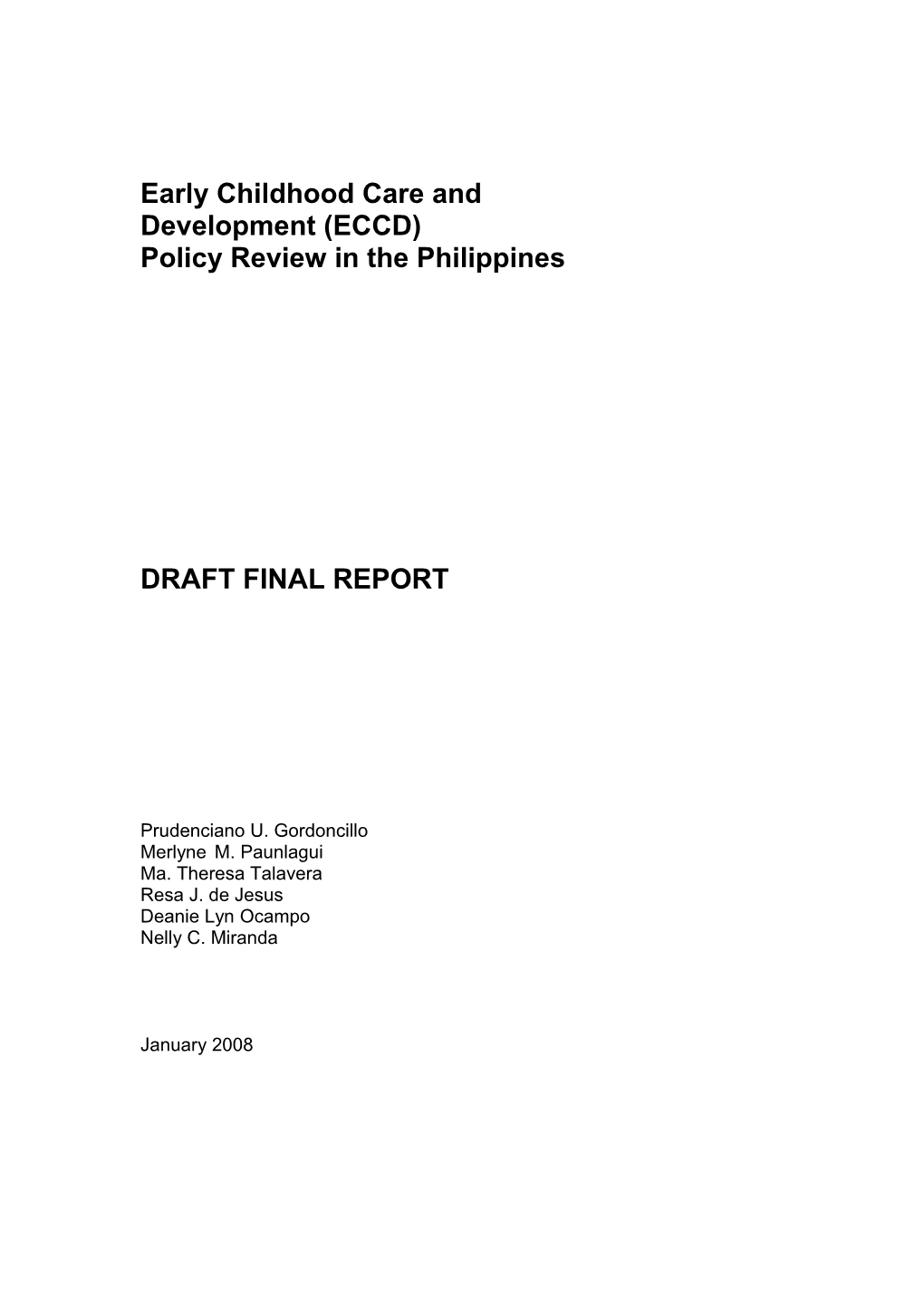
The conceptual framework for this Program review was drawn from the original ECCD framework adapted from Brofenbrenner (1988) in the baseline survey as well as in the evaluation study as outlined in Figure 2.1.
To establish the review in proper perspective, it is necessary to understand the interaction among the stakeholders of the ECCD Program across various levels – from an individual perspective, household, community, local government unit (LGU) level, and up to the national level. These interactions that influence the overall development of the child involves resources, events, values, and communications. The review will also be guided by the principle that intervention in early childhood development should be holistic and that the critical role of the primary care givers and the parents should be considered. Further, ECCD interventions should provide for the
inclusion of vulnerable children, smooth transition from home-to-center-to-school, and gender sensitivity.
National Institutions
Interaction Communication Church, School, Health Care
Community
Family
Value System People Child
Household
Immediate Community
Institutional community Physical Activites (Space, Ameneties) Socio-Political Framework (Events,Routine Cycles) FigureFigure 1. The2.1 Child’s The Environment child’s environment
Source: International Development Research Center, 1988.
2.2 Analytical Framework
The specific areas of concerns or themes that the review process focused on include access, quality and the level of integration, and convergence of ECCD services. In terms of access, the following specific questions were addressed: What were the causes of low participation?; Was it a problem of availability, accessibility, affordability, awareness, or attitudinal?; and Who were the disadvantaged and the advantaged and how were the gaps generated?
The process of assessing the quality of service focused on the appropriateness of the intervention, content, standards, the mode of delivery, and the capacity and level of commitment among the service providers. Similarly, the review looked at the adequacy and appropriateness of ECCD infrastructures, facilities, and material support. It also assessed the sensitivity of the services to the cultural and social character of the communities.
One of the guiding principles advocated for an ECCD intervention is that the approach should be holistic and integrated. Hence, the fundamental question addressed in the review process was in terms of the mode and extent of integration of the various ECCD services.
There were also cross-cutting issues that the review dealt with, particularly in terms of resources, governance and effectiveness of the delivery system. Source and mode of financing were also critical. In most developing countries, allocations of resources are often guided by political interest. Thus, there is a need to address the issues concerning the mechanisms instituted to insulate the program from political interventions as well as
2
the structures established to define and delineate accountabilities. At the current phase of ECCD implementation in the Philippines, effectiveness was assessed through established mechanisms to operationalize the monitoring and evaluation component of the program.
The review was guided by a framework of analysis as shown in the schematic diagram Figure 2.2. It is argued here that to assess the mode and extent of integration of ECCD services, one need to look at the household as the basic and focal unit. In a status quo, the state of the child development is determined primarily by the resources available at the household level. However, attitudes and values also play a critical role in the It is the interplay of these factors that basically determine the development of the child.
Figure 2.2 Schematic diagram indicating the link between ECCD services and child development.
Child Survival, Growth and Development
Therefore, any attempt to intervene towards the development of children in terms of health and nutrition, psycho-social and early education as well as social protection in an integrative manner will have to be focused at the household level, in general, and to the child, in particular.
2.3 The Case Study Sites
The cases were conducted in five provinces where the ECCD were already implemented. Two study sites each were selected from Luzon and Mindanao and one from the Visayas (Figure 2.3). The provinces of Cagayan and Zambales represented the island of Luzon; Leyte for Visayas; and Davao Oriental and Misamis Occidental for Mindanao.
2.4 Data Collection and Analytical Techniques
The review used both qualitative and quantitative data. The process included three phases, namely: secondary data review, primary data collection, and analysis.
3
The secondary data included existing policies promulgated to effect child development, and a situational analysis based on published reports and statistical bulletins. The analysis situated the country’s current ECCD status in relation to the regional patterns and in relation to the country’s commitment to the MDG, WFC and EFA.
Primary data were collected through participatory rapid appraisal (PRA). This technique of data collection required the establishment of experts from various disciplines who conducted field visits within a period of four to five days. The team was composed of experts from the fields of health, nutrition, child development/early childhood education, development economics, sociology and social protection.
Bgy. Capatan, Tuguegarao City, Cagayan Valley Bgy. Porac, Botolan. Zambales
Bgy. Milagrosa, Sta. Fe, Leyte
Bgy. Siloy, Calamba, Misamis Occidental Nangan, Governor Generoso, Davao Oriental
Figure 2.3 Case study sites
In every field visit, courtesy calls were made with the Provincial Social Welfare Office, Office of the Governor, and Office of the Mayor. Focus group discussions (FGDs) were conducted with the Provincial Early Childhood Care and Development Committee (PECCDC), Municipal Early Childhood Care and Development Committee (MECCDC), and the Barangay Early Childhood Care and Development Committee (BECCDC). In addition, the following served as key informants (Table 2.4)
Secondary data were collected from the Provincial and Municipal Planning Development Office (P/MPDO), Provincial and Municipal Nutrition Office (P/MNO), Provincial/Municipal Social Welfare and Development Office (P/MSWDO) and Barangay. The secondary data provided relevant information about the province, municipality, and barangay.
4
Table 2.4. Key informants by LGU level: 2007 Location Key Informant Province Provincial ECCD Action Officer Municipality Municipal ECCD Action Officer Municipal Nutrition Action Officer Social Development Worker Barangay Rural Health Midwife (RHMW) stationed/assigned in Barangay Grade One Teacher (GOT) Kinder/Pre-elementary Teacher 3.0 RESULTS AND DISCUSSION Day Care Worker (DCW)
3.0 RESULTS AND DISCUSSION
3.1 Situational Analysis
This section reviews the health, nutrition, early childhood education (ECE), and social protection situation of the ECCD children in the country. Included also are the policies, programs and projects implemented by the government to address the health, nutrition, early childhood education, and social protection to address the challenges affecting preschool children.
In 2000, the population of preschool children was 13,557,000, representing 18 percent of the total population of the Philippines. It was projected that by 2007, the number will increase to 16,052,000 or 2,495,000 preschool children more than in 2000 (Table 3.1).
Table 3.1. Population of preschool children by single age group, Philippines: 2000-2007 (in millions) Age 2000 2001 2002 2003 2004 2005 2006 2007 0 1,876 1,927 1,972 2,018 2,066 2,114 2,163 2,214 1 1,876 1,969 2,015 2,062 2,110 2,159 2,210 2,262 2 1,944 1,998 2,045 2,092 2,141 2,192 2,243 2,295 3 1,962 2,016 2,063 2,112 2,161 2,212 2,263 2,316 4 1,970 2,024 2,072 2,120 2,170 2,221 2,273 2,326 5 1,969 2,023 2,071 2,119 2,169 2,219 2,271 2,325 6 1,960 2,014 2,061 2,109 2,159 2,209 2,261 2,314 Total 13,557 13,971 14,299 14,632 14,976 15,326 15,684 16,052 Source: NSO
3.1.1 Nutrition
3.1.1.1 Protein-energy Malnutrition
The average prevalence of underweight, under height, and thin in the eight surveys conducted were 30.4 percent, 33.4 percent and 5.7 percent, respectively. The incidence of underweight and under height preschool children showed a declining trend (Table
5
3.1.1.1.1). The percent of underweight increased from 1993 to 1996 by 0.9 percentage points; and from 1996 to 1998 by 1.2 percentage points. However, the figure for underweights consistently decreased. The prevalence for stunting showed a more consistent declining trend except in years 1993 and 1996 when a very small increase was noted.
Table 3.1.1.1.1 Percent distribution of preschool children (0 to 5 years) by nutritional status, Philippines: 1989-2005
1989- 1992 1993 1996 1998 2001 2003 2005 Remarks 90 Underweight 34.5 34.0 29.9 30.8 32.0 30.6 26.9 24.6 High
Stunting 39.9 36.8 34.3 34.5 34.0 31.4 29.9 26.3 High except in 2003 & 2005 Wasting 5.0 6.6 6.7 5.2 6.0 6.3 5.3 4.8 Low
Sources: DOST-FNRI NNS, 1993; 1998; 2003; Regional Updating of the Nutritional Status of Children, 1989/1990; 1992; 1996; 2001; 2005
The study of Pedro et al. (2006) estimated that reducing the proportion of underweight children to 17.25 percent by 2015 is difficult to achieve given that the average annual reduction was only 0.58 percent. However, the trends are expected to improve when there would be improvements in food intake, health, and water and sanitation. The prevalence of wasting is also expected to decrease but not stunting. In fact, the incidence of underweight will tend to decrease at a faster rate than that of stunting (Kennedy et al. 2006).
Table 3.1.1.1.2 shows the decreasing trend in the occurrence of underweight, under height, and thinness by age group from 1998 to 2005 for all indicators in all age groups. However, as the children grew older, the prevalence of underweight, under height, and wasting more than doubled. For instance, the incidence of underweight among infants increased from 10.2 percent to 28.9 percent; under height from 5.4 percent to 25.4 percent; and wasting from 4.5 percent to 12.0 percent. This suggests that the period between zero to one year of age is the critical period, a phase where under nutrition and growth faltering occur. Then, as the children grow older, a large number of them continue to suffer from under nutrition.
6
Table 3.1.1.1.2. Proportion of 0-5 year old children by nutritional status and by age Index/Year Age in years 0 1 2 3 4 5 Underweight 1998 12.9 38.6 37.2 34.1 34.6 32.6 2003 11.7 31.2 31.7 29.6 27.3 29.9 2005 10.2 28.9 24.7 25.6 27.7 26.3 Under height 1998 8.7 33.0 31.5 40.0 43.6 42.7 2003 8.2 25.4 31.8 37.9 36.4 38.2 2005 5.4 23.5 25.5 30.0 34.6 36.2 Wasting 1998 5.7 14.9 5.8 2.5 3.5 3.5 2003 ------2005 4.5 12.0 4.0 4.3 2.7 2.1 Sources: DOST-FNRI NNS, 1998; 2003; Regional Updating of the Nutritional Status of Children 2005
3.1.1.2 Iron Deficiency Anemia
There was an increasing trend in the prevalence of iron deficiency anemia among six months to less than one-year old children and one year to five years old from 1993 to 2003 (Table 3.1.1.2). On a per age group basis, the incidence was highest among one- year old children in both nutrition surveys at 53.2 percent and 53 percent, respectively. Moreover, the decrease in the prevalence was very low at 0.02 percent from 1998 to 2003. As the children grew older, the frequency of anemia decreased because the children were now able to eat a wider variety of iron-rich foods. The problem on anemia was attributed primarily to inadequate iron intakes (Pedro et al. 2006). Other factors included poor child feeding and weaning practices and poor compliance with iron supplementation programs (Kennedy et al. 2006). Table 3.1.1.2. Prevalence of anemia among preschool children by age group Age Prevalence/year 1993 1998 2003 6 mos to < 1 year 49.2 56.6 65.9 1 year – 5 years 25.7 29.6 29.1 1 year - 53.2 53.0 2 years - 36.9 34.8 3 years - 23.4 24.8 4 years - 20.0 18.8 5 years - 18.2 14.7 Sources: FNRI-DOST. NNS, 1993; 1998; 2003
3.1.1.3 Vitamin A deficiency
Vitamin A deficient (VAD), which has been defined as serum retinol <20 ug/dl, is considered a public health problem if it affects 15 percent of children aged six to 59 months. The prevalence of VAD had been increasing among preschool children, particularly among infants (Table 3.1.1.3). The incidence of VAD also increased by 10 percentage points from 1993 to 2003. The high prevalence of VAD among preschool children was attributed partly to the poor micronutrient status of pregnant and lactating women (Pedro et al. 2006).
7
Table 3.1.1.3. Prevalence of deficient and low 3.1.1.4 Iodine Deficiency levels of vitamin A among preschool Disorders children Age Prevalence (%) Data on the incidence of 1993 1998 2003 iodine deficiency disorder 6 mos to > 1 year 37.5 42.2 47.0 (IDD) among preschool 1 year – 5 years 35.6 37.6 39.3 children is not available. However, goiter prevalence 6 mos – 5 years 35.3 38.0 40.1 (national) had been studied in Source: DOST-FNRI. NNS, 1993, 1998, 2003 1993 and was found to be 6.7 percent among subjects 7 years old and above with the highest occurrence among pregnant females between ages 13 to 20 years old (Tuazon and Habito nd). Another parameter was used later on, which 1was urinary iodine excretion. The 2003 national nutrition survey (NNS) of the Food and Nutrition Institute (FNRI) reported a decline in the prevalence of IDD from 36 percent in 1998 to 11 percent among children 6 to 12 years. A similar trend was noted among pregnant women from 28.4 percent moderate to severe in 1998 to 18 percent in 2003. The reduction was attributed to the implementation of the Salt Iodization Program and the increasing availability and consumption of fortified processed foods (Pedro et al. 2006; Philippine Food Fortification Program nd).
3.1.1.5 Zinc Deficiency
The problem of zinc deficiency is considered as moderate given that the overall prevalence was 9.8 percent (10.6% and 9.1% for the males and females, respectively) (Table 3.1.1.5). The 4-year old children had the highest incidence of deficiency at 13.7 percent which was also considered moderately high.
Table 3.1.1.5. Zinc deficiency by age and by gender (in percent Age group/sex Male Female % deficiency 6-11 months 8.7 9.7 9.1 1 year 11.1 8.4 19.1 2 years 8.6 7.8 8.2 3 years 11.3 6.9 9.1 4 years 13.4 13.9 13.7 5 years 9.3 7.9 8.5 All children 10.6 9.1 9.8 Sources: DOST-FNRI NNS, 2003 . 3.1.1.6 Other Micronutrient Deficiencies
Deficiencies in other micronutrients were included in the fourth NNS (FNRI, 2003). The results showed that zero to six year-old children were found to manifest clinical signs suggestive of deficiencies in riboflavin, thiamin, and vitamin C. Less than 1 percent of children were found to suffer from angular stomatitis (0.7%), cheilosis (0.4%), magenta tongue (0.2%), spongy bleeding gums (2.3%) and pale conjunctiva (19.2%). Angular stomatitis, cheilosis, and magenta tongue are signs associated with riboflavin deficiency; pale conjunctiva for iron deficiency anemia, and spongy bleeding gums for vitamin C. Riboflavin deficiency was not considered prevalent because of the low percentage (Tuazon et al. 1997). In contrast, thiamin deficiency was a nutritional problem based on
8
the erythrocyte transkelolase activity where 34.4 percent of infants and preschoolers were found to be deficient.
3.1.1.7 Overweight/Obesity
The rate of recurrence of obesity remains to be significantly less than under nutrition but still needs to be addressed. While a small proportion of children are obese, the increasing trend in the rates of obesity is alarming since half of the children who are obese at six years of age are more likely to become obese in their adulthood (Pedro et al. 2006). Moreover, obesity is a risk factor for several diseases such as type 2 diabetes, coronary heart disease, hypertension and some types of cancers (WHO 1997 as cited in Kennedy et al. 2006).
3.1.1.8 Breastfeeding and Young Child Feeding Practices
Based on the results of the 2005 NNS of the DOST-FNRI, about 89 percent of mothers practiced exclusive breastfeeding with a mean duration of three months. This falls below the recommended exclusive breastfeeding for six months. On the other hand, 87 percent of children were breastfed for a mean duration of almost six months.
3.1.1.9 Food Intake and Nutrient Adequacy
The food intake and nutrient adequacy can partly explain the current poor nutritional status of preschool children. Inadequate food intake is a direct or primary cause of under nutrition. As children grow older, the amount consumed per food group increases except for milk. The mean intake of rice increases from 116 grams to 202 grams from infancy to five years old. In contrast, the mean intake of milk decreases from 726 to 59 grams. The decrease is also more significant after infancy from 726 grams among 6 to11-month old children to 355 grams among one-year old children. Starting at two years old, children are not able to consume the recommended one glass (240 grams) of milk a day.
In general, the food intake of preschool children was found to have increased from 1978 to 2003. However, in terms of adequacy, the preschool children were found to be inadequate in energy and other nutrients (iron, vitamin A and calcium) except protein. Rice, milk and milk products, fish, meat and poultry, and fruits were the major contributors to the children’s diet. The inadequate food intake contributed to the children’s poor nutritional status.
3.1.2 Health
Among all children, the under five-year old population has been recognized as most vulnerable to health problems. Healthy children become healthy adults: people who create better lives for themselves, their communities and their countries (UNICEF nd). Knowing that health status would have an impact on children’s growth and development, child health is an important public health concern.
3.1.2.1 Infant Mortality
Infant mortality was not only declining but declining faster in the more recent years. Between 1993 and 1998, infant mortality only decreased at an average of 1.58 percent per annum compared to the 6.29 percent annual reduction between 1998 and 2006. As
9
such, there is a very high probability of meeting the infant mortality rate of 19 per thousand live births in 2015 as specified in the MDG.
Table 3.1.2.1. Selected health indicators, 1993 to 2006 Indicator 1993 1998 2006 Percent Change 1993-1998 1998-2006 Infant mortality rate 38 35 24 -1.58 -6.29 Sources of Raw Data: 1998, 2003 –NDHS; 1993 – National Demographic Survey; 2006 – Family Planning Survey
In the 2003 Philippine Health Statistics (PHS), eight of the 10 leading causes of infant mortality were conditions affecting neonates or infants one month old or younger. These included neonatal infections, congenital malformations, and conditions related to events surrounding the child’s birth such as pregnancy complications and difficult deliveries. These causes accounted for 64.8 percent of the total infant deaths. This indicates that majority of deaths occur in the newborn period, emphasizing the importance of interventions and programs that address these problems. Also noteworthy was that four out of the 10 leading causes of infant mortality were infectious in nature, namely: pneumonia, neonatal sepsis, congenital pneumonia and infectious diarrhea. In spite of preventive measures and advances in medical care, infections remained to be significant contributors to infant mortality.
3.1.2.2 Under-five Mortality
UNICEF data ranked Table 3.1.2.2 Ten leading causes of child mortality (1-4 years the Philippine under- old), number and rate/100,000 population five mortality rate at Philippines, 2000 86th in the world. In Both Cause Male Female Rate* the National Sexes Demographic and 1. Pneumonia 1,540 1,341 2,881 37.76 Health Survey 2. Accidents 839 506 1,345 17.63 (NDHS) (2003), it was 3. Diarrheas and gastroenteritis 685 546 1,231 16.14 estimated at 42/1000 of presumed infectious origin live births. Mortality 4. Measles 452 425 877 11.50 rate was higher in 5. Congenital anomalies 350 337 687 9.01 rural (52/1000) compared to urban 6. Malignant Neoplasm 219 153 372 4.88 (30/1000) areas. 7. Meningitis 201 155 356 4.67 8. Septicemia 173 173 346 4.54 Under-five mortality 9. Chronic obstructive pulmonary 174 164 338 4.43 rate in the Philippines disease and allied conditions declined from 90 per 10. Other protein-calorie malnutrition 175 159 334 4.38 1000 live births in *rate per 100,000 population of corresponding age-group 1970 down to 62 in Source: PHS 2000, DOH 1990 and to 33 in 2005. The rate of reduction was higher from 1990-2005 with an average annual rate of 4.2 percent compared to the period 1970-1990 with an average annual rate of 1.9. Nonetheless, the MDG of 26.7 per 1000 livebirths in 2015 is highly attainable (Canlas nd).
10
In 2000, about 70 percent of deaths in one to four-year age group were due to pneumonia, diarrhea, measles, meningitis, and malnutrition (Table 3.1.2.2).
3.1.2.3 Maternal Health Indicators
One indicator that is used to reflect the health of pregnant women is the maternal mortality rate. Maternal mortality was declining, from 209 per 100,000 live births in 1993 to 162 in 2006. The decline, however, was sharper between 1993 and 1998 than between 1998 and 2006 (Table 3.1.2.3.1). In fact, the slowing down in the reduction of maternal mortality cast doubt on the ability of the government to meet the MDG of reducing maternal mortality rate to 52 per 100,000 live births in 2015.
Table 3.1.2.3.1 Maternal mortality rate, Philippines: 1993 to 2006 (per 100,000 live births) Percent Change Indicator 1993 1998 2006 1993-1998 1998-2006 Maternal 209 172 162 -3.54 -1.16 Mortality Ratio Sources of Raw Data: 1998, 2003- NDHS; 1993 – NDHS; 2006 – Family Planning Survey
The most common causes of maternal death were hypertensive complications and hemorrhage accounting for 43.7 percent of all maternal deaths (Table 3.1.2.3.2). The causes of maternal deaths remained almost the same through the years.
Table 3.1.2.3.2. Maternal mortality by main cause, number rate per 1000 livebirths and percentage distribution, Philippines, 2003 Cause Number Rate Percent Other Complications related to pregnancy during 811 0.5 45.1 labor, delivery and puerperium Hypertension complicating pregnancy, 479 0.3 26.6 childbirth and puerperium Postpartum hemorrhage 319 0.2 17.7 Pregnancy with abortive outcome 189 0.1 10.5
*Percent share to total number of maternal death Last Update: January 11, 2007, www.doh.gov.ph/kp/statistics/maternal_deaths 3.1.2.4 Expanded Program of Immunization
Infections are significant contributors to the morbidity and mortality in children. Fortunately, vaccines have been developed to protect individuals against these infections. However, in spite of the availability of this preventive measure, significant numbers of vaccine preventable diseases are still being reported.
In the Philippines, the incidence of diseases for which vaccines were part of the routine immunization schedule decreased remarkably (Table 3.1.2.4.2). The reported cases of preventable diseases were all below 50 except for tetanus with reported cases of 161 in 2006. In fact, there were no reported cases of neonatal tetanus in 2006 and only nine cases for pertussis.
11
Remarkably, most cases for most diseases were reduced in 1995, particularly for pertussis and polio whose number of reported cases dropped by around 90 percent between 1990 and 1995.
In spite of the decrease in the incidence of these diseases, they persist to be significant causes of deaths among children. Year 2000 health statistics showed that the highest number of deaths were associated with measles and tetanus (Table Table 3.1.2.4.1 Number of deaths <5 and 3.1.2.4.3). total deaths Diseases Deaths Total Great efforts have been made to <5 years deaths increase the immunization rate. A old (000) child is said to be fully immunized (000) Vaccination for which vaccination is part of most if he or she has received BCG, national immunization schedule three doses of polio and DPT, and measles vaccinations. In the 2003 Measles 540 610 demographic survey, the HiB 386 386 completion rate was only 70 Pertussis 294 294 percent with higher completion Tetanus 198 213 rate in urban areas (74%) than in Yellow fever 15 30 rural areas (65%). Diptheria 4 5 Polio <1 <1 Hepatitis B <1 600 Vaccine for which a licensed vaccine is available Nationwide coverage with individual vaccines was around 80 Japanese encephalitis 5 14 percent in 2005 and 2006. Meningoccocal 10 26 However, there was a slight Rotavirus 402 449 decrease in nearly all types of Pneumococcal 716 1,612 vaccine from 2005 to 2006. For Total 10,468 57,029 instance, immunization rate for BCG slightly went down from 82.4 percent in 2005 to 81.70 percent in 2006. By contrast, the immunization rate for Hepatitis B almost doubled during the same period (Table 3.1.2.3.4). As such, immunization rate for all types of vaccine hovered at about 80 percent in 2006. Full immunization among 9 to11-month old children this year was reported to be 76.7 percent for the whole Philippines; across regions, the immunization rate varied by location and type of vaccine.
Table 3.1.2.4.2. Reported cases of vaccine preventable diseases, Philippines: 2000 Diseases 1980 1985 1990 1995 2000 2005 2006 Measles 1,910 1,669 921 173 88 118 47 Pertussis 26,765 62,959 42,938 3,913 7,120 118 9 Polio * 19,844 19,628 4,135 22 23 20 41 Tetanus 432 557 85 40 0 0 0 (neonatal) Tetanus (total) 1,506 1,244 291 288 281 177 161
12
Table 3.1.2.4.3 Mortality among immunizable diseases by age group, Philippines, 2000 (Rate per 100,000 population) Cause Under 1 1-4 5-9 10-14 Measles (B05) 20.9 11.5 1.1 0.4 Tetanus (A35) 7.4 0.1 0.5 0.6 Tuberculosis of Meninges (A17) 1.2 1.5 0.8 0.7 Diphtheria (A36) 0.3 0.2 0.1 0.0 Other Tuberculosis (A14-A18;B90) 1.8 0.9 0.7 1.3 Acute Poliomyelitis, including late 0.0 0.0 0.1 0.0 effects (A80) Source: PHS 2000, DOH file:///G:/eccd/health%20situation/immunizable.htm
Table 3.1.2.4.4 Vaccination rate by type of vaccine, Philippines: 2005 & 2006 Diseases 2005 2006 BCG 82.4 81.7 DPT1 83.3 81.9 DPT2 81.6 80.7 DPT3 81.0 80.0 OPV1 83.6 81.8 OPV2 82.5 80.6 OPV3 81.9 79.9 Hepa B1 48.9 78.8 Hepa B2 45.1 74.0 Hepa B3 42.9 72.9 Measles 84.1 83.2
3.1.2.5 Integrated Management of Childhood Illnesses
The under-five year old mortality rate in developing countries has remained to be high. According to World Health Organization, seven out of the 10 under-five deaths are due to five preventable and treatable diseases, namely: pneumonia, diarrhea, measles, malaria, and malnutrition. Inadequate diagnostic services, equipment and drugs are among the factors identified to have contributed to these deaths. The UNICEF has addressed this problem by developing the Integrated Management of Childhood Illnesses (IMCI) strategy. The Philippines, together with Vietnam, were the first countries in the western pacific to adopt IMCI.
IMCI is an integrated approach that focuses on the well-being of the child. It includes both preventive and curative elements that are implemented by health facilities with the participation of families and communities. Instead of the conventional single disease approach to diagnosis, IMCI combines the factors that contribute to increased risk in children. This approach ensures that all conditions present in the child will be diagnosed and correspondingly treated. The IMCI guideline provides a stepwise approach to the management of childhood illnesses. It also emphasizes preventive measures and good nutrition.
13
Integrated in the IMCI approach are the protocols for control of diarrheal diseases and acute respiratory infection. Nationwide, 14 percent of diarrhea cases in children aged 0 to 59 months were given oral rehydrating solution (ORS). 3.1.2.6 Newborn Screening
Republic Act (RA) No. 9288 or the Newborn Screening Act of 2004 promulgates a comprehensive policy and a national system for ensuring newborn screening. The act ensures that every baby born in the Philippines is offered the opportunity to undergo newborn screening (NBS). The screening system in the country offers early detection of five diseases, namely: G6PD deficiency, congenital hypothyroidism, phenylketonuria, galactosemia, and congenital adrenal hyperplasia. When left untreated, these conditions may lead to mental retardation and even death. However, early detection and treatment can save the infant from these complications.
NBS in the Philippines started through the initiative of two pediatricians: Dr. Carmelita Domingo, an endocrinologist and Dr. Carmencita Padilla, a geneticist. In 1991, they requested the Department of Health (DOH) to include NBS in routine newborn care. They headed the lobby in the congress and senate for the approval of the NBS bill. It was only in 2004 that the NBS Act was passed. Since then, there was a dramatic increase in the number of NBS facility nationwide.
The number of newborns screened increased steadily from 11,992 during the initial introduction of NBS to 66,784 in 2003 (Figure 3.1.2.6). It increased exponentially when the NBS Act was passed from 88,938 in 2004 to 175,694 in 2006. However, this staggering number only corresponds to 10.5 percent of all newborns.
Number of New borns Screened
200,000 175,694
150,000 126,815
100,000 88,938 60,269 66,784 40,888 46,535 32,301 33,432 50,000 24,572 11,992 0 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 Figure 3.1.2.6 Number of newborns screened, 1996-2006
3.1.2.7 Safe Motherhood
Safe motherhood is a program that aims to address the causes of maternal mortality. As most of these causes overlap with the causes of stillbirths, neonatal mortality, and neonatal morbidity, a reduction in these health indicators can also be expected. There are four basic components to a Safe Motherhood Program, namely: family planning, antenatal care, clean and safe delivery, and essential obstetric care.
Family planning ensures that parents have the information and services to plan the timing, spacing, and number of pregnancies. In the 2006, Field Health Service Information System (FHSIS) report, there were 4.7 million current users of family planning method. The most common method used was the pills (39.0%) followed by injectables (14.6%), and IUD (13.1%). Among the new acceptors of the family planning,
14
the most common methods used were the LAM (51.8%), pills (21.1%), and injectables (12.9%).
Antenatal care by early identification and appropriate treatment is important to prevent complications of pregnancy. Pregnant mothers are also advised about breastfeeding and tetanus toxoid injection. In 2003, among the surveyed women who had a live birth in the five-year period before the survey, 62 percent of pregnant women had three or more prenatal visits while 6 percent had no prenatal check up. Thirty-seven percent received two or more doses of tetanus toxoid. In the 2006 FHSIS Report, the percentage of pregnant women who had three or more prenatal check up was slightly lower at 59.1 percent. On the other hand, the vaccination rate with two or more doses of tetanus toxoid increased to 59 percent in 2006. Clean and safe delivery component of safe motherhood ensures that birth attendants have the knowledge, skills, and equipment needed for safe and clean delivery. It also includes the provision of post-partum care to mothers. In the 2003 survey, only 38 percent delivered in a health facility while the rest delivered at home. A total of 60 percent were assisted by a trained professional, either doctor, nurse, or midwife. Meanwhile, 69 percent had at least one postpartum follow-up.
3.1.3 Early Childhood Education (ECE)
3.1.3.1 Day Care Program
A country case study by the Department of Education (DepEd) and Department of Social and Welfare Development (DSWD) in 2002 cited by UNESCO (2004) reported three types of early childhood education program: day care center (DCC), preschool (public and private), and ECE for Grade 1. The most numerous are the DCCs with 32,787 (Table 3.1.3.1.1). The number of public preschool was four times less than the number of DCC while the private DCC was even lower at a little over 5,000.
The ECE was largely provided by the government. In terms of enrolment, the ECE for Grade 1 had the most number of enrollees at 2,474,009 which was almost twice the number of day care pupils at 1,526,023. The share of the private ECE providers was a mere 8 percent of the total enrolment.
In terms of the target group, the DepEd public preschool was the only ECE which attended to single year age group. On the other hand, the other ECE programs were for three to five years and six to seven years old (Table 3.1.3.1.1.).
15
Table 3.1.3.1.1 Children’s participation in various ECCD programs Type Number of Enrolment Age group served schools/centers/classes Day care center 32,787 1,526,023 3-5 years NGO’s community- - 30,000 3-5 years based preschools DepEd public 7,447 349,653 5 years preschools Private preschools 5,064 297,880 3-5 years ECE for Grade1 All Grade 1 classes 2,472,009 6-7 years Source: DepEd, DSWD. 2002. ECCD Indicators: A country case study, Consultative Group on ECCD as cited in UNESCO 2004
The total number of DCC, 32,787, is still short by 9, 2008 as provided for in RA 6972 because as of December 2006, there, are already 41,995 barangays in the Philippines. It also appears that not all DCCs have assigned day care workers (DCWs). Of the 6,697 DCCs, there were only 6,039 DCWs. This means that 10 percent of the centers were either just structures and do not have any day care class or a DCW handles more than one DCC. The study did not offer any explanation.
The shortage of DCCs was less pronounced in the study areas covered under the early childhood development (ECD) study (ECDP 2005) wherein 88 percent of the 7,491 barangays had DCCs. However, disparity was noted occurs in the three regions (Table 3.1.3.1.2). Among the regions, Region VI had the highest percentage of barangays with DCC from 2001 to 2006. On the other hand, Region XII had consistently been at the bottom of the list since 2000. However, it is worth noting the increase in the number of barangays having DCC in Region XII. From a little over half (53.6%) in 2000, the proportion of barangays with day care had consistently increased to about three-fourths in 2004.
Table 3.1.3.1.2. Percentage of barangays with day care centers, Regions VI, VII and XII, Philippines: 2000-2006 Region 2000 2001 2002 2003 2004 VI 77.8 82.8 84.1 86.6 90.9 VII 84.1 91.1 90.9 90.6 90.9 XII 53.6 61.9 68.6 72.4 73.6 Total 76.0 82.6 83.8 85.6 88.1 Source: Early Childhood Development Project. 2005.
Another observation was the ability of Region VI to be at par with Region VII in 2004 despite the fact that the former had slightly lower percentage of barangays with DCCs in 2000. By 2004, both regions had 91 percent of the barangays in both regions had DCCs.
The ECD study found that at best, participation rate of children aged 36 to 71 months was less than half (48%) in 2004 for all the three regions (ECDP 2005) (Table 3.1.3.1.3). When disaggregated by region, participation rate appeared to keep on increasing for the
16
three regions but the increase was faster in Regions VI and XII. For instance, participation rate in Region VI increased from 32.4 percent in 2000 to 52.6 percent in 2004. Surprisingly, the participation rate in Region VII also increased, but very slow when compared with the progress of the other two regions, (from 35.7 in 2000 to 38.4 percent in 2004). Table 3.1.3.1.3. Participation rate of children aged 36-71 months, Regions VI, VII and XII, Philippines: 2000-2004 Region 2000 2001 2002 2003 2004 VI 32.4 42.2 46.9 48.9 52.6 VII 35.7 35.6 35.3 36.1 38.4 XII 37.6 41.9 44.6 44.0 51.4 Total 34.4 40.0 42.8 43.8 48.0 Source: Early Childhood Development Project. 2005
The ECDP study also reported that the 48 percent attendance for the three regions was 4.20 percentage points higher than the 2003 attendance. The ECDP study attributed the increase in participation rate to: 1) trained DCWs in 41 percent of the LGUs in the three regions, 2) upgraded DCCs, 3) construction of new DCCs, 4) additional DCWs, and 5) support extended by the LGUs and non-government organizations (NGOs). The achievements could be further enhanced by addressing the following concerns: 1) attitudinal problems of parents such as children being too young to attend day care, and 2) pre-occupied parents with livelihood activities who are constrained to bring their children to day care.
The study of Gordoncillo et al. (2006) included access to early education among indigenous people (IP) children. The predominant trend in enrollment among them was lower when compared with the national average, although there were some noticeable improvements. In Regions VI, VII and XII, participation rates were found to be 29.8 percent, 11.1 percent and 16.9 percent, respectively in 2001-2002. In 2004-2005, such values increased to 34.5 percent, 33.0 percent, and 31.6 percent, respectively. However, these figures were still way below the national level.
The low level of enrollment in a learning center for children zero to six years old was further compounded by cases of dropping out, which even escalated for all the regions in 2005. Before 2001, incidences of dropping out for Regions VI, VII and XII were 6.3 percent, 1.1 percent, and 2.5 percent, respectively (Gordoncillo et al. 2006). In 2005, these values swelled to 21.8 percent, 5.5 percent, and 8.4 percent for Regions VI, VII and XII, respectively.
A summary of the UNESCO report reveals the following characteristics of the day care program in the Philippines: 1) there are more community-based day care programs in the urban than in the rural areas; 2) the existing day care centers are insufficient to accommodate the large number of three to five years old children, particularly in the urban areas where the number of preschoolers ranged from 35 to 60 per class. Using the figures in Table 3.1.3.1.1, the average class day care class is 46. This can be reduced to 23 if there will be two shifts: one in the morning and one in the afternoon. This number is close to 27, the average number of children found in a study evaluating the impact of the early childhood development in Regions VI, VII and XII and VIII (Gordoncillo et al. 2006); and 3) Day care class is usually smaller in rural areas than in the urban areas for several reasons including lack of awareness and appreciation among
17
parents of the importance of ECE, limited finances for the tuition, and location of the day care center.
3.1.3.2 Day Care Services (DCS)
The main task of day care workers is to provide psycho-social development and early education services like supervised play and group activities (arts and crafts, music and movement, story telling), childcare for personal hygiene, supplemental feeding, health and nutrition education, learning experiences for early literacy and mathematics, and socialization experiences to support social and emotional development. As a result, more than half of the time of the DCW is spent with students. The DCW is also tasked to conduct routine growth monitoring, and health protection for enrolled children and for their parents like immunization and feeding programs. The DCW is also required to submit monthly and quarterly reports.
A DCW works for an average of five hours and a half per day, three hours of which were spent with the students (Gordoncillo et al. 2006). Thus, there still remained two hours for other activities like talking to parents, preparing reports, and conducting home visits for children enrolled in the day care center. The DCW also conducts classes for parents. There was a marked increase in the proportion of DCWs holding classes for parents between 2001 and 2005, after the implementation of the ECD program.
3.1.3.3 Day Care Workers
There is no national data on the number and profile of day care workers. Thus, only research studies are the main sources of information for the DCWs. Again, using the UNESCO study, the service providers: 1) are mostly recruited from the community to conform with the provision of the law that these providers should live near the center, (2) majority are between the ages of 30 to 40 years, (3) mostly are over qualified, (4) have no work experience, and (5) are committed public servants.
Based on the special ECCD projects and surveys, it was found that majority (44%) of DCWs were between the ages of 30 to 40; 38 percent were between 20 to 30 years old; and 8 percent were between the age 40 to 50 years. A similar finding was presented in an ECD study (2004) where the average age of a DCW was computed at 39 years old.
Majority (62.5%) of the day care workers were college undergraduates, college graduates (16%) and high school graduates (22%) – the educational requirement for DCWs. Gordoncillo et. al (2005) reported, however that there were DCWs who have not completed their secondary education.
In terms of experience, only 8 percent had some experience of working with children while 30 percent had some form of work experience but not related to children. Less than 30 percent had participated in some of form of in-service training meaning that they learned to work with children on the job. Referring to the study of Gordoncillo et al., (2005), the percentage of day care workers in the non-ECD areas who had attended training related to their work was 35 percent compared to the 88 percent of those residing in the ECD areas.
The length of service of DCWs ranged from less than a year to more than10 years. Twenty-six percent had experience working with children for six to 10 years; 19.7 percent for two to three years; 13 percent for more than 10 years; and 9 percent for only one year.
18
On the average, a DCW receives a monthly salary of PhP3,000. This is much higher than the average honorarium received by a DCW in a non-ECD area while it was almost at par with those in the ECD barangays. However, there are LGUs who are trying to increase their honorarium as in Naga and Zamboanga where a resolution was passed to cover the premiums for the Social Security System (SSS) and Philippine Health Insurance (PhilHealth) (City of Naga 2005, Zamboanga City 2007).
As will be discussed later, there are barangays without a DCC. Perhaps the explanation could be in the cost involved in operating a DCC. For instance, when conducting a feeding program, the cost is very high but in most cases, feeding is only served once or twice a year. If that is the case, the payment of honorarium of about PhP36,000 makes the most expense (Table 3.1.3.3.1).
Table 3.1.3.3.1. Typical expenditure items for one day care center (in pesos) Item Monthly Annual Honorarium of day care worker 3,000 36,000 Repair and maintenance 2,000 20,000 Supplies and materials 1,000 10,000 Feeding (PhP5/child/20 days) 6,000 50,000 X 60 children (average number of children at center) 12,000 126,000 Cost per child 200 2,000 Source: Department of Education and Culture, DSWD. 2002. ECCD Indicators: A country case study, Consultative Group on ECCD as cited in UNESCO 2004.
One reason for smaller class size in the rural area is the cost of attending a day care. UNESCO estimated that a family spends an average of PhP365 per month or a total of PhP2,850 pesos (Table 3.1.3.3.2).
Table 3.1.3.3.2. Costs paid by a family with one child in public day care Item Monthly Annual Registration fee 5 50 Participation fee 50 500 Daily allowance (PhP10/child/day) 200 2,000 Clothing (uniform) 100 300 Total* 355 2,850 *At an average of PhP200 daily wage or an annual income of PhP48,000, the total cost per child roughly represents 6 percent of the total household family income. Source: Department of Education and Culture, Department of Social Development. 2002. ECCD Indicators: A country case study, Consultative Group on ECCD as cited in UNESCO 2004.
3.1.3.4 Supervised Neighborhood Play
Delos Angeles-Bautista (2004) considered Supervised Neighborhood Play (SNP) as a less widespread but very promising form of ECE which was introduced under the ECCD.
19
SNP is a component of the Parent Effectiveness Services (PES) where play groups are convened in a designated home from one to five times a week. It was organized as a way of building on informal peer groups to develop stimulating settings for socialization and early learning.
The participation rate of children aged 0 to 71 months in SNP for Regions VI, VII and XII was also covered in the report of the ECD Project (2005). The participation rates of these children in the SNP were all lower for the three regions when compared with the participation rates in the day care center despite the increasing pattern between 2000 to 2004 (Table 3.1.3.4). Among the regions, Region XII had the lowest participation rate of 5 percent in SNP while Region VI had the highest participation rate of 28.2 percent in 2004
Table 3.1.3.4. Participation rate of children aged 0-71 months in Supervised Neighborhood Play, Regions VI, VII and XII, Philippines: 2000-2004 Region 2000 2001 2002 2003 2004 VI 2.0 6.4 8.2 17.7 28.2 VII 0.9 1.8 7.9 6.9 14.1 XII 0.6 0.7 0.5 2.8 6.0 Total 1.2 3.2 5.0 9.9 16.7 Source: ECDP, 2005
3.1.3.5 Preschools, Kindergartens and Nursery Classes
Pre-elementary classes in the public schools were established by the Bureau of Public Schools in 1971. The Education for all 2000 Assessment Country Report for the Philippines (UNESCO no date) grouped the preschool education programs into: DECS preschool program, community-based preschools, Pre-school Service Contracting early childhood, and early childhood experiences for Grade I.
First, is the program of DECS for pre-school was launched in 1993. This was initially implemented in the 20 priority divisions for Countryside Development Programmes. It aims to provide 5-year-old children in the disadvantaged areas the stimulating experiences required to develop their social, motor and readiness skills, so that they would be prepared for socialization before starting Grade I work.
Second is the Community-Based Preschools was initially launched in 1995, although the as early as 1971, DECS had already issued a policy document encouraging the school divisions to establish public preschool classes whenever possible. In March 1995, DECS further affirmed the importance of pre-schooling but also stated that preschools should be developed by the community to provide early childhood development experiences for 5-year old children before they enter Grade 1. Thus, the concept of community-based non-profit preschools, to be established through a collective partnership that includes DECS, NGOs and LGUs is being promoted.
Another pre-school initiative of the DECs is the pre-school Service Contracting This Pre- school Service Contracting Scheme as an alternative delivery system was launched in 1997 when pre-school classes were organised in the 5th and 6th class municipalities, urban poor and resettlement areas (for those affected by natural calamities and armed
20
conflict). Service providers are NGOs, private schools, LGUs and PTCAs. The general arrangement is that DECS will pay P250 per child per month for 6 months while the service providers will organise classes with 20-25 pupils per class as well as provide the salary of qualified teachers, school/classroom facilities, adequate instructional materials and basic school supplies. Funding comes from the DECS regular budget supplemented by the Bases Conversion Development Authority (BCDA) from funds raised through the sale of military camps (UNESCO nd). As of 2007, there were 714 permanent pre-school teachers under DepEd. This number will increase to 835 in 2008 as additional 121 new items have been approved.
Similar with the day care service, the primary aim of preschool is to teach young children. This program was launched in 1993 and initially implemented in the 20 priority divisions for Countryside Development Programmes. It aims to provide 5-year-old children in the disadvantaged areas the stimulating experiences required to develop their social, motor and readiness skills, so that they would be prepared for socialisation before starting Grade I work.
As a requirement, preschools should have a nurse as one of their staff. It was found that very few private preschools with population ranging from 80 to 250 children aged between two and six years actually have nurses among their staff and most include the minimum number of staff for non-teaching tasks and administration.
Generally, participation in preschool was lower than the participation rate in day care in the three regions (Table 3.1.3.5). Regions VI had the highest participation rate among the three regions, although it is lower when compared with the day care participation rate as presented in the earlier section. This is mainly due to the higher tuition rate for preschool services. For instance, in Bucao, Botolan, Zambales, the tuition for pre- elementary school was PhP150 per month compared to PhP50 for the day care tuition. Despite, the offer of reducing the tuition fee to PhP100 per month, parents opted to enroll their children in the day care. As such, there is competition between pre-elementary and day care services in Barangay Bucao.
Table 3.1.3.5. Participation rate of children aged 0-71 months in preschool services (DepEd and Private), Regions VI, VII and XII, Philippines: 2000-2004 Region 2000 2001 2002 2003 2004 VI 39.8 39.9 37.1 37.6 37.4 VII 19.5 18.9 20.3 22.3 25.9 XII 20.4 19.5 22.9 26.2 27.1 Total 25.4 24.9 26.4 28.6 29.8 Source: ECDP, 2005
In 2005, the DepEd launched the National Pre-school Education Program in line with Pres. Arroyo’s Ten-Point Pro-Poor Legacy Agenda for 2005-2010, her 2004 SONA to “standardize what is taught in barangay day care centers,” and Executive Order No. 349 (2004) which provides that “the government will incorporate pre-school in the education ladder to encourage early childhood development.” This program aims to achieve universal coverage of all five-year-olds for pre-school by 2010.
To determine the school readiness of all incoming Grade One pupils, the School Readiness Assessment Tool (SRAT) is now administered twice in a school year in public
21
schools (DepEd Order no. 13, s. 2006; DepEd Order no. 25, s. 2007). The assessment includes the different developmental domains, the results of which are used as bases for providing interventions in school and in homes.
The conceptual framework and structure of the SRAT is similar to the Revised ECCD Checklist which was designed in 2002 “to objectively monitor a child’s development” in seven developmental domains. It is to be administered to children from aged 0 months to 5 years 11 months. This is presently used in the DCCs as assessment tool in order to identify children at risk for developmental delays and to input for curriculum development.
Data on early childhood experience is not as readily available as with the health and nutrition status of children. Data were sourced from research studies, thus national estimates are rarely available. As noted earlier, provision of DCS was devolved to the LGUs with the DSWD providing technical assistance. It was not clear if there is any monitoring mechanism. Thus, data on the number of DCC and DCWs and participation rate of children are not as available as with the other indicators for children aged zero to six years.
3.1.4 Social Protection
3.1.4.1 Street Children
These are highly visible children, spending more than four hours on the streets. The national estimate ranged from 45,000 to 50,000. Of these children, 75 percent are with families, 20 percent refrain from going home, and 5 percent are without families.
A UNICEF study (2002) of highly visible children in 22 cities nationwide covering 8,513 sample children showed that 46.5 percent of the street children were 6 to12 years old, 31.5 percent were 13 to 15 years old, and 8 percent were 2 to 5 years old.
Segregated by gender, the highly visible children on the streets were mostly males (67.7%) than females (32.2%). These children generally belonged to a large family, having an average of five living brothers and sisters. In birth order more than half (61.8%) were middle children and about one-fourth (25%) were the eldest. About one- third of the children did not go to school the past school year. The highest percentage of those who dropped out of school has reached primary level (40.4%).
The reasons cited for not going home were: (1) to earn money (3.2%); (2) did not like home chaotic home/afraid of parents (21%); (3) physical/verbal abuse from parents/siblings (21.4%); (4) separated parents with step parents (5.9%); (5) accessibility to distance from home (7.4%); (6) abandoned/do not know where parents were (14.7%); (7) poor living conditions/ basic needs not provided (2.1%); (8) like to be with friends/peers (2.7%); (9) stow away (8.3%) no house prefer to stay in the center (13.3%); (10) they have used prohibited drugs the past six months (15.4%); and (11) they are into rugby sniffing (81.9%), shabu (19.7%), syrup (2.4%), and marijuana (17.8%).
3.1.4.2 Child Labor
Child labor as defined by International Labor Organization (ILO) as forced labor in hazardous and exploitative conditions and deprivation of education opportunities. In the Philippines, child labor is defined as the illegal employment of children below the age of
22
15 who are not directly under the sole responsibility of their parents or guardian or whose works do not impair their normal development. Child labor also includes children below the age of 18 who are employed in hazardous situations (KC Link 2003). There were four million child laborers age 5 to17 years who were predominantly from rural households (67.1%) in Regions IV, VI and XI. A total of 65 percent were boys, 59 percent were exposed to hazards, six out of 10 were unpaid, 64 percent were in agriculture, 16.4 percent were in sales, 9.2 percent in production work, and 8.8 percent in services/trade. Thirty-seven percent of working children did not go to school (NSO 2001).
As indicated earlier, child labor is a serious problem in the Philippines, particularly in the rural areas where the age requirement for schooling and work is not enforced. Children work for long hours with minimal pay in farms or factories. Their work conditions are devoid of stimulation for physical and mental development.
3.1.4.3 Children with Disability
This category of children in need of special protection has more boys than girls. One of five children in zero to six age bracket has some form of disability, with those in the 10 to 14 age groups having the highest prevalence rate. The most common form of impairment is hearing and visual disorder. More than half are acquired and can be prevented (NSO 2000 census). Only two percent of persons with disabilities of school age are enrolled in formal educational institution (UNESCAP 2006).
This situation exists despite international and local mandates declaring that education is a basic right for all children and calling for the inclusion of all children in primary education. Infants and children with disabilities require access to early intervention services, including early detection and identification (birth to four years old) with support and training to parents and families to facilitate the maximum development of the full potential of their disabled children. Failure to provide early detection, identification, and intervention to infants and young children with disabilities and failure to support their parents and caregivers results in secondary disabling conditions which further limit their capacity to benefit from educational opportunities. Provision of early intervention should be a combined effort of education, health, and social service (UNESCAP 2003).
According to the Philippine definition, disability means a physical or mental impairment that substantially limits one or more psychological or anatomical functions of an individual. It further defines persons with disability as those suffering from restriction of different abilities as a result of mental, physical or sensory impairment in performing an activity in the manner or within the range considered normal for a human being.
As cited in the PES module for parents, one out of five children aged zero to six years suffers physical and mental disabilities. Fifty percent of these are acquired disabilities in hearing, vision, and movement. Majority of these children come from poor families who are unable to provide even the basic needs of their “normal” or able-bodied children. It was also pointed out that the government has not been able to provide adequate special education for these children. These children’s situation in the rural areas is more serious because they have not received even basic education. These children are also confronted with other problems, ranging from discrimination to lack of access to adequate social services. Globally, less than 10 percent of the world’s disabled children attend school.
3.1.4.4 Children in Other Difficult Circumstances
23
There are other situations wherein children are in disadvantaged positions. However, due to lack of information, it is very difficult to determine whether children aged zero to six years old are involved or not and the extent and nature by which the preschool children are affected. These are the children in ethnic/cultural communities, undocumented immigrants, victims of commercial sexual exploitation, sexual abuse, without primary caregivers, affected by HIV/AIDS, and victims of armed conflict.
3.2 National Policies on Early Childhood Care and Development
3.2.1 Nutrition Policies
As early as 1974, nutrition was already considered an important concern of the government. The first law that was enacted and declared nutrition as a priority was Presidential Decree (PD) 491 (Nutrition Act of the Philippines). It also mandated the creation of the National Nutrition Council (NNC) which is the highest policy making body on nutrition. The chairmanship of the NNC has been changed from time to time, e.g. Department of Agriculture (DA) to DSWD then to DA and now to DOH. The possible effect of this change could be in the focus or perspective of program implementation. With DA, the program included food and nutrition; with DOH, the focus were nutrition and health services. Nevertheless, the preschool children are still included as target groups.
The other laws that were passed related to or have an impact on nutrition can be grouped into three categories (Table 3.2.1), namely: 1) laws providing legal framework and budget for specific interventions to be implemented; 2) laws related to the organization and structure of NNC; and 3) laws identifying and deploying nutrition workers at the local levels.
Table 3.2.1. List of some nutrition and related laws Category 1-Legal Category 2 – Organization and Structure Category 3-Nutrition Workers Framework at the Local Level 1. RA 7600 “The 1. PD 491 Nutrition Act of the Philippines 1) P.D. 1569 “Strengthening Rooming-in and 2. LOI 441 in 1976 which specified the the Barangay Nutrition Breastfeeding Act” functions of the different members Program by Providing for (1992) 3. EO 234 Reorganization of NNC (1987) a Barangay Nutrition 2. EO 51 “Milk Code” which called for the expansion of the Scholar in Every (1986); membership of NNC to include the Barangay, Providing 3. RA 8172 “Act of Salt Departments of Labor and Employment, Funds Therefore, and For Iodization Trade and Industry, Budget and Other Purposes” Nationwide” (1995) Management and the National 2) RA 7883 “An Act Granting 4. RA 8976 “An Act Economic Authority (NEDA) Benefits and Incentives to Establishing the 4. Administrative Order 88 (1988) which Accredit Barangay Health Philippine Food transferred the NNC back to the DA Workers and for Other Fortification Program from the DSWD Purposes” and for Other 5. EO 472 transferring NNC to the DOH. 3) P.D. 1286 Practice of Purposes”. Nutrition and Dietetics in the Philippine, and for Other Purposes
24
In the third category, PD 1569 mandates the implementation of a Barangay Nutrition Scholar (BNS) program and that one BNS per barangay should be identified and appointed. However, some barangays do not have a BNS. RA 7883 provides for the training and deployment of Barangay Health Workers (BHWs). The BHWs would be responsible for providing primary health care services in the community after having been accredited properly by the DOH. Unlike the BNS, they are entitled to hazard allowance, subsistence allowance, free legal services, and preferential access to loans. The ideal ratio of BHW to households is determined by DOH. PD 1286 was signed in 1978 and it provides for the regulation of the practice of the Nutrition and Dietetics profession. The law also states (among others) that there should be at least one nutritionist-dietitian for each province, city, municipality, and rural health unit. However, this law has not been fully enforced as it is not considered a priority position in the Local Government Code (LGC).
Worthwhile to be mentioned as well is the LGC which was enacted in 1991. The law mandated the transfer of powers from the national government agencies (NGAs) to the LGUs to plan, implement, monitor, supervise, and improve basic services including health and nutrition. The law facilitated the implementation of various programs in an integrated manner under the leadership of the local chief executives (LCEs). It also opened new doors for NNC to explore coordinative strategies. The chair of the local nutrition committee is the mayor or governor. The members of the committee are the heads of agencies that implement nutrition and related interventions.
In terms of laws on nutrition, no new laws have been passed after the ECCD system has been implemented. The transfer of the NNC to the DOH from DA was not related to the implementation of the ECCD law. Previous to the implementation of the ECCD law, nutrition laws such as food fortification and salt iodization were implemented. Recently, the NNC has conducted a mid-term review of the MTPPAN. Hence, some changes in the strategies that would further improve implementation of nutrition programs are expected to happen before 2010.
3.2.2 Health Policies
A number of national policies, plans and frameworks, and programs are already in place, targeting various aspects that impact on newborn and child health, implementation, and monitoring and evaluation.
Under a decree (P.D. 996), all children below eight years old must receive vaccinations against tuberculosis, diphtheria, tetanus, pertussis, polio, measles, rubella, and other basic immunization which the Council for the Welfare of Children (CWC) will recommend to the DOH. The Expanded Program of Immunization (EPI) is a program of the DOH that implements this decree. In practice, rubella is not included in the EPI schedule of immunization. Although rubella is not usually accompanied by complications in young children, rubella in pregnant women particularly in the first trimester can lead to debilitating and disabling conditions in the infant such as deafness, cataracts, and congenital heart disease.
EPI schedules the above immunizations during the first year of life. Newborns and infants less than one year old are followed up by the BHW to encourage immunization. However, there is a need for greater surveillance of children more than one year old who have not completed the above immunizations as the decree provides for immunization of children below eight years old. Even the EPI TCL in the ECCD areas included only infants immunized. The reporting for full immunization covers infants less than 11
25
months only. Immunization services have been extended to children one to eight years old mostly during nationwide immunization campaigns. There have been campaigns against measles and polio which have included children less than eight years old regardless of vaccination status.
The EPI must have provisions for the immunization schedule of children beyond the first year of life and health care providers must be correspondingly trained. Section 6 of the decree provides for immunization of school entrants who have not received the immunization. According to of one the DCW interviewed, the immunization status of their students is obtained during enrollment. Those who have not completed the immunization are advised to go to the health center. There must be coordination between the DCW and health centers to ensure that preschool entrants get immunized. There must be a surveillance system of to ensure that both private and public schools follow the PD. The current recommendation of most pediatric specialist organizations is to give a booster of DPT and polio at 18 months and at four years old. The EPI may be extended to give compulsory DPT/polio immunizations upon entry to the day care.
Compulsory immunization against Hepatitis B for infants and children below eight years old was articulated under RA 7846. Among the immunizations offered in the EPI, Hepatitis B vaccination has the lowest reported coverage mainly because of inadequate supply of the vaccine. If there is not enough supply of this vaccine for infants, more so for children ages one to eight years old.
There is a need to emphasize the importance of Hepatitis B vaccination among the community residents, health providers, and local governments. Hepatitis B infection increases the risk of cancers of the liver; this form of cancer thus may be preventable. If there is increased awareness of the importance of the vaccination, then there may be corresponding increase in government commitment and support. One way of increasing, awareness is to include Hepatitis B vaccination in the reporting of a fully immunized child.
The specific population of persons at risk of Hepatitis B infection are infants born to mothers who are carriers of the infection. Special attention to this group was provided in Section 2 of the decree. It states that infants of women with Hepatitis B shall be given the vaccine within 24 hours after birth. Therefore, to control the spread of the infection, there must be an accompanying policy for compulsory screening of all pregnant women for Hepatitis B or compulsory immunization within 24 hours of birth for all infants regardless of the Hepatitis B status of the mother.
The Rooming-in and Breastfeeding Act (RA 7600) of 1992 provides incentives to all government and private health institutions with rooming in and breastfeeding practices. The policy states that the Senate adopts rooming in as a national policy to encourage, protect, and support breastfeeding practices. The benefit of breastfeeding has long been established. However, breastfeeding rate has declined probably because of a number of factors such as increasing number of working mothers, mothers not well-informed about the benefits of breastfeeding, and marketing strategies of formula milk manufacturers. This Act imposes breastfeeding practices in government and private hospitals by giving incentives to those that adopt the policy and by giving sanctions to those that violate the Act.
One of the incentives listed in Section 13 is tax deduction of expenses incurred by private hospitals in complying with the Act provided that the hospitals comply within six months after the approval of the Act. For government institutions, they shall receive an additional appropriation equivalent to the savings derived as a result of adopting the
26
rooming in and breastfeeding policy. There is no detail given as to the nature of the savings. Perhaps the only tangible and direct saving from breastfeeding is the cost of milk formula which is purchased by the parents. It is very difficult to quantify the savings from decreased infections, decreased hospitalizations, or decreased staff and utility requirements in nurseries. Sanctions were clearer, ranging from reprimand or censure to suspension of the license to operate in case of repeated and willful violations. There appears to be less commitment to giving incentives compared to giving sanctions in the implementation of the Act.
Newborn Screening Act (RA 9288) of 2004 promulgates a comprehensive policy and a national system for ensuring newborn screening. This policy ensures that every infant born in the Philippines will be given an opportunity to be screened for diseases that when left untreated may lead to complications such as mental retardation or even death.
One of the provisions of this policy is the responsibility of the health provider who attends or assists in the delivery of an infant. The Act provides that the DOH must inform and educate the health providers about this responsibility. Since many pregnant women deliver at home attended by midwives and trained hilot, there must be an extra effort to educate health providers who engage in private practice and are not connected with any agency. Different agencies also need to collaborate more in promoting newborn screening.
NBS is one ECCD program that has not been implemented by the municipality of Botolan. The members of the council have not attended any training on NBS at the time of interview. However, NBS facility was already available
The provision on the establishment of newborn screening centers is not so clear on whether private laboratories can offer newborn screening tests as testing kits are commercially available. Rather than preventing them, there must be a provision for accreditation, quality control, monitoring and evaluation of existing laboratories who would want to offer newborn screening test apart from that offered in the NIH. Private laboratories and paying patients may have the resources for more diseases to be screened. This would mean more benefit to those newborns who have access to such tests. Accreditation will also ensure that the tests being offered are of good quality. If these private laboratories are not accredited and they still offer the tests, then there would be a group of newborns who will not be included in the national database for NBS.
Newborn screening rate is quite low for a number of reasons. In fact, statistics on livebirths screened are only available from 2004 up 2006. Moreover, the screening rate was very low at 4, 7 and 11 percent in 2004, 2005 and 2006, respectively. The main reason is that the service is quite new, thus it is not as widely known to health providers in the rural areas and available in the health facilities compared with the other health services for children. The other reason is the cost, about PhP600, which is not affordable for many couples. Though PhilHealth offers a discount of PhP100 for its members, it is still costly for them more so for the many non-members.
3.2.3 Early Childhood Education Policies
Twenty-five years ago, the first law promoting early childhood education in the Philippines was passed. PD1567 or the Barangay Daycare Law provided that at least day care center in every barangay with at least 100 households must be built in order to run early childhood socialization activities for neglected preschool age children. The day cay center shall “look after the nutritional needs and social and mental development of all
27
children from ages 2 to 5 when their parents are unable to do so.” It was the first act of government to provide state funded early childhood education.
Meanwhile, laws which are broad in scope have also provided the legal basis for the development and implementation of Early Childhood Enrichment Project. This refers to PD 603 or the Child and Youth Welfare Code of 1978. PD 603 clarifies the responsibilities and obligations of the state and its citizens in relation to children as well as the duties and responsibilities of children and youth themselves (UNESCO 2004). The Early Childhood Enrichment Project (ECEP) from 1978 up to the mid-80s gave the day care program a much needed-boost in the 1980s.
Then in 1990, Republic Act 6972 or the Barangay-Level Total Development and Protection of Children Act. RA 6972 mandates the establishment of a day care center in every barangay with a total development and protection of children program. The first law centers on socialization activities while the latter emphasizes the total development of children. RA6972 included programs 1) monitoring the registration of births and the completion of the immunization series for prevention of tuberculosis, diphtheria, pertussis, tetanus, measles, poliomyelitis and such other diseases for which vaccines have been developed for administration to children up to six (6) years of age; 2) growth and nutritional monitoring, with supplementary nutritional feeding and supervision of nutritional intake at home; and care for children of working mothers during the day and, where feasible, care for children up to six (6) years of age when mothers are working at night. Further, RA6972 also emphasized that children are the community’s collected responsibility and that the barangay must ensure a safe environment that promotes that total development.
The provision of DCS has been extended to places outside the barangays. Executive Order No. 340 (1997) directs national government agencies and government-owned and -controlled corporations to provide day care services for their employees' children under five years of age. These services shall include proper care and nutrition; development of social and intellectual skills, spiritual, socio-cultural and nationalistic values; substitute parenting and protection from neglect, abuse and exploitation.
All these years, the Department of Social Welfare and Development (DSWD) was mandated to manage the day care program of the government. Then in 1992 when the Local Government Code of 1992 was passed, the DSWD together with the Department of Health and Department of Agriculture transferred their political and administrative authority, functions and responsibilities to the local government units. For the day care program, this meant that only the policy and program development and technical assistance was retained with the DSWD. The supervision of the provincial and municipal welfare and development officers, and the allocation of funds for early childhood education rest with the local government executive. Similarly, the health and nutrition functions and responsibilities of the other departments where decentralized. The quality and access to the provision of early childhood education depend largely on the priority of the local government units. The allocation of funds for training over other competing requirements like infrastructure could mean a lot to the total development of children. As it is, there is so much to be done to improve the quality and access of children to early childhood education (UNESCO (2004).
Despite the passage of RA6973 some barangays do not have day care center. At the same time, the status, wages and working conditions of day care workers which form critical aspect of early childhood education remained unchanged through the years. According to UNESCO (2004), a day care workers is one of the most underpaid, overworked and inadequately supported public servants.
28
As early as 1971, the Bureau of Public Schools encouraged the public sector to organize pre-school classes through their parent-teacher associations (Memo no. 25, s. 1971). The Education Act of 1982 or Batas Pambansa Building 232 provides for compulsory basic formal education corresponding to six or seven grades, including preschool programs. In 2001, the Governance of Basic Education Act (R.A. 9155) reiterates that early education is part of basic education which is the foundation for subsequent learning.
The goals of ECE, as stipulated in MECS Order no. 8, s. 1986, are to prepare children for elementary schooling and to improve pupils’ achievement at the elementary level. These goals seemed to have shifted in the 1990s. The Master Plan for Basic Education 1996-2005 articulated that the aim of ECE is to provide children with ECCD, thus, the focus became the total development of children.
Standards for the organization and operation of nursery classes (for children aged three to four years old) were developed in the 1970s (Department Order no. 60, s. 1975 and MECS Order No. 24, s. 1978).
In 1987, the Coordinating Council for Pre-school Education in the Philippines (CONCEP) was established. CONCEP is a body of pre-school specialists from the private and public sector tasked to coordinate pre-schools all over the country. It articulated guidelines for the regulation, licensing, organization, management and supervision of private and public pre-schools (MECS Order no. 60, s. 1975; DECS Order no. 41, s. 1985; DECS Order No. 107, s. 1989; DECS Memo no. 100, s. 1997).
The effect of the decentralization and the concern for the integration and convergence of services for the total development of children aged 0-6 years old have provided the impetus for the passage of the Early Childhood Care and Development Act in 2002. Among others, the ECCD Act provided for the institutionalization of a National System for Early Childhood Care and Development that is comprehensive, integrative and sustainable involving multi-sectoral and inter-agency collaboration at the national and local levels among government; among service providers, families and communities; and among the public and private sectors, non-government organizations, and academic institutions. Of special mention are children with special needs and advocate respect for cultural diversity.
As mandated by R.A. 8980, the DSWD is responsible for regulating the quality of ECCD programs for children, including those provided through various centers. Thus, in 2004, the DSWD developed accreditation standards and indicators to ensure effective and quality delivery of the Day Care Service and other ECE-ECCD programs for children below six years old through various centers and its service providers (A.O. no. 29, s. 2004; E.O. 221).
However, functions of standard setting and issuance of permits are assigned to the DepEd. Because of the overlap, the National ECCD Coordinating Council defined and delineated the roles and functions of the DSWD and DepEd on the accreditation and licensing of center-based ECCD programs in 2004 (Council resolution no. 1; DepEd joint memorandum circular no. 001-12-04).
The Medium-Term Philippine Development Plan 2005-2010 include among others the following policies on education: . pre-school as a prerequisite to Grade 1 and part of the education ladder;
29
. the present barangay DCCs to provide ECE services following a standardized ECE curriculum for five-year olds; . the present coverage of organized ECCD programs to expand to reach all five-year-old children, with priority to children of poorest households; . DepEd to adopt the Standard SRAT; and . DepEd, in coordination with DOH and LGUs, to expand health and nutrition programs in public DCCs and preschools
UNESCO (2004) believes that the integration of ECCD services happen at the household level and not at the day care centre or any service delivery point. Thus, it is a challenge for the ECCD implementers to center all its efforts on the family unit. Moreover, there are a number of activities that the ECCD needs to address, including the following:
Activating and strengthening of the multiple layers of co-ordination; Intensify the efforts to secure the necessary resources for programming and to explore more and better ways to work with children and families; and Develop more opportunities for the interaction of various stakeholders for developing program features or processes for the full realization of the ECCD objectives.
BFurther, despite the passage of laws from both the legislative and executive branches, there are still issues which have to be responded to by the government. These are as follows:
. While the roles and responsibilities of the DSWD and DepEd in the registration, licensing and accreditation of center-based ECCD programs have been delineated, there is still no policy recommendation or joint circular for the adoption of DSWD’s “Standards for Day Care, Other ECCD Centers and Service Providers” by the DepEd for public and private pre-schools; and the Curriculum Framework (Early Learning Standards for 0-6), which has not yet been developed, must ensure that foundational principles, curriculum, teaching-learning experiences and materials, and evaluation/ assessment processes and procedures are developmentally-appropriate for ECCD children and that smooth transition and continuity across age groups and settings is established, regardless of which operating ECE programs are under the jurisdiction of DSWD and DepEd. Note for example that the use of workbooks in the DCS is not an indicator of service quality in the Standards.
. Pres. Gloria Macapagal-Arroyo’s 2005 SONA commitment to make pre-school education a prerequisite to Grade 1 and part of the education ladder shall be able to meet its goals efficiently and effectively only if home-, community-, and center-based early education programs for children below 6 years old (under DSWD) are strengthened and expanded in terms of service quality and availability in barangays and other settings; and the total development of children, not preparation for elementary schooling alone, remains the imperative of all early education programs, including Early Childhood Experiences in Grade 1.
. Parallel to this, creative and dynamic mechanisms for the professionalization of the said programs’ service providers are to be developed and implemented. R.A. 6972 treats day care workers as “private volunteers, who are responsible members of the community” and enjoins the Sangguniang barangay to tap them to provide “consultative services for medical, educational and other needs of children.” While this long history of barangay- level volunteerism has become the backbone of ECCD service delivery, it has
30
likewise exploit the service providers because they are in reality extending full-time work.
. Moreover, early education programs for children aged 0 to 3 years old have to be given more legislative, programmatic, and financial support. This age group belongs to an even more critical stage in children’s development and early stimulation and interventions produce significant positive outputs in learning.
. There is a need to intensify the training and monitoring of service providers on the utilization of assessment results—from the Revised ECCD Checklist or the SRAT— for curriculum planning so that children’s early education experiences are appropriate, stimulating and challenging.
. Orientation and capacity-building programs must be conducted directly with the service providers and not through various levels. Training design and methodologies need to be evaluated at the LGU level in order to improve ways of building competencies of the service providers according to standards and other benchmarks.
. Policy guidelines and implementation need to be set on long-standing conflict points between the DCS and public school-based ECE programs like the PTCA-initiated kindergarten classes competition in terms of serving the same clientele (mostly the four- and five-year-olds) since the monthly honorarium of DCWs and kinder teachers largely come from the monthly contributions of the enrollees; and preference of public schools for Grade 1 entrants who enrolled in the PTCA-initiated kindergarten class the previous year; school heads reason that “it is easier to teach such children in Grade 1 than children who come from DCCs”.
. Because PD 1567 mandates that a DCC must be established in every barangay with at least 100 households and R.A. 6972 states that “a DCC is to be established in every barangay,” some LGUs limit the number of DCCs to only one in each barangay. Factors such as population of target clientele, non-maximized facilities (such as unused classrooms in DepEd schools), and conduct of DCS sessions in the afternoon can justify the construction of new DCCs or expansion of the DCS in the community.
3.2.4 Social Protection Policies
In 1989, the Philippines became a signatory to the United Nation’s Convention on the Rights of the Child (UNCRC), which was ratified in July 1990. Through this international commitment, both government and NGOs were provided a meaningful shift in the framework for program development, policy formulation, and intervention strategies for children. This new direction brought about legislations embodying the rights of children broadly categorized as rights to: survival, development, protection, and participation. However, long before the advent of the Convention on the Rights of the Child in l989, the Philippines had already formulated a landmark legislation for children as early as June l975, with the passage of PD 603, otherwise known as the Child and Youth Welfare Code. The Code recognizes that the child is one of the most important assets of the nation and it upheld the “natural right and duty of parents in rearing of the child for civic efficiency”. The code explicitly detailed 12 rights of the child, two of which (Nos. 8 and 10 of Art. 3) were specific to their “rights to protection against exploitation, improper influences, hazards and other conditions or circumstances prejudicial to his physical, mental, emotional, social and moral development.” Further it states, that “every child has
31
the right to the care, assistance and protection of the state particularly when his parents or guardians fail or are unable to provide him with his fundamental needs for growth, development and improvement”. “Moreover, special categories of children, such as the dependent, neglected and abandoned, the physically and mentally disabled, and youth offenders below 21 years old are protected by the State under the doctrine of parens patriae.” Also, this decree created The Council for the Welfare of Children in August 1975. Specific legislations which focus on child protection are evident in Table 3.2.4
Table 3.2.4 Legislations related to child protection Republic Act RA 7610 Otherwise known as an act providing for stronger deterrence and Special Protection against child abuse, exploitation and discrimination (1992) RA 7727 Magna Carta for Disabled Persons (1992) RA 8369 Family Courts Act of 1997 RA 8552 Domestic Adoption Act of 1998 RA 8043 Inter-Country Adoption Act of 1995 RA 8980 The Early Childhood Care and Development Act of 2000 RA 9344 The Comprehensive Juvenile and Justice Welfare Act of 2006
Executive Order (EO) EO 275 S 1995 Creating a Committee for the Special Protection of Children from all forms of neglect abuse, cruelty, exploitation, and discrimination to their development EO 184 S 1999 Establishing the Presidential award for the Child Friendly Municipalities and Cities EO 310 S 2000 Authorizing the adaptation and implementation of the Phil. National Strategic Framework for Plan Development for Children 2000- 2025 or child 21 and its Accompanying Medium-Term Plan and Framework EO 56 series of Adapting the Comprehensive Framework for Children in Armed Conflicts 2001 and Directing National Government Agencies and LGUs to Implement the Same
3.2.5 The ECCD Law (RA 8980)
Given the legal framework through which ECCD interventions were initiated under various statutes covering nutrition, health, early education, and child protection, Republic Act 8980, otherwise known as the Early Childhood Care and Development Law was promulgated in 2000. The basic element of the law was to provide a system based on multi-sectoral and inter-agency collaboration in the delivery of a comprehensive, integrative, and sustainable ECCD services at various levels from the national to the local levels of implementation. However, it must be noted that, while the existing statues have broader scopes, ECCD is focused on the welfare of children from zero to six years old. In more specific terms, from inception to an age under seven years.
32
To achieve the goals outlined in the Law, the following components were identified: (1) early childhood care and development curriculum, (2) parent education and involvement, (3) human resource development program, (4) ECCD management, and (5) quality standards and accreditation.
In terms of Program implementation, the law provides for the creation of ECCD Coordinating Committees from the national down to the provincial, municipal, and barangay levels. It must be noted that at the barangay level, the Barangay Council for the Protection of Children (BCPC) was also designated as the Barangay ECCD Coordinating Committee. The Barangay ECCD Coordinating Committee as provided for under P.D. 603 (for the BCPC) is constituted by the following: Barangay Captain, School Head, BHW, BNS, DCW, Sangguniang Kabataan (SK) Chairman, parents, and NGO representatives.
4.0 THE CASE STUDIES
4.1 Province of Zambales
4.1.1 Profile
Zambales is located along the western coast of Central Luzon. It is bounded on the north by the province of Pangasinan; on the east by Tarlac and Pampanga; on the south by Bataan; and on the west by China Sea. The topography of the province is generally irregular, with the coastal plains and valleys stretching from Lingayen Gulf down south towards Subic Bay along the western coast and further towards a 17 kilometers (km.) stretch of shoreline.
Zambales has a total land area of 3,714.4 square kilometers (sq. km). Botolan and San Marcelino have the largest land area with 613.7 sq. km. and 440.9 sq. km., respectively. These are the towns where the mountain ranges of Zambales are found. Sixty-nine percent of the land area is classified as timber land.
As of 2000, the province has a total population of 627,802. Olongapo City had the highest number of population at 194,260 followed by Subic with 63,019 and Sta. Cruz with 49,269. The Municipality of Botolan where Barangay Porac is located ranked fourth with 46,602 total population.
While the number of infant deaths decreased from 2000 to 2003, there was a notable increase from 2001 to 2002. This was in contrast to the country’s pattern where there was a decrease in infant deaths from 99 or 11.4 per 1000 livebirths reported (FSHS 2006). Infant deaths were a lot higher compared to deaths in the one to four years and in the 5 to14-year age groups. The high incidence of under-five mortality was attributed to the group’s inherent low resistance to diseases aggravated by the inadequate supply of essential drugs especially to the underserved population.
The most common causes of infant mortality had not changed from 1998 to 2003. Pneumonia remained to be the most common cause. Five out of the 10 leading causes were conditions present during the newborn period such as prematurity, congenital anomaly, sepsis neonatorum, ARDS, and asphyxia neonatorum. In the 2006 FHSIS data, Zambales had eight deaths from neonatal tetanus equivalent to a rate of 0.9 per 1000 livebirths.
33
The following are the health services offered in the province:
Expanded program of immunization. There was no common trend for all the municipalities in the province on this aspect. Only San Antonio had a steadily increasing trend during the four-year period while the rest of the municipalities showed fluctuating rates. However, full immunization rates were higher in 2003 compared to 2002 in Palauig, Botolan, Cabangan, San Antonio, San Marcelino, Castillejos and Subic. The total full immunization rate for the entire province did not vary greatly but the rate in 2003 was lower than the rate in 2000.
Hepatitis B vaccination has been included in the EPI but has not been widely implemented yet. The provincial accomplishment for Hepatitis B immunization from years 2000 to 2003 was low because of the irregularity and inadequacy in the delivery of vaccines. In 2003, the rate was lowest in Masinloc (20.4%), Palauig (21.3%), and Botolan (32.5%), while the highest was in San Felipe (72.8%).
Prenatal and postnatal care. The percentage of pregnant women who received tetanus immunization during prenatal checkup was 43 percent in 2003. This was higher than the 2000 value at 38.6 percent. Pregnant women were also informed about the benefits of breastfeeding. Regional Health Unit (RHU) personnel and BHWs conducted health education to motivate them to breastfeed exclusively.
After the delivery of the infant, the personnel visit post-partum mothers at least twice before the cord stump falls off. Post-partum mothers go to the clinic for at least one post- partum check-up. The percentage of mothers who had at least one post-partum check- up declined steadily from 61 percent in 2000 to 49.3 in 2003. In 2003, it was lowest in Subic at 22.9 percent and highest in Castillejos at 87.9 percent.
Moreover, malnutrition remains to be a problem of Zambales, affecting particularly young children. From 2003, the province started to use the International Reference Standard (IRS) for classifying the nutrition status of children. Based on the IRS, the prevalence of below normal (low and very low) weights among preschool children declined steadily from 2003 to 2005. However, the prevalence increased from 9.79 percent in 2005 to 11.37 percent in 2006.
Examining the occurrence of underweight according to age group in 2004 and 2005, it is apparent that the prevalence is lowest at 0 to 11 months old (0.69 %) compared to any age group between 12 and 71 months (1.86-2.31%). However, 2005 data showed an increased frequency in the 0 to 11 months old to 0.82 percent while there was a decline in the prevalence in age groups 12 to 71 months.
The incidence of below normal weight was higher among school children (age 6 to12 years old) compared to preschool children in all years studied. However, the increasing trend from 2005 to 2006 was also noted in the school-age children.
Micronutrient deficiency is another public health concern in Zambales. According to the FNRI data in 1998, 13.4 percent of children six months to five years old in Zambales had vitamin A deficiency. This was higher than the prevalence in Region III (6.8%) and in the Philippines (8.2%). The same observation was noted in iron deficiency anemia wherein the prevalence in children six months to five years old in Zambales was higher than the regional and national values. Iron deficiency anemia was highest in children six months to one year old at 68.6 percent and lactating mothers at 60.5 percent. Anemia in pregnant women was 38.9 percent, which was lower than the regional and national values.
34
4.1.2 ECCD Structure and Management
The Governor is the over-all chairman of the ECCD system and the PECCDCC is the managing team. The provincial government has an existing Sub-committee for the Welfare of Children (PSCWC) which also serves as the PECCDCC. The chair of PECCDCC is the Provincial Social Welfare and Development Officer while the School Division Superintendent acts as the Vice-Chair. The members are composed of the representatives from the Provincial Health Office (PHO), PPDO, Provincial Population Social Services Division, Provincial Nutrition Action Office (PNAO), Department of Interior and Local Government (DILG), Provincial Finance Committee, Philippine National Police or PNP-Women’s Desk Officer, Chairman, Provincial Council Committee on Social Services, PSWDO, NGO (Hiyas ng Pagasa), PO (ABSNET) and DSWD-SWO II.
The provincial government hired an Assistant Provincial ECCD Officer (APECCDO) in accordance with the guidelines set by the CWC. CWC guidelines allow the LGU to hire either a PECCDO or an APECCDO. However, the province of Zambales has opted to hire an APECCDO for reasons that an outside person lacks the connections with the agencies involved. While the other members of the PECCDCC have other responsibilities outside of ECCD, the APECCDO’s responsibility is solely on ECCD, and s/he acted as the over-all coordinator of the program.
Every ECCD municipality has its own management team referred to as the MECCDCC. In Botolan, the Municipal Council for the Protection of Children (MCPC) also serves as the Municipal ECCD Coordinating Council (MECCDCC). ECCD matters are discussed as part of the agenda in MCPC meetings. In the barangay level, the BCPC functions as the Barangay ECCD Coordinating Council (BECCDCC). No additional staff was hired in Botolan and Porac for ECCD implementation.
4.1.2.1 Planning ECCD implementation in Zambales started in June 2006. But even prior to the passing of the ECCD law, the provincial government had already prepared a strategic plan to address the needs of children in their Local Development Plan for Children (LDPC) for year 2000. The detailed plan was sponsored by Vice-Governor Cheryl Deloso. Unfortunately, it was not implemented because of the lack of funding and change in administration after the elections. When the ECCD law was passed, the said LDPC was revived and was used as the basis for the ECCD implementation in the province.
In 2003, the province started compiling data from the component municipalities on the 10 indicators set by CWC as the basis for the selection of program areas. These 10 indicators are: 1) population of zero to six children; 2) maternal mortality rate; 3) infant mortality rate; 4) participation on ECCD programs; 5) drop-out rate in Grade 1; 6) prevalence of underweight; 7) prevalence of stunting; 8) prevalence of wasting; 9) under- five mortality rate; and 10) poverty incidence. Among these indicators, data available were only on the first six, which became the basis in ranking the municipalities. The ranking was utilized in the ECCD planning workshop to identify program areas. To concentrate the ECCD funds and to make a considerable impact, the top 3 municipalities, namely: Masinloc, Botolan, and Subic were chosen.
On March 23, 2005, the provincial council passed Resolution No. 2005-120 authorizing then Governor Vicente P. Magsaysay to enter into a Memorandum of Agreement (MOA)
35
with CWC National Executive Director Lina B. Laigo and DSWD Regional Director Margarita B. Sampang. The MOA was finally executed on December 28, 2005.
During the planning stage, the municipalities attended an orientation and workshop on ECCD. They were also required to submit an investment plan and work and financial plan (WFP). After the approval of the said plans, Resolution No. 2006-54 was passed by the Provincial Council adopting the said ECCD investment plan and WFP on March 6, 2006. The province was then required to raise an equity equivalent to 30 percent of the total investment plan for three years. Each municipality, on the other hand, needed to put up an equity of 10 percent. All of the required equities were met by the LGUs.
The municipalities used different bases for choosing the barangay to be included in the implementation of ECCD. In Masinloc, all 13 barangays were said to be included to avoid complaints from any barangay that would not be chosen. Five out of 13 barangays in Subic were included in the ECCD implementation; most of these barangays have significant numbers of Muslim communities.
In Botolan, 10 out of 31 barangays were included in the ECCD implementation. The selection was based on six criteria set by the CWC for which data were available. The 31 barangays were ranked according to the indicators. The ECCD team in Botolan together with the mayor decided to get the top 10 most needy barangays to be included in the program to concentrate the funds in priority areas. The MECCDCC recognized the commitment of the Mayor to the ECCD program; he has volunteered to shoulder the construction and upgrading of the health centers and DCCs so that the CWC fund could be devoted solely to the actual implementation of the ECCD programs.
4.1.2.2 Financial Management
The PECCDCC prepares a budget based on the investment plan and WFP submitted by the ECCD municipalities. Once approved by the CWC, arrangements are made for the transfer of the funds. The provincial government is required to put up a counterpart equivalent to 30 percent of the total budget before the release of the funds. The total ECCD budget for 2006 was PhP7,852,476.20. Eighty percent of the total budget was allotted for the ECCD implementation in the three selected municipalities. The 20 percent remained in the province for administrative and training expenditures under the Centrally Managed Fund.
ECCD implementation in Zambales started on the third quarter of 2006. PECCDCC released the budget to the three ECCD municipalities in two installments, each to finance the programs for two quarters of the year. Each municipality was required to put up 10 percent equity for the program implementation. After almost a year of implementation, utilization of the first half of the budget was 86.8 percent. The remaining funds were added to the budget for the second half of the year. The release of the second half of the fund was delayed because of the delay in the liquidation in some municipalities.
Botolan received a total of PhP2,095,238 for the first year of implementation. In addition to this, they put up an equity of PhP259,000.00. Only 46.5 percent of the total ECCD fund has been utilized after a year of implementation. The MECCDCC is the main administrating body of ECCD funds. It makes the purchases and distributes them to the 10 ECCD barangays in Botolan. MECCDCC also required equity from each barangay. The BECCDCC in Barangay Porac was not aware of how much fund was allocated to their barangay. However, they were asked to give PhP10,000.00 as equity for the feeding program.
36
4.1.2.3 Delivery System
The PECCDCC gave the municipalities the CWC guidelines on what programs may be funded by the ECCD. The MECCDCC then decided what programs they would spend the fund on. All the implemented programs in Botolan were included in the recommended programs by CWC. They have not implemented programs outside of the CWC recommendations because of the limitations set by the latter. The implemented programs in Botolan were supplemental feeding, day care service, eight-week curriculum, family planning, PES/ERPAT, micronutrient supplementation, nutrition education through PABASA, home and community food production, and maternal and child health care including prenatal and postnatal care, immunizations, and family planning. These services are administered and monitored by the respective agencies as it was before the ECCD implementation. Accomplishments are then reported to the MECCDCC.
At the barangay level, the barangay officials of Barangay Porac had their first meeting regarding the ECCD program in November 2005. According to them, they were included in the program because they had a high number of malnourished children in their barangay. In the implementation of the ECCD program, they have concentrated their efforts and resources on Sitio Bucao. This part of the barangay has a high number of Aetas that migrated from Mt. Pinatubo when it erupted in 1991. According to the reports of the BHW and BNS, there are many malnourished children among this subpopulation.
The barangay officials are the implementing team of ECCD in the barangay. There are no additional personnel hired for ECCD implementation. They attend regular meetings at the municipal level to discuss ECCD. However, there is no regular meeting for ECCD in the barangay level; ECCD matters are discussed during the BCPC meetings.
The MECCDCC is the main administrating body of the ECCD funds. The barangay council is not aware of how much fund is allocated to their barangay. But the barangay officials appreciate the presence of funding from the ECCD program. Because of ECCD, they have funding for their feeding programs. The MECCDCC has also distributed supplies for the DCC as well as medicines and some equipment for the health center. The barangays do not request for particular supplies; all supplies are purchased and distributed by the MECCDCC.
Although the provincial and municipal ECCD teams understand the ECCD programs, some of the barangay councils have no concrete understanding of what ECCD is all about. Some believe that all children under 18 years old are covered by the program.
4.1.3 Accessibility/Quality of ECCD Services
4.1.3.1 Health Services
The Bucao Health Center is located on a hill, about 30 meters climb from the main road. It is estimated to be two kilometers away from the farthest household. Walking through rocky trails is the only means for residents to go to these centers. Sitio Bucao has four BHWs assigned to a specific area to ensure that the residents are informed about health services. They usually go from house to house to inform residents of health programs or even to deliver health services.
37
The basic ECCD services are offered in the Bucao Health Center. These are immunization, prenatal and postnatal care, family planning, and primary health care. Most of the services are scheduled on the day that the rural health midwife (RHMW) is present in the center. She is present in the center once a week only and the task of carrying out unscheduled services lies on the BHW.
The Bucao RHMW said that majority of the population avail of all the services provided. In 2006, they have attained 100 percent full immunization rate in Bucao. Not all pregnant women go to the health center for prenatal and postnatal care. Some of them go to other service providers. In 2006, 29 pregnant women were seen in the Bucao Health Center. Thirteen were referred to other service providers for management of high-risk pregnancies. Eleven delivered in the hospital while 18 delivered at home. Only one of the home deliveries was attended by the RHMW. The rest were assisted by a trained hilot.
The RHMW estimated that about 10 percent do not avail of services. Possible reasons given were 1) distance from the health center, 2) the children work with their parents in the fields, and 3) the parents fear that the children might get sick after immunization.
4.1.3.2 Nutrition Program
Barangay Porac has invested on the feeding program because of its high malnutrition rate. According to the PNAO, an effective feeding program must be conducted for 120 days. In this program, the children are fed once a day either around noon or three o’clock in the afternoon. The budget is PhP12 per child. In Bucao, they were able to conduct a feeding program for 67 underweight children in 2006. The feeding program lasted for two months only. There was good participation with only one dropping out because the family transferred residence. However, out of the 67 participants only three gained weight and only one had a sustained weight gain even after the feeding program.
Another feeding program has been started in July 2007 with 48 participants. There has been an interruption to the feeding schedule because no food has been delivered from the MECCDCC. One reason for the delay in the delivery of goods is the procurement procedure as set by Commission on Audit (COA). No cash advances are allowed. No new funds are released if the liquidation of the previous disbursement has not been completed yet. This becomes a problem particularly in the feeding programs because the feeding should be conducted daily but the organizers should make requests and do canvassing every week to comply with COA procedures.
The BNS of Bucao also conducts the PABASA which is a mother’s class program about nutrition. The 10 modules for the program have been compressed so that the program can be finished in seven days. Upon completion, the participants are given an examination regarding nutrition. The BNS also encourages the families to plant vegetables to augment their food source.
38
4.1.3.3 Health and Nutrition: Quality
The health center in Bucao was observed to be used for only a week during the interview conducted. The RHMW and BHW were still organizing the center. The previous site of the health center was a corner of the multi-purpose hall. There was no distinct room for the health services. When the municipal office built a new building for the DCC, the old DCC was converted into a health center. There were no room divisions yet, as it used to be a classroom. There is, however, a curtained corner which would serve as the examination room. It has provisions for a toilet with plans to have water connection underway. The center has on its walls different information posters on immunization, family planning, and IMCI treatment protocol. Some are old but most are new and recently put up.
The Bucao Health Center has the necessary equipment for the delivery of services. From the ECCD fund, they have acquired a new Salter scale to measure weight more accurately than the commercially available scales. The center also has enough supplies of gloves and syringes though it doesn’t have medicines.
The Health Center is open eight hours a day from Monday to Friday. However, the RHMW is available only on Thursdays because she goes on duty in other health centers on the other days. Regular services such as immunizations and prenatal check-up are scheduled on a Thursday. Consultations or concerns from the neighborhood that arise on other days are initially attended to by the BHW. There are four other BHWs that rotate on duty at the health center so that at least one BHW is present. The BHW comes from different areas in Bucao and they have been assigned to promote the services to their respective areas.
In terms of competencies, the RHMW is a registered midwife. She has been in the service for six years. She has attended training seminars on IMCI, EPI and MCH. The BHW interviewed finished 3rd year high school. Before ECCD implementation, she has already attended trainings on tuberculosis, healthy lifestyle, and birth control. However, she has not yet attended any training on ECCD or health protocols.
The BNS, who also functions as a BHW, has completed a two-year secretarial course. She has attended a training to become a BNS. She was also able to attend the ECCD orientation in December 2006 together with the RHMW and was involved in the planning of ECCD activities. She goes on duty as a BHW at the health center every Thursday. She supervises the feeding program daily at 3 pm. There was good participation in the feeding program in 2006 with only three children unable to finish because they needed to transfer residence. There were instances when they brought the food to the house of the child who was not in the site of the feeding program. In some areas, there were complaints about the same type of food being given daily.
4.1.3.4 Early Childhood Education
The day care center is beside the health center and children who attend the service must walk through the same rocky path. To get to the DCC, one must pass across a one-foot wide and two-foot deep canal. The DCW says she has not heard any concern or complaint about the safety of the surroundings and that the children are used to it. Some of them are not even accompanied by their parents or relatives in going to school.
The day care service is under the direct supervision by the DSWD. It is offered to children three to five years old for a fee of PhP50 monthly. Teaching sessions are
39
conducted daily from Monday to Friday. Each session usually lasts three to four hours. In 2006 only 30 out of 80 children ages three to five years old were able to attend the day care. The DCW related that the IPs do not have good attendance in school for reasons similar to those given for not availing of health services. For those who live in the mountains, the day care may be as far as a half day walk from their residence. Some also cited financial reasons for not sending their children to the DCC.
Three out of the 30 children enrolled failed to finish the school year. Ten students were transferred to pre-elementary education in the middle of the school year because they were already five years old and were therefore eligible for pre-elementary.
The pre-elementary is under the supervision of DepEd. The pre-elementary teacher’s compensation comes from the monthly student fees of PhP150 per student. Furthermore, the five-year old children from the DCC were transferred to pre-elementary to meet a total of 25 students in the latter. (The DepEd has promised to give an item to the pre-elementary teacher if there are at least 25 students). According to the DCW, there was coordination between the MSWDO and DepEd regarding this matter.
The pre-elementary classes are held from Monday to Friday with each session lasting for two to three hours. The teacher follows the eight-week curriculum in the pre-elementary classes. The entire school year is divided into two semesters. A child may choose to start in any semester or start from the first semester and finish the entire school year. In the latter case, the student would have gone through the eight-week curriculum twice. In Grade 1, the child is again taught the eight-week curriculum at the beginning of the school year.
The eight-week curriculum has been designed for Grade 1 students at the beginning of the school year. The Grade 1 teacher interviewed said that the children who benefited most from the curriculum were those who have not gone through the day care or pre- elementary.
4.1.3.5 Early Childhood Education: Quality
The DCC is a new building constructed from the municipal budget outside of the ECCD fund. During the visit, the center has not yet been used. It still lacks furniture and classroom décor. However, some of the teaching materials from the old center have been transferred. There were educational charts on topics such as days of the week, weather, months of the year, national symbols, family life, and rights of the child. There were books provided by the ECCD program. The available compact discs were a mixture of English nursery rhymes and Filipino children’s songs. There were a variety of hand- made children’s educational toys such as picture puzzles, memory game, picture lotto, among others, made by the DCW themselves. The DCW complained that learning materials are not enough that she sometimes had to borrow from other teachers. Each child also has on file an accomplished ECCD checklist. This is routinely done for every child in the day care.
The DCW is a college graduate and she has been in the service for the past four years. She replaced the previous Grade 1 teacher who has retired. She has attended on-the- job training on the Day Care Manual in 2004 and training on the new ECCD Revised Day Care Manual in June 2007. The Grade 1 teacher finished Bachelor in Science in Industrial Engineering with 18 units of Elementary Education. She has been an elementary school teacher for 19 years but year 2007 is her first time to handle Grade 1
40
students and to implement the eight-week curriculum while she did not receive formal training on the curriculum, she gained on the topic from her colleagues and supervisor.
4.1.4 Integration and Convergence
The most common understanding of integration is the collaboration of different agencies in implementing of a certain goal such as the ECCD program. They say this integration is evident in the ECCD program because different agencies are involved. However, the actual conduct of specific programs has not changed after the implementation of ECCD. One difference is that the different agencies have become aware of the activities of the others. This decreases the chance of duplication of services. There is also sharing of data between agencies as exemplified by the weight and height measurements data by the Municipal Nutrition Action Office (MNAO) being utilized by an NGO to determine the target population. Perhaps the greatest impact of ECCD is the provision of funding for services that benefit children aged zero to six years. Such investment by ECCD to this age group has increased the awareness of different agencies and service providers on the importance of the normal growth and development of children if they are to become productive individuals.
This idea of integration in ECCD was shared by the members of the PECCDCC and MECCDCC. However, majority of the ECCD council and the service providers in the barangay do not have an idea of what integration is. Some do not even know what ECCD is about; some heard of ECCD only during the interview. Although some of them have attended an ECCD orientation, the information has not been shared with the rest of the persons involved.
The household interviewed has seven members. Three are children aged six months old, one year old, and four years old. Other members living in the household are the children’s parents, grandfather, and uncle. The mother was the informant during the interview. She has had prenatal check-up and vaccination against tetanus during her pregnancies. All children were registered at birth. All of them were breastfed exclusively for about one to two months. All of them were also fully immunized under the EPI program. However, the father has not participated in any ECCD program. The parents have not attended any PES or ERPAT. The mother has expressed the need for advice on family planning, education on how to take care of children, and knowledge on tending to a sick child. Table 4.1.4. Knowledge and attitude of service providers Knowledge and attitude statements Score Children’s rights 0.90 Maternal and child health KAP statements 0.63 Cognitive development 0.54
4.1.5 Monitoring System
The PECCDCC conducts a monthly monitoring of the ECCD programs in the province. They visit the ECCD areas and interview beneficiaries to evaluate the programs. Data are also validated to assess the program based on the approved project proposal. The individual agencies are responsible for evaluating their respective ECCD activities. Each agency has its own monitoring instrument for the purpose. At the time of the interview, the MECCDCC was still in the process of designing a common tool for monitoring and evaluation of the implementation of ECCD programs. Until such tool is designed, the individual agencies continue to utilize their respective reporting and monitoring forms.
41
4.2 The ECCD in Leyte
4.2.1 Profile
Leyte is one of the six provinces in Region VIII and it is classified as a first class province. It has a total land area of 5,712.80 square miles divided into five congressional districts. It has 2 cities, 41 municipalities, and 1,641 barangays (76.5% rural and 23.3% urban). It is bounded by Carigara Bay in the north; San Juanico Strait and the Leyte Gulf in the east; Southern Leyte in the south; and Camotes Sea in the west. The province is mainly agricultural with some manufacturing industries.
Sta. Fe is one of the 41 municipalities in the province with a land area of 81.90 sq. km. It is composed of 20 barangays and is classified as a 5th class municipality. It is bounded in the north by Tacloban City; on the south by the municipality of Pastrana; on the west by the municipality of Alangalang; and on the east by the municipality of Palo. The municipality is located along the highway. Thus, it is quite accessible from Tacloban City. However, it has far-flung barangays which can be reached by a single motorcycle.
The major source of income of households is farming with rice and coconut as main crops. As of 2005, the total population was 15,384 which increased from 13,695 in 1995. With an annual growth rate of 2.32 percent, the population is expected to increase to 20,301 by 2009. The population density is also expected to increase from 167 persons per square km. to 247 persons per square km.
There is no hospital in Sta. Fe but it has one municipal health unit which is run by one doctor, one nurse, three midwives each one assigned to cover seven barangays, one dentist, one sanitary inspector, and two medical technologists. There are 42 BHWs who are considered as the frontliners in the delivery of health services. In Barangay Milagrosa, there is only one BNS. It was also reported that there is a disproportionate number of health workers vis-à-vis the population. At present, each midwife is covering more than 5,000 individuals spread over six to seven barangays.
Based on the 2007 Annual Operations Plan of the Municipal Health Office (MHO), about 87 percent of mothers had prenatal check-up. Only 88 percent of the children were immunized because the mothers failed to bring their children to the health center due to work, fear of side effects/reactions of children, shortage of syringes, and no master list of children and log book for missed children, and failure to follow-up. The municipality also reported a high prevalence of malnutrition at 25 percent with an OPT coverage of about 86 percent.
4.2.2 ECCD Structure and Management
4.2.2.1 Planning
The implementation of the ECCD in Leyte started with the conduct of two workshops (September 1-2, 2004 and November 4-9, 2004) initiated by the regional office of the DSWD/CWC. The PSWDO selected two municipalities while priority barangays in each municipality were selected by the MCPC. The province had no participation in the selection and prioritization of the barangays. For a municipality to be involved in the ECCD program, the following requirements had to be complied with: 1) Memorandum of Agreement, 2) investment plan adopted by the Sangguniang Panlalawigan, 3) approved WFP, 4) bank certificate as proof of the deposited counterpart, 5) appointment or
42
designation of an ECCD officer, 6) EO reorganizing and strengthening Local Council for the Protection of Children (LCPC), and 7) letter of request. At the preparatory stage, one of the target municipalities failed to submit the required counterpart on time which affected the other municipality that was able to remit on time. The PSDWO wrote a letter to the mayor to inform him that non-compliance could lead to giving the slot to the next municipality in line.
The two municipalities, Sta. Fe and Matag-ob, were selected by the PCPC using three criteria: 1) incidence of malnutrition, 2) non-participation in elementary school, and 3) non-completion in elementary school. The PCPC used the 2002 OPT and National Statistical Coordination Board (NSCB) data as basis. Sta. Fe ranked 2nd in criteria 1 and ranked 1st in the other two. On the other hand, Matag-ob ranked 7th, 2nd, and 8th in the three criteria, respectively. The ECCD plans prepared by the two municipalities were consolidated by the PCPC into a provincial ECCD plan with additional activities necessary for the management, i.e. communication, monitoring, advocacy, training, among others. On the other hand, the barangays were selected by the MCPC together with the PCPC.
Planning at the provincial level was done through the conduct of workshops. The Regional Sub-committee for the Welfare of Children (RSCWC) organized the ECCD planning workshop which was held in Villa Hotel, Ormoc City. Selected members of the PCPC, MCPC, and BCPC were invited to attend. The workshop included several sessions on 1) Framework of Child-Friendly Local Governance and Situating Child Rights in Local Development Planning, 2) Situation Analysis, 3) Defining Strategic Directions Until 2025: Vision, Mission, and Goals, 4) Defining Medium-Term Strategies, Directions, and Actions; 5) Monitoring and Evaluation, and 6) Action Planning. The RSCWC organized the workshop in coordination with the provincial government headed by Governor Carlos Petilla.
The total budget needed to implement the plan for three years is PhP21,986,100. The funds would come from the LGU (PhP4,125,000), CWC (PhP16,500,000) and municipal/barangay funds (PhP1,361,100). For 2006, the approved WFP showed a budget of PhP7,311,890; 80 percent of which came from CWC (PhP4,724,632) and 20 percent from the LGU (PhP1,181,158). For 2007, the budget amounted to a total of PhP4,400,000; 30 percent (PhP1,300,000) from the LGU and 70 percent (PhP3,100,000) from CWC.
Assessment was done at all levels using secondary data, i.e. prevalence of undernutrition. The goals/objectives were also set by the PCPC, MCPC, and BCPC during the planning workshops. No additional goals were added or deleted from the national goals. The assessment stage is an important element in the whole planning process. Thus, while using secondary data is practical, these may need to be complemented with other assessment procedures, e.g. FGDs, conduct of strengths, weaknesses, opportunities, and constraints (SWOC). Assessment can be given more time and its own funding. Doing so could reduced disapproved proposals as well as increase confidence in the plans to be submitted as these would reflect the true picture/situation of the area.
At the provincial level, the provincial governor issued EO No. 085 which called for the reorganization and strengthening of the Leyte Council for the Protection of Children. Moreover, the Sangguniang Panlalawigan of Leyte authorized the governor to enter into an agreement with CWC through a resolution (05-282) entitled “A resolution authorizing the Hon. Carlos Jericho L. Petilla, Provincial Governor, to enter into a MOA with the CWC relative to the implementation of the ECCD program in the province of Leyte”.
43
Another resolution was passed, Resolution No. 06-190, adopting and implementing the ECCD investment plan for the Province of Leyte for CY 2006-2008 in the municipalities of Matag-ob and Sta. Fe with a total project cost of PhP20,625,000.
At the municipal level, the MSWDO/ECCD coordinator requested for a meeting of the MCPC and requested proposals per department. Then selected members, i.e. MHO, MBO, Municipal Planning and Development Council (MPDC), engineer, DepEd, and MSWDO attended the workshop held in Ormoc City. The accounting officer was included in the planning but not in the workshop.
At the barangay level, the members of the BCPC responded to the invitation of the municipality to be part of the ECCD program. They said that the municipality identified and prioritized their barangay to be included in the ECCD program. During the FGD, the BCPC members said that while they were able to attend and participate in the planning workshop, they were not informed which of the proposed activities were approved or disapproved. Moreover, at the time of the visit, the BCPC did not have a copy of the plan that was submitted to the municipality and province. Thus, majority of the BCPC members did not know the status of the ECCD program implementation in their barangay.
The BCPC enumerated the needs of the barangay, i.e. renovation of the day care fence, presence of underweight children; renovation of the old barangay hall to become the barangay health station/center (which can be equipped with prenatal equipment, supplies, and information materials); renovation of the day care center since it has no playground (which limits the children’s activities); no electricity, kitchen, water, and lights; and no supply of medicines for simple ailments such as headache and iron supplements. The BCPC conducted meetings to prioritize the identified needs of the barangay; these, in turn, were submitted to the municipal level.
The BCPC was also able to comply with all the requirements including the counterpart of PhP11,200 per year or a total of PhP33,000 for three years. The BCPC during the FGD said that they were willing to give the amount from their Internal Revenue Allocation (IRA) since the barangay would receive more than what they have invested in return.
4.2.2.2 Financial management
According to the ECCD coordinator, the work and financial plan is prepared at the municipal level with technical assistance from the ECCD coordinator and assistant ECCD coordinator and consolidated by the ECCD provincial secretariat. Each LGU is required to provide a yearly counterpart. It takes two months to prepare and process project proposals but the release of funds takes longer.
The funds are disbursed by the Provincial Treasurer to the Municipal Treasurer as cash advance depending on the total amount of proposals submitted and approved at the provincial level following the “no liquidation, no succeeding release policy”. The supply unit of the municipality is responsible for buying the equipment and supplies. But the amount and type of supplies and materials to be procured are based on the approved budgetary requirements specified and requested by the LGU. The equipment, supplies and materials are procured locally when the proposal is approved.
The procurement process includes: 1) proposal prepared and submitted for approval of the LCE, 2) supply unit prepares the purchase request with attached approved proposal, 3) delivery of supplies, 4) inspection, 5) prepare and processing of voucher for payment.
44
The barangay captain said that he liked the present set-up wherein the ECCD money is not released to the barangay for disbursement. This way, he said, there will no questions on how the ECCD money is being used. However, in this set-up, the BCPC will become “powerless”, e.g. they will not know how much money had been utilized and how much money is left. Consequently, they will not be able to determine/assess if there is a need to realign the budget. For instance, the money for supplementary feeding is released from the municipality every week. When the treasurer is out of office, the activity stops due to the non-release of funds which, in turn, results to the unscheduled stoppage of the feeding program.
4.2.2.3 Delivery system
At the provincial level, the PCPC is responsible for the implementation and supervision of the ECCD program in the municipal and barangay levels. On top of the province is the RSCWC, which reports to the CWC at the national level. The CWC is responsible for the development of overall policy and program, setting and dissemination of guidelines and standards, and providing of technical assistance to the LGUs. One of the technical assistance needed at the municipal and barangay levels is the issuance of guidelines/standards on the different services. It is possible that all the guidelines/standards, e.g. building code for DCC, standards for program delivery, can be compiled and issued in the ECCD areas.
While the orientations/planning workshops were held in 2004 and the ECCD plan was formulated in 2005, the implementation started in the fourth quarter of 2006 (October) upon the release of funds. If the plan was implemented on time, the original schedule of implementation was February 2006. With the delay in the release of funds, the activities that are being implemented in 2007 are still using funds from the 2006 release. The delay was due to the revisions in the ECCD plan as well as the need to resolve the issue on cost sharing.
Between the two pilot areas, Matag-ob is implementing the identified activities much faster than Sta. Fe. As of April 2007, more than PhP1M have been released to Matag- ob. In Sta. Fe, implementation has been delayed because of various unexpected problems such as recent death of the municipal nutrition action officer and inability of the municipal ECCD coordinator/social welfare officer to work due to the sickness and death of a son.
4.2.2.4 Service Providers
The personnel involved in the ECCD program can be categorized into three groups, namely: 1) ECCD partners which would include NGOs or private agencies implementing programs focused on children; 2) personnel implementing or providing the services at the local level; and 3) members of the BCPC/MCPC.
In the first group, one NGO (World Vision) was reported to have collaborated with the provincial office but none were tapped or invited to become involved in the ECCD program at the municipal and barangay levels. The NGO provided billboards showing the rights of the child in the 21 barangays of Matag-ob. It is possible that this aspect was not emphasized during the planning workshop; probably at the regional level, this is not practiced; or guidelines on how to implement or accredit new partners have not been issued or are not clear to the LCPCs.
45
In the second group, the service providers are present at the provincial down to the barangay levels. At the provincial level, the ECCD coordinator (designated by the PSWDO) and assistant ECCD coordinator are the prime movers. The members of the PCPC are involved in the assessment, planning, and monitoring of the ECCD program. At the municipal level, the municipal ECCD coordinator (who is also the MSWDO) coordinates the implementation of the ECCD program. The ECCD program frontliners (direct contact with households and children) are the Grade 1 teacher, midwife, BHW, BNS, and DCW. These separate workers provide services on health, nutrition, and preschool education, respectively.
The last group is composed of members of the PCPC, MCPC, and BCPC. The members of the committees are also noted to be the members of the local nutrition committees. As members of the local CPC, they do not receive additional payment or honorarium for work rendered to the ECCD program from the LGU. Moreover, no additional personnel were hired at the barangay, municipal, and provincial level. At the provincial level, an assistant ECCD coordinator was hired and is being paid using ECCD funds. If additional payment or honorarium will be given to the service providers, this will give an impression that the ECCD program is a special project of the government and this could affect the service providers’ enthusiasm and attitude as well as the program’s sustainability.
4.2.2.4.1 Social Welfare Officer
The social welfare officer finds the ECCD goals as realistic and relevant “if given full government support”. She said that the goal is “to ensure that children from birth to six years old receive consistently high-quality care and education so that they can develop their fullest potential”. She is also aware of the legal basis for ECCD as well as the target participants (0 to 6 years old) and gives her full support and commitment. As a result of the implementation of the ECCD program, her work load and responsibilities have increased. At present, she is directly involved with the supplementary feeding which she finds relevant, appropriate, and socially acceptable. Supplementary food is given to underweight children (0 to 6 years old) in barangay Milagrosa, Sta. Fe once a week. She always follows the protocol because “we are subordinates” even though she had not received training for implementing supplementary feeding. Interventions are promoted by conducting meetings with parents and community. She also said that participation in interventions is 100 percent.
The social welfare officer was not involved in the planning and decision-making process of the ECCD program. She does understand that integration is “immersion and oneness”. The nature and extent of participation is “satisfactory” at the community level but there is no collaboration with other private agencies or NGOs. The ECCD has improved the delivery of services by improving the nutritional status of the children.
4.2.2.4.2 Barangay Nutrition Scholar and Barangay Health Worker
The BNS conducts OPT together with the BHW and midwife and assists the DCW in the implementation of the supplementary feeding. The BNS has been working as such for only six months. Thus, she is not able to fully perform the tasks expected of her, i.e. conduct nutrition education which is quite a critical function. She needs training as well as logistical support.
The BHW assists the midwife in providing health care services to a group of 20 to 30 households in a barangay. A law (RA 7883 enacted in 1995) has granted the BHWs hazard and subsistence allowances, educational programs, civil service eligibility, and preferential access to loans (Solon 2006). There are more BHWs (200,000) than BNSs
46
(22,000) in the country. In Sta. Fe, there are 45 BHWs spread over 20 barangays. They conduct yearly OPT, assist the midwife, and follow up clients for immunization, family planning, among others. The BHW is given PhP900 per month honorarium by the barangay.
4.2.2.4.3 Rural Health Midwife
The midwife provides the health care services, e.g. immunization, prenatal care which she believes are relevant, appropriate, and socially acceptable. She provides these services to mothers and children every month when she visits the barangay. She said that only about 4 percent of children and mothers are able to avail of the services due to insufficient funds to fully implement the different health programs. She finds the paper work, e.g. FHSIS and immunization reports difficult. She submits these reports to the nurse every month who is also her direct supervisor and the latter gives her feedback. The midwife is assisted by the BHW in measuring blood pressure and weighing. She has not attended training related to ECCD.
4.2.2.4.4 Day Care Worker
The DCW teaches the preschool children enrolled in the DCC and assists in information campaign for immunization and dental services. She also weighs children enrolled in the day care. However she does not compute the age in months, determines the nutritional status, and implements and coordinates the supplementary feeding program (with 12 enrollees). The DCW is not using the ECCD curriculum and not yet conducting an assessment using the ECCD checklist.
The DCW has been involved in the planning/decision-making because she attended the planning workshop. Based on her estimate, about 90 percent of the population avails of the services offered by the DCC while the rest cannot do so due to their distance from the DCC. On some occasions, some children do not attend class for one week when there is heavy rainfall or when they do not have money for transportation. Information campaign about the day care service might not be as needed as the health services since mothers would enroll their children based on their initiative.
The DCW finds teaching children as the easiest work because it is her main task; while the hardest thing is working with the parents. The parents are difficult to organize and are also busy with work in or out of the house to be involved in the activities of the DCC. The DCW attends meetings at the MSWDO. However, she did not receive training on weighing of children, using the IRS to determine the nutritional status of children, and the conduct of supplementary feeding. She did receive verbal instructions but no handouts or manuals. She was also able to attend a seminar on using the revised manual and on using the new session plan for ECCD. The DCW also have other responsibilities such as being a member of the barangay council. Sometimes, she has a hard time dividing her time because meetings are called when she is teaching.
The DCW is using the integrated curriculum which she learned from the training on the revised manual held last 6-10 August 2007 in Ormoc City. Her travel expenses were shouldered by the barangay. During the training, she received a notebook, ballpen, Manila paper, cartolina, and pentel pen. She also said that she further simplified the curriculum and the activities since there were no materials or books that could be used by the children. Further, she also organized meetings with parents, i.e. twice in 2006. However, very few parents attended the meeting. She would also like to learn more about guiding children’s behavior, children’s development, and use of Internet/computer.
47
The DWC is supervised by the MSWDO who visits the DCC monthly to look at her work during sessions. She likes being “monitored” and “supervised” since she can receive advice. She also submits quarterly report (number of children, drop outs, enrollees, transferees, among others), but she seldom receives feedback. There is perception that discussions are done but no actions are implemented. With regards to ECCD, there is no ECCD form or checklist that is being used.
The current DCW is qualified since she was able to meet the qualifications which are as follows: female, between 18 and 45 years of age; high school graduate; physically healthy; of good moral character; preferably with prior work experience with preschool children; willing to undergo training and accept technical supervision from the MSWDO; must render full-time service for a minimum of two years (UNESCO 2006).
With regards to the need to coordinate with the Grade 1 teacher, the DCW said that DepEd offers pre-elementary education from October to May. The children eligible for Grade 1 in the following school year transferred to the pre-elementary because free notebooks are provided. Consequently, the number of children enrolled in DCC decreases by October.
4.2.2.4.5 Grade One Teacher
The Grade 1 teacher handles two classes in one classroom. She has 22 and 18 pupils in Grades 1 and 2, respectively. She has attended the training on eight-week curriculum and has started to use it. She said that she needs support in developing teaching materials to be used for teaching the pre-elementary class. She also stated that it is quite difficult to teach two classes at the same time but she has to abide by the rule is that one section should be composed of at least 35 students.
The DepEd prescribes the following qualifications and profile for teachers (Education Order 107s, 1989) in preschools: 1) a Bachelor of Science degree with specialization in Early Childhood or Kindergarten Education, Family Life and Child Development or Elementary Education with at least 18 units in ECCD; an allied non-education college degree with at least 18 units of ECCD; 2) male or female, between the ages of 21 to 35 years; 3) training, experience, and interest in working with young children; and 4) certified physically and emotionally fit (UNESCO 2006).
The Grade 1 teacher also implements the Food for School Program implemented last September 2006 which involves giving of 1 kilo rice everyday to Grade 1 pupils. The teacher was of the opinion that the service was appropriate and relevant and all Grade 1 pupils were reached/covered. The direct supervisor is the principal-in-charge. The teachers report their accomplishments every month using Form 2 (Attendance); Lesson Plan/Daily Activity; and Exam (includes the result). The attendance and lesson plan are submitted to the principal. Attendance is submitted monthly while the lesson plan depends on the need. Feedback is usually received through an acknowledgement of the submitted reports/form. The teacher was able to attend the planning workshops and from there received handouts. The three topics that the teacher would want to learn more are on 1) investment programming for children; 2) implementation process and financial management; and 3) action planning.
In general, the various service providers have knowledge on children’s rights, maternal and child health and nutrition, and cognitive development even though they had no training. Among the service providers, the DCW got a perfect score on children’s rights and on children’s cognitive development. The score of the other service providers are Table 4.2.2.4.5 Knowledge and attitudes of service providers ITEMS GOT BNS DCW RHMW
On children’s rights 0.80 0.90 1.00 0.90 48 On maternal and child health 0.75 0.81 0.75 0.75 On children’s cognitive development 0.73 0.82 1.00 0.82
shown in Table 4.2.2.4.5. This could mean that they have other sources of information other than from training, e.g., printed materials. All service providers need more information on maternal and children health and nutrition . 4.2.3 ECCD Accessibility/Quality of Services Delivered
The implementation of the ECCD programs/services is being coordinated by the ECCD coordinator and assistant ECCD coordinator at the provincial level. At the time of the field visit, the assistant ECCD coordinator has not been paid her salary for two months already. Some activities proposed by the LCPCs were disapproved by CWC. For example, as part of its advocacy program, the PCPC has requested for an LCD to be used during trainings and workshops but this was disapproved by CWC. The BCPC said that their request to fence the playground was likewise disapproved.
The ECCD plan includes several program/projects/activities as shown in Table 4.2.3.1.The plan does reflect the need of the two pilot municipalities in health, nutrition, and day care services. Some of the identified areas were similar but others were different particularly for the maternal and child care package. The supplies and equipment identified by the Sta. Fe group included: 1) examining table, 2) weighing scale, 3) stethoscope, 4) sphygmomanometer, 5) scissors, and 6) umbilical cord clamp, among others. This was because the barangay does not have a barangay health station. The midwife assigned to the barangay holds clinic at the barangay hall which also needs improvement. Moreover, the barangay hall is not suitable for prenatal care because of the absence of the necessary supplies and equipment.
Table 4.2.3.1 Summary of accomplishment in the two pilot areas as of 2007 Sta. Fe Accomplishment indicator . Orientation of BCPC on ECCD . Conducted; 85% functionality attained . Procurement of computer table . Part of computer set requested . Supplemental feeding . Ongoing; 85% of beneficiaries increased . Treatment of infectious and other in nutritional status diseases . Ongoing; 100% of children and mothers treated from infectious diseases
The barangay captain, as chair of the BCPC, leads the implementation of the ECCD plan. He also coordinates the implementation of the plan and conducts informal monitoring visits together with some of the councilors. Moreover, the BCPC said that they depend on the “say so” of the MCPC, e.g. what the MCPC gives, they accept, and they wait for the next one. For example, the municipal engineer told them that the construction of the health center will start in September 2007 so they are waiting for it to be implemented. This situation, in addition to the fact that the BCPC did not have a copy of the ECCD plan, shows that the barangay may not be proactive in implementation.
As of the first quarter of 2007, the activities listed in Table 4.2.3.2 were reported to have been accomplished and/or the implementation is ongoing at the municipal and barangay level.
The MCPC FGD participants said that the ECCD helps the LGU in providing services to children. The indigent families in the barangays will be given assistance in terms of medicines and immunization, and supplementary feeding. They expect that the children in the day care centers would have improved nutritional status, increased attendance, and increased number of available learning materials.
49
Table 4.2.3.2 Summary of activities included in the ECCD plan in Sta. Fe Programs Projects/Activities Sta. Fe ECCD advocacy Involves the provision and installation of materials such as / signboards, etc. Social services Capacity building: orientation of BCPCs on ECCD, training / on the revised DCWs manual, parent effectiveness service, basic business management skills training, and skills enhancement Accessing social services: improvement of day care centers, / procurement of day care learning materials, provision of honorarium to DCWs, livelihood assistance, upgrading/procurement of day care facilities and structures, installation of day care recreational/play ground facilities Health/nutrition Treatment of infectious and other diseases (ARI, CCD, / services nutrition, PTB, dengue, measles, deworming) Treatment of PTB on children Maternal and child health care (pre-natal, natal, post-natal) / Immunization / Procurement of dental health facilities and equipment (e.g. / dental chair, anesthesia for children) Health education focused on proper dental care Improvement of the Barangay Health Station to the standard / of Sentrong Sigla, e.g. installation of comfort room, lavatory Women’s reproductive health, e.g. pap smear, breast and / pelvic exam Family planning and health education / Organization/ CPC/BCPC meeting / Management
The MCPC FGD participants also reported that the funds being used in 2007 are still from the 2006 release. The day care center in barangay Milagrosa has not been renovated. But materials are being procured; canvassing was already done. Except for supplementary feeding, nothing much was done due to the election and to the delay in the release of funds.
At the barangay level, the only program being implemented was supplementary feeding. The DCW is given PhP700 to be used to buy foods and this is released and liquidated every week. The allowance for each child is PhP12 per day for five days a week. There were 12 preschool children included in the feeding program. The problem with the weekly release of funds is that when the Municipal Treasurer is out of the office, there is no money to buy food. Consequently, the supplementary feeding stops and resumes when the Municipal Treasurer is present to release funds again. The children suffer from this kind of arrangement because they are supposed to get the food for 90-120 days as scheduled. Another issue is that some of the parents were too busy to do the tasks assigned to them. Thus, the DCW either would do the work for them or find other mothers to act as substitutes. This condition means additional work for the DCW. It could also indicate that mothers are not fully supportive of the program or that other strategies are needed to account for mothers who cannot do their assigned tasks due to work inside or outside the home.
No innovative strategies or interventions or activities were identified and/or included in the ECCD plans at the provincial, municipal, and barangay levels. It is possible that the LCPCs are constrained from being creative and resourceful because of the requirements
50
and because funding is comes from the CWC. Probably a budget ceiling has been set or a set of services has already been identified and enumerated in the guidelines.
Moreover, plans or programs for promoting ECCD were not in place. The P/M/BCPCs had included advocacy activities in the plans, but these were not yet implemented pending release of funds. Moreover, only activities were identified/listed with corresponding budget; these were not really an “advocacy or social marketing plan” with its own set of objectives, strategies, and implementing guidelines.
The family that was interviewed had not heard about the ECCD program and was found to have limited access to health services (midwife goes to the barangay hall once a month); DCSs; and to nutrition programs such as food, seeds for planting, information, communication and education (IEC) materials, and counseling (BNS is newly appointed and had not received training yet). This is a reflection of the access to ECCD services by other households in Barangay Milagrosa which could also be described as limited. For instance, there is no barangay health station; the midwife holds office in the barangay hall which does not have the necessary facilities such as water, toilet, electricity, and room for consultation. The midwife’s visit is limited since she is covering seven barangays. Further, the newly appointed BNS is not performing the expected tasks except OPT. Lastly, Barangay Milagrosa also has no nutrition action plan, indicating that there is no comprehensive action addressing malnutrition problem in the barangay. At the moment, target households have access to supplementary feeding, immunization, day care service, and growth monitoring through OPT. There are some areas in the barangay which are quite far from the barangay hall thus, making access to health services more difficult.
Though limited, the respondent was able to avail of prenatal care services including tetanus toxoid immunization only. Four of her children were provided with medical examination, birth registration, full immunization; two of her children were exclusively breastfed and were able to enjoy extended breastfeeding and complementary feeding. Her children were also able to attend the DCC which she thought should take in children aged four years so that they would learn at an earlier age. She also said that children were not accepted in Grade 1 if they were not able to attend day care.
The ECCD services are primarily being delivered through DCCs, elementary school (Grade 1 entrants), and health centers/barangay health stations. The MSWDO has been responsible for the implementation of the day care system since 1991 when the DSWD was devolved after the enactment of the LGC. It is considered the largest provider of ECE and education services for three- to four-year old children (UNESCO 2006). The operation of the DCC is actually part of the National Preschool Education Program which aims (among others) to upgrade the quality of preschool education to ensure that the children would be ready to enter elementary school. As of 2000, there were 32,787 day- care centers (out of 41,924). In 1998, 26.7 percent of the barangays was found to have access to this program.
Likewise, the MHO is responsible for providing health and nutrition services through the municipal health centers and barangay health stations. These are considered to be the “main service delivery points for decentralized maternal and child health services that complement the group experiences in day care centers” (UNESCO 2006). The municipal health centers are manned by doctors, nurses and midwives. The barangay health stations are staffed by midwives, BHWs, and in some areas, including BNSs.
There is a need to determine the reasons for not accessing health services. Based on the DOH’s Health Sector Development Project, only 70 percent of the poor used health
51
facilities, lower than the middle-income (75%) and the rich (82%) despite a corollary survey showing that 32 percent of poor adults were sick compared to only 19 percent of rich adults. Same report showed that the poorest 30 percent turned to traditional healers 40 percent of the time.
On the other hand, the DepEd (not a devolved department) implements the eight-week curriculum to entrants to Grade 1 who have either graduated from public and/or private preschools or have not attended preschool.
Based on observation, there is a need to establish the links between services and/or to make known the links from one service to another. For instance, the preschool child who is expected to graduate from the DCC should be referred/linked to the Grade 1 teacher (either in the private or public elementary school present in the area). There should also be a referral system between the day care center, barangay health station, Barangay Health Office (BHO), and police, among others. The types of links would probably vary depending on the extent of present or future use of services. As of now, establishing the linkages, especially at the barangay level, is quite feasible since the physical facilities are located near one another. This strategy would probably help concretize the concept of convergence and integration of services at the household level.
The quality of the ECCD services provided in Barangay Milagrosa was assessed in terms of inputs (qualifications of personnel, availability of materials, and facilities) and process (meeting the standards of what and how interventions should be done). The barangay has a total population of 550 with 106 households; 19 pregnant women; 19 lactating women; and 16 children aged 0 to 16 years old.
4.2.3.1 Day care service/preschool education
The quality of day care service/preschool education needs to be improved. The day care center needs to be renovated to include electricity, kitchen, playground (outside), play or activity corners inside the classroom, and additional learning materials. The DCC operates five days a week but with half-day sessions only. Each session would be comprised of supervised play and group activities (arts and crafts, music and movement, storytelling), childcare for personal hygiene, supplemental feeding, learning experiences for early literacy and mathematics, and socialisation experiences to support social and emotional development. The day care worker needs to be trained on the new ECCD curriculum. There is also a need for the DCW to implement the assessment of the preschool children’s developmental status using the Child Development Checklist and to start using the new ECCD curriculum. In the supplementary feeding program, some parents were not participating because of the cropping season. It was also observed that feeding for some children has become a substitute for lunch or dinner. The protocol for supplementary feeding is not being followed.
According to the mother/respondent, her children like to attend day care because they like the teacher and they receive allowance everyday. The children like best the drawing activity. However, the mother does not know of other activities done in the day care, of any assessment made on the children, and how the assessment is done. However, she knows that a child is given one star if she/he needs practice, two stars for ‘good’ rating, and three stars for ‘very well’ rating. She is also not aware or has not been informed of her children’s progress in attending the day care.
4.2.3.2 Health services
52
The quality of health services is relatively poor. There is also low quality of BHS and DCC infrastructures which affects the quality of services delivered to the children, i.e. inadequate materials and facilities. Ideally, a barangay should have a barangay health station with one midwife to provide services. In reality, the absence of a health facility can be a major impediment to the delivery of services, i.e. pre and postnatal care, dental services. Coverage of immunization and OPT were found to be both less than 100 percent. There is also a need to train the health personnel (midwives, BHWs) to become more capable on managing childhood diseases. Moreover, health facilities/infrastructure should be improved and medical supplies should be provided as scheduled. Between a BHW or BNS and DCW, there were more DCW noted than health volunteers.
The midwife holds consultation and provides health services at the barangay hall (located within a compound which includes the day care center that serves as the barangay health station) once a month. The barangay hall has a floor area of 4 x 5 meters and has been used as BHS for 10 years. The barangay hall is described as “bungalow type” with jalousy windows, roof made up of galvanized iron sheets, with concrete walls, and cemented floor. In front of the barangay hall is the highway and in its back is a rice field. Beside the barangay hall is a free space which serves as a waiting area or a playground. The source of water is a deep well. The barangay looks unclean and untidy; it has no provision for garbage, but it has a small toilet. It has one table at the center of the room, one filing cabinet, and one typewriter. A number of clients are served per visit, e.g. 8 to 10 pregnant mothers and 20 lactating women; six children aged one to three years old; five children aged four to six years old; and two children four to six years old; and five adults. There is no annual plan and no budget for its operation as well. Records that were available were target client list (updated); record of live births (updated); family record (not updated); and daily service log. There are no equipment and facilities in the barangay hall, e.g. stethoscope, thermometer, among others. Syringes and sterile needles are brought by the midwife during her scheduled visit once a month.
4.2.3.3 Nutrition service
The barangay nutrition committee has not been organized and no barangay nutrition action plan has been developed. The BNS is newly appointed and has not attended any training yet. She conducts OPT together with the midwife and BHWs and assists the DCW in the implementation of the supplementary feeding. The OPT is a nationwide program aimed at determining the nutritional status (using weight-for-age index) of preschool children so that immediate nutrition assistance could be given to those identified as underweight. The results of the OPT is also used in identifying and planning nutrition programs.
Ideally, nutrition services for children refer to those covered by “PPAN impact programs” such as nutrition education or promotion of exclusive breastfeeding for six months; adequate complementary feeding starting at six months with continued breastfeeding for two years; appropriate nutritional care of sick and malnourished children; adequate intake of vitamin A, iron, and iodine; and food production, among others. Some of these services are probably not being provided given the lack of training of the BNS and the absence of a BNAP. The PNO prepares a nutrition plan funded by the provincial government but this is not being submitted to the Regional Office of NNC.
53
The results of OPT among preschool children and weighing among Grade 1 pupils in barangay Milagrosa in 2007 are shown in Table 4.2.3.3.
Table 4.2.3.3. OPT among preschool children and weighing results among Grade 1 pupils, Barangay Milagrosa OPT results (2007) Result of underweight among Grade 1 students (as of January 2007)
Total number of preschool children: 126 Below normal: 4 Number normal nutritional status: 91 Normal: 11 Number of below normal (BN): 18 Above normal: 0 Number below normal very low (BNVL): 2 Number of overweight (OW): 0 Total weighed: 111 Incomplete immunization: 20
4.2.3.4 Pre-elementary education/eight-week curriculum
The quality (in terms of time and attention to pupils) of the teaching of Grade 1 pupils is constrained by having just one teacher handling two classes (Grades 1 and 2) at the same time. The two classes cannot be separated because of the DepEd rule that each section/class should have at least 35 students. While the teacher is already using the eight-week ECCD curriculum in Grade 1, there is a need for supplies to prepare learning/educational materials.
The Grade 1 teacher should also continue to administer the school readiness test. This test is given to all Grade 1 entrants in public elementary schools to determine children's readiness of four developmental domains: (1) gross motor; (2) fine motor; (3) cognitive; and (4) language. The children are then classified into those that are “school ready” and “not ready”. Students who are "not ready" are made to undergo the eight-week curriculum. Those who are "school ready" are expected to use the Grade 1 curriculum right at the start. This classification and arrangement cannot be implemented in the class observed since the teacher does not have enough time and space to separate sessions for the “not ready” and “ready” children. Both Grades 1 and 2 classes as said earlier are held in the same room. Moreover, the teacher bears the cost of photocopying the school readiness form. The Grade 1 teacher is also burdened with measuring the weight and height of pupils because she does not have the necessary equipment and the training for nutritional assessment.
4.2.4 Integration and Convergence
The ECCD program framework puts importance on the concepts of coordination, integration and convergence of services. In general, these concepts are not fully operational at the local level.
Coordination is important in implementing the ECCD program. It could improve program efficiency, reduce duplication, and maximize the use of resources. Coordination can be done horizontally and vertically. Coordination exists at various levels, i.e. between the chair and members of the LCPCs; among members of the PCPC, MCPC, and BCPC; and from PCPC to MCPC to BCPC. This activity needs funding for activities such as meetings, communication, visits, among others. The strategies used in coordination should also be identified, i.e. meetings, communication through different channels.
54
Coordination is mostly done through meetings of the LCPCs. Relations of the members of the LCPCs with the chairs (governor, mayors, barangay captains) was described as ‘satisfactory’. The linkage from PCPC to MCPC to BCPC was also described as ‘well established’. However, coordination among members of the PCPC, MCPC and BCPC particularly with the DepEd needs to be further defined and strengthened. At the provincial level, the representative from DepEd does not regularly attend the PCPC meetings. At the municipal level, the new district needs to be oriented on his/her role in the ECCD program. At the barangay level, the Grade 1 teacher has to coordinate with the DCW (e.g., more than half of the enrollees to the DCC are abruptly “transferred” to attend the pre-elementary curriculum).
During the meetings, issues on implementation of projects/activities are discussed (e.g., reasons why supplementary feeding was stopped, actions to be taken to improve the construction of the BHS, etc.) However, it is the BC who coordinates with the MCPC and the DCW with the MSWDO.
The concept of integration (“joining up”) of services must be understood by service providers and the households since it helps improve access to, awareness of, and confidence in delivering/availing of ECCD services. By providing the counterpart, the LCE/LGU has shown its commitment to the ECCD program. However, this commitment should be translated into more concrete terms (e.g., the target priority families should be able to receive or access the services that they need at the time that the need these). Moreover, for this to work, there is a need to identify the services that are already being provided and the gap in each service that should be responded to accordingly.
The concept of integration is not uniformly understood and/or its being a component of the ECCD program is not known to all. The PCPC refers to integration as the implementation of services relevant and specific to children that maximizes resources and prevents overlapping of services. The MCPC participants refer to “integrated ECCD services” as “wholesome”; “more on the enhancement of children”; and “similar to coordination where each agency implements its own ECCD related activities.”
There is a need to have one definition of integration (formal and informal) and to explain the where and what (levels) of integration. The approaches of integration being used should also be identified, whether community-based (recognition of the family and community as the natural context of the child), holistic (integrates, promotes and provides for the child’s needs through cluster of services, e.g. health services, nutrition services), or rights-based (rights of the child). Further, there is a need to identify the integrating mechanism, e.g. center-based delivery of services or joint planning, assessment, and implementation.
One possible strategy of addressing this issue is to explain what approach/es are being used to deliver ECCD integrated services, i.e. use of information or referral system, placement of services near one another (barangay hall, barangay health station, day care center are located in one area in the barangay), and pointing out the link between the services provided from the barangay health station to day care center to elementary school.
A consolidated review at the household level shows that the family was able to receive routine services (not funded by ECCD), such as preschool education from the day care center, and immunization, vitamin A capsule, and prenatal care from the health center. The family also received supplementary feeding from the ECCD program funded by the ECCD.
55
The family is composed of the father, mother and five children; two of whom are aged 4 years old and 10 months. The father works irregularly as a “mason” and occasionally sells coconut salad while the mother tends to the sari-sari (variety) store. The mother has more responsibilities than the father (Table 4.2.4.1). Some responsibilities are also shared by the father and mother but nobody waits for the children while the latter are in school. Either the parents lacked time and would rather use the waiting time for more productive activities or they really felt no need for waiting. The shared responsibilities of the parents, however, showed the importance of education in their family life as they spent time teaching and helping the children with their lessons.
Table 4.2.4.1 List of responsibilities of mother and father Responsibility of father Responsibility of mother Shared responsibilities . teaching children their . laundrying/ironing of . teaching children homework clothes homework . helping children with their . bringing kids to school . helping children with their homework . teaching homework homework . putting children to sleep . preparing meals for . buying food . buying food children . feeding the children . buying food . taking care of children . getting health services for children, e.g. immunization, VAC capsule, iron supplements . bathing children . helping children with their homework
In terms of parenting, time is spent with the children in doing some activities together such as: 1) preparing the children’s meal, 2) playing with the children, 3) taking children to and from school, 4) helping the children with their homework, 5) exchanging/telling stories with the children, and 6) sleeping. Activities which are not done together with the children are 1) feeding the children, 2) taking the children for strolls or outings, 3) working for pay, and 4) participation in community organizations.
The respondent believes that it is better and easier to discipline the children when they are at the right age of 8 to 10 years old. When children behave, they reward them with food (fruits), praises, and hugs/kisses. These are done so that the child would persevere and get inspired to behave well. However, they do hit their children when they misbehave especially when they don’t listen to advices. Parents teach the values of being God-fearing, helpful unselfish, and respectful to elders by frequently reminding their children of these values. They would like to see their children finish their education, learn how to socialize with people, and praise God.
The respondent tries to protect her children by selecting their printed reading materials and by minimizing the exposure of children when they (couple) have arguments/confrontations. The family does not engage in neighborhood activities because they do not know how to play bingo and other forms of gambling. Rather, they encourage their children to attend religious activities and engage in worthwhile undertakings like playing musical instruments and joining in sports.
The mother had six pregnancies but one child died at birth. In all her pregnancies, she availed of prenatal care from the BHW. She also breastfed two of her five living children for four months. She decided to breastfed her children because of limited money to buy
56
milk formula. She started complementary feeding with foods like vegetable soup or fish, cereal (e.g., Ceralac) when her children were eight months old. The frequency of feeding was eight times a day, which is relatively high. To prevent the children from getting sick, the mother 1) gives them a bath (about five minutes spent with child), 2) sterilizes feeding bottles, 3) buys water for drinking (PhP2/container), and 4) ensures having a toilet inside the house. She also feeds her children with mango, biscuit and soft drink (e.g., Royal) when they are sick.
Parents especially the primary care giver should be taught how to prepare food since they are the ones who purchase and provides food to the preschool children. They make decisions in behalf of the children. Thus, poor parenting skills related to nutrition (e.g. poor weaning practices) could exacerbate the problem on nutrition among preschool children. Studies have shown that children under five years have a greater demand for nutrients and energy to support the body's requirements for growth and development than at any other time throughout their life cycle (Taylor et al. 2004).
The respondent has minimal knowledge and awareness and different perceptions on children’s rights, maternal and child health nutrition, and cognitive development (Table 4.2.4.2). The mother was not able to provide the correct answer to the following statements:
1. A child with disorder is better kept in the house than being enrolled in the school/DCC; 2. When a newborn child is healthy and without problems, there is no need to bring the child to the center or clinic for check-up; 3. Dark green and leafy vegetables are good for the eyes; 4. It is possible for a pregnant woman with goiter to give birth to a mentally retarded child; 5. Children with measles should not be given vitamin A capsules; 6. The Sangkap Pinoy seal in food products indicates that the price is discounted; 7. Children who are afraid of their parents behave better; 8. Children learn faster if the teacher is strict; 9. It is not good for a child to ask a lot of questions; and 10. Children start learning only when they begin school.
Table 4.2.4.2. Knowledge and attitudes of service providers Knowledge and attitude statements Score Children’s rights 0.90 Maternal and child health KAP statements 0.63 Cognitive development 0.54
4.2.5 Monitoring System
At the provincial level, the PCPC included a mid-term review and monitoring visits in the place. The provincial ECCD coordinator and one technical staff conduct the monitoring visits. The ECCD provincial team also conducts monitoring visits accompanied by the RSCWC focal person and/or ECCD regional coordinator. They provide verbal feedback to the mayor and to the municipal ECCD coordinator as well as to the regional office and PCCD team. Because of the feedback during the monitoring visits, concerns are immediately acted upon. The ECCD coordinator has devised a monitoring tool to facilitate the recording of the results. However, no management information system has been established at all levels. No prescribed monitoring tool has also been prescribed for the barangay, municipal, or provincial levels.
57
At the municipal level, the MCPC conducts monthly monitoring. Funds for these visits have been included in the plan. During the monitoring, the MCPC learns of issues on implementation at the barangay level. For instance, some mothers are not able to buy the food to be used in the feeding program (their assigned tasks) since they do not have money for fare going to the market. Some mothers do not cook the food to be served to the children because they are either busy or they feel that they are always the ones cooking. The MCPC inform the chair of the MCPC and BCPC on such issues.
At the barangay level, the BCPC chair and councilor monitors the implementation of ECCD activities, e.g. supplementary feeding done in the DCC. However, this is done informally (i.e. mainly observation, doing unplanned visits) and no monitoring tool is used. The DCW also submits reports on the supplementary feeding activities to the MSWDO and the MNAO, and gives a file copy to the barangay. The DCW contends that the BCPC knows the status of the supplementary feeding’s implementation since the child of one of the councilors is among the beneficiaries.
4.3 Province of Davao Oriental
4.3.1 Profile
Davao Oriental lies on the Southern section of Mindanao. It is bound by the Pacific Ocean in the east; by Agusan del Sur and Surigao del Sur in the north; by Davao Province in the west; and the Davao Gulf and the Celebes Sea in the south. Its geographic location follows the highly irregular southeastern coast of Mindanao facing the Pacific Ocean from Cateel Bay down to Cape San Agustin. The topography is characterized by extensive swamps and lowlands.
The province has a total land area of 516,446 hectares representing 16.26 percent of the total land area of Region XI. It has 11 municipalities divided into two districts. District 1 comprises Baganga, Boston, Caraga, Cateel, Manay, and Tarragona. District 2 includes Mati, Banaybanay, San Isidro, Lupon, and Governor Generoso.
The Municipality of Governor Generoso is located in the southernmost tip of the Philippine archipelago. It is bound in the north by the Municipality of San Isidro; in the west by Davao Gulf; and in the east by the City of Mati, about 75 kilometers away from Governor Generoso. The terrain of the municipality is characterized by tapering of rolling hills and green plains. With 30,295 hectares of land, the municipality ranks ninth of the 11 municipalities comprising the province of Davao Oriental.
The municipality is shaped like the body of a shrimp. It is composed of 20 barangays, 14 of which are coastal barangays. Barangay Nangan, the barangay chosen for this study, is a costal barangay.
Barangay Nangan is located 27 kilometers from the town proper of Governor Generoso. Barangay Nangan is an agricultural barangay (70% of its land is devoted to agricultural production) wherein coconut is the major crop. Other crops grown include banana, corn, mango, coffee, root crops, cacao, and other fruit trees. 4.3.2 ECCD Structure and Management
4.3.2.1 Planning
58
Orientation on ECCD took place on July 21, 2004 when the UNICEF and CWC representatives visited the province of Davao Oriental. Highlights of the orientation included the introduction, presentation of the goal, vision and mission, interventions, funding scheme, monitoring and evaluation of ECCD, and points to consider in the preparation of the plan. The pointers highlighted the need to: 1) prioritize the implementation of activities based on urgency and long-term impact, 2) pool activities where resources are limited, 3) ensure that people involved in the implementation are fully aware of the objectives of ECCD, 4) make action steps (what to do, who to do and when to do) for big activities, and 5) take care on over committing resources.
After the orientation, the technical working group prepared the investment plan on August 11, 2004 at the PSWDO in the province. Based on the plan, ECCD will be implemented in all municipalities and their corresponding barangays in three phases. The prioritization was based on the level of malnutrition and suggestion from the Governor and the consultant of the Provincial Committee on Women and Children. The priority municipalities for the first year of implementation included Boston, Governor Generoso and Baganga; the three municipalities of Lupon, Caraga, and Manay and the City of Mati for the second year; and the remaining four municipalities of Banaybanay, San Isidro, Tarragona and Cateel for the last year.
As an ECCD recipient, the province prepared several documents which were required by the CWC. The first document passed was the EO which enabled the creation of the PCPC. Others included the Provincial Development Plan for Children, Resolution of the Sangguniang Panlalawigan allowing the provincial government to enter into a Memorandum of Agreement with the CWC, ECCD WFP, investment plan, and the MOA. For its financial contribution, the province provided the 30 percent equity.
4.3.2.2 Financial management
The provincial government handled the disbursement of the ECCD funds. Only the money allocated to the rehabilitation of DCCs and RHUs were directly issued to the Barangay Captain. Moreover, there were claims that government rules and regulations in the disbursement of fund were not followed. The bidding for supplies and materials were not conducted; instead, cash advances were requested.
4.3.2.3 Delivery system
The PECCDCC, headed by the Governor, is responsible for the implementation of the ECCD programs and projects. The technical working group, directly under the Board Member who is the chairperson on Women and Children, is currently coordinated by the ECCD Officer who is the Assistant Provincial Health Officer.
When the PECCDC was formed, it, in turn, created a technical working committee. The technical working committee is composed of members designated by the members of the PECCDC to carry out their functions. It has only four members despite efforts to include other concerned units of the province. Specifically, the four members came from the MHO, Nutrition Action Center, DILG, and PPDO. The representative from the PPDO was designated as the Provincial ECCD Coordinator by then Governor Maria Elena Palma-Gil.
A Provincial Office for ECCD was created under the Office of the Governor. The ECCD Assistant Coordinator mans the Office as the ECCD Coordinator is based at the PPDO. There are currently five staff stationed at the ECCD Office. There are other positions
59
created when ECCD started in the province but are still vacant. These include roving bookkeeper, encoder, draftsman and engineer.
The provincial government hired municipal and barangay ECCD coordinators (MECCDC/BECCDC) while supplemental feeding was ongoing. For its first year of implementation, every barangay had BECCDC, which was reduced to one barangay coordinator for every five barangays during the second year. The salary of all the ECCD staff, excluding the ECCD Assistant Coordinator, was charged to the budget of the province outside of ECCD equity.
The MECCDC is mainly responsible for monitoring the feeding and weighing activities in the barangays. The consolidated report of these activities is forwarded to the Provincial ECCD Office for submission to CWC. A copy of the report is also submitted to the MCPC. The MECCDC receives the supplies and materials for the feeding program. For their part, the BECCDCs are hired to monitor the supplemental feeding program in the barangay. Both MECCDC and BECCDC are hired for six months while supplemental feeding is ongoing. The MECCDC can be rehired in the other municipalities scheduled for the second and third years of implementation.
At present and with the new Governor, the ECCD Provincial Office has four support staff; three were hired after the recent election while another clerk was on detail from the Office of the Provincial Veterinary Office. There is uncertainty whether MECCDC and BECCDC will be hired.
The ECCD organizational structure in Davao Oriental is quite different from the other provinces included in the study. As noted earlier, planning was highly centralized, thus all the activities are being coordinated at the top. An advantage of this set-up is the well- organized documentation, particularly of the feeding and weighing program. The BECCDC keeps the record of all the supplemental feeding which is then forwarded to the MECCDC for consolidation at the municipal level, then forwarded to the PECCD Office.
Corresponding MCPC was organized at the Municipal and Barangay levels despite the fact that planning and implementation was done at the province. The Municipality of Governor Generoso passed Executive Order 09-2004 Series of 2004 merging the MCPC and the ECCD Coordinating Council. This was done to avoid confusion and duplication of similar council/committee in the LGU with the MCPC as the umbrella organization for all programs for children. The MCPC is headed by the Mayor with the Sangguniang Bayan members who chair the Committee on Social Welfare and Development and Committee on Women Affairs. The other members are the SK Chairperson; Municipal Local Government Operation Officer; Municipal Planning and Development Officer: Municipal Social Welfare and Development Officer; Municipal Treasurer; Chief of Police; Municipal Nutrition Aid; DepEd North and South District Supervisors and an NGO representative as member (Figure 4.3.2.3).
60
Corazon N. Malanyawon Governor-Chairperson
Delfin B. Miones, Board Member Vice-Chairperson
Technical Working Group
PNO PHO Provincial ECCD PSWDO DILG Luz P. Salvacion Coordinator Roseny N. Casicnan Ma. Cerenia Sunggay Dr. Joy S. Sanico Cora P. Son
Assistant ECCD Coordinator Myla Villa M. Aquino, RSW
Roving Bookeeper Encoder Clerk Draftsman Engineer Glenn B. Morales Salvador Bijis II
Municipal ECCD Municipal ECCD Municipal ECCD Municipal ECCD Coordinator Coordinator Coordinator Coordinator Lupon Mati Manay Caraga
Figure 4.3.2.3 Provincial ECCD Coordinating Committee
Despite the many members, the Committee was reported not functional for several reasons. Only one or two members of the committee are actively participating and there has never been a regular meeting of the committee. Furthermore, the province-hired MECCDC coordinated and monitored the ECCD activities in the barangays and prepared the needed reports which are then certified by the Mayor before these were forwarded to the PECCD Office.
A corresponding BCPC was organized at the barangay level. The BCPC was headed by the BC with the Barangay Councilor on Family and Children, DCW, BHW, Chief of Tanod, SK Chair, and PTCA as members.
The absence of committees is another demonstration of the inconsistent implementation of ECCD in the province. Committees for ECCD implementation from the province to the municipality to the barangay were not created.
As noted earlier, to officially signify the start of the program, a MOA was signed between CWC and the Province. In turn, a MOA was drawn between the province and the municipalities covered in the first and second years.
4.3.3 Accessibility/Quality of ECCD Services
The interventions followed the programs indicated in the ECCD Act with supplemental feeding as its banner activity. Other interventions included provision of health and nutrition supplies and materials, deworming, livelihood program, livestock program, renovations of day care centers/rural health units, capital assistance to day care parents
61
and provision of day care center leaning materials. Specifically, the interventions are grouped as follow (Table 4.3.3.1):
4.3.3.1 Support service delivery
Included in the group of programs/projects are nutrition education; upgrading of barangay health service and barangay health center for primary health care; growth and monitoring and promotion; deworming; micronutrient supplementation; and supplemental feeding.
The Technical Working Group (TWG) decided that three barangay health stations for every municipality would be renovated. Thus, 33 were indicated in the investment plan.
Table 4.3.3.1. Support service delivery, Governor Generoso, Davao Oriental Program/Project Brief Description Beneficiary Lead Office Nutrition Pabasa sa Nutrition 15,155 mothers of 0-6 PHO Education yrs old children Mothers’ Class DepEd Breastfeeding & Counseling Upgrading of Provision of BHS/BHC PHO BHS/BHC for sphygmomanometer primary health care Provision of 120 pieces Salter 0-6 yrs old children Weighing Scale Provision of 120 pieces Pregnant Mothers Bathroom Weighing Scale Rehabilitation of Repair of BHS 33 BHS BHS Growth Monitoring Provision of ECCD Checklist & 15,155 children 0-6 yrs PHO/MHO/ and Promotion Nutrition Facts Booklets old BHS Deworming Provision of Deworming BNVL children 2-6 yrs PHO/DepEd old Micronutrient Provision of Vitamin A 3,245 children 0-6 yrs Supplementation old Provision of vitamin Iron 3,245 children 0-6 yrs old Supplemental Hot meals 3245 BN and BNVL PHO/DepEd/ Feeding children 0-6 yrs old DepEd
62
4.3.3.2 Establishing and institutionalizing the system
This component deals with activities on the briefing of the organization of the LCPCs in all levels and provision of advocacy sessions on ECCD to Sangguniang Panlalawigan /Sangguniang Bayan/BC/LCPC (Table 4.3.3.2). Table 4.3.3.2. Components of system establishment and institutionalization, Gov. Generoso, Davao Oriental Program/Project Brief Description Beneficiary Lead Office Briefing the Strengthen the operation of 11 municipalities DILG/ organization of the LCPCs in all levels 183 barangays PSWDO/ the LCPCs in all levels LGU
Provision of Improvement and well- 100% of SP/SB/Brgy DILG advocacy session informed officials officials and LGU on ECCD to improved KAS SP/SB/BC/LCPCs
4.3.3.3 Capability Building
Training of service providers and provision of livelihood activities to beneficiaries are enumerated under this group of intervention. Examples of training programs are: training of Grade 1 teachers on the eight-week curriculum; training of health personnel on IMCI, IRS; upgrading of DCW on the new manual and ECCD checklist; and upgrading of parents and service providers on PES incorporating VAWC and ERPAT. Under the livelihood component are skills training of parents on backyard gardening, poultry, piggery, and goat raising. Provision of capital assistance to parents engaged in food processing for livelihood is also included.
Table 4.3.3.3. Capability building for service providers and provision of livelihood activities to beneficiaries. Program/Project Brief Description Beneficiary Lead Office Training of GOTs on Teaching Staff and Production of Grade 1 Teachers DepEd eight-week Teaching Materials curriculum
Training of Health Training in IMCI (1st Yr only) MHO, PHN, RHMW PHO Personnel Upgrading of DCC Enhance RS Day Care Worker Day Care PSWDO Workers Manual/ECCD Checklist Officers/Accreditors and Day Care Workers
Upgrading of DCC PES Training Incorporating VAWC MSWDO and DCWs PSWDO Parents and Service and ERPAT Providers Enhancing Livelihood Parents’ Skills training on Livelihood Parents with below normal OPAG/PNO Skills for Parents PS Livelihood Faith Backyard Programs Vegetable/Poultry/Piggery/Goat Raising Provision of capital assistance to Organized Day Care Parents PSWDO parents engaged in food processing for livelihood
63
4.3.3.4 Protection
There are only two activities under this intervention: the upgrading of day care centers and the provision of learning materials. Similar with the plan for the rehabilitation of BHS, only three DCCs for every municipality will be allowed for renovation.
Table 4.3.3.4. Programs for day care centers Program/Project Brief Description Beneficiary Lead Office Upgrading of Rehab of Day Care Centers Pre-schoolers in 326 PSWDO Day Care and Parent-Child Development DCCs Centers (DCCs) Programs
Provision of 326 DCCs DCC Learning Materials
4.3.3.5 Planning and Management
This last component covers the setting up of database and management information system (MIS); meetings at the provincial, municipal and barangay levels regarding ECCD, such as monitoring evaluation, PIR; and acquisition of computer set for documentation purposes.
Table 4.3.3.5 Planning and management programs Program/Project Brief Description Beneficiary Lead Office MIS/Documentation/Data Monthly updated and accurate ECCD Council/Pilot PPDO & Banking information Municipalities ECCD Council Computer set Equipment/facility for data ECCD Personnel ECCD encoding Council PCPC meeting Quarterly Council Member PPDO & ECCD Council MCPC Meetings Quarterly
TWG Meeting Monthly TWG ECCD Council
Monitoring Evaluation 2nd/4th quarter Gov Gen. Boston, and PIR Baganga
Financing for all the activities was estimated at PhP23,570. The national ECCDCC will shoulder 70 percent of the total budget while the remaining 30 percent will be the share of the LGU. As indicated in the provincial investment plan, the total amount was almost equally divided into three years of implementation
4.3.3.6 Accomplishments
64
The accomplishment is divided into first and second years. Nearly all the activities listed in the work and financial plan for the first year were implemented, although there was a big lag between the ECCD’s introduction and implementation in the province. The lag delayed the project’s implementation for the second years, and this was further held back by the holding of election in 2001. The 2007 barangay election will also affect the implementation of the ECCD. The third year of implementation should have been started, but as of September 2007, the project has not started yet. The new Governor was asking for a complete audit of the first two years of the ECCD project before approving its continued implementation.
4.3.3.6.1 Health component
For the initial year, all the nine rural health units in the identified barangays have been renovated (Table 4.3.3.6.1). These health centers were also provided with equipment/materials, including: refrigerator, mechanical bed, steel filing cabinet, office table, office chair, sphygmomanometer, white board, and stand fan. All barangay rural health stations information, communication and education of the three municipalities included in the first year of implementation were also provided with sphygmomanometer, Salter weighing scale, bathroom weighing scale, ECCD health growth Table 4.3.3.6.1. Rehabilitation rural cards, vitamin A, iron, and deworming health station by municipality, Davao pills. Oriental Albeit small, the renovated RHU is well Municipality/ Barangay ventilated and well lit because of the Baganga Batawan big windows. It has a consultation Baculin room and a waiting area for the Kinablangan patients. The RHU is generally clean Sibahay including the surroundings. However, Boston Cauwayanan the room which functions as kitchen a Cantilan and the room for ligation and vasectomy were quite crowded. The Nangan Governor RHU has piped water and electricity Tamban Generoso and filled with equipment and Tandang Sora materials purchased under the ECCD project.
As mentioned earlier, the identification of the RHUs for renovation was identified at the provincial level in consultation with the barangay officials and rural RHMWs, BNSs, and BHWs. For Barangay Nangan, the check amounting to PhP63,000 was issued directly to the Barangay Captain. The monitoring of the renovation was done by the Provincial ECCD-based engineer. As such, the municipality did not have any participation which was in opposition to what was being espoused by the ECCD project. This is the downside of the project implementation. Nevertheless, the barangay council headed by the barangay captain has taken the challenge and proven its capability to supervise well the rehabilitation (Box 1).
4.3.3.6.2 Supplemental Feeding
The 120-day supplemental feeding for six months officially started in November 2005 and ended in May 2006. Children younger than two years old were supplied with Nestogen mild while children two to six years old were fed with a hot meal. As planned, the supplemental feeding for all the barangays of the three municipalities of Baganga, Boston, and Governor Generoso was implemented simultaneously. A total of 3,008
65
children coming from 49 barangays were fed. Originally, hot meal was provided for the supplemental feeding with ingredients such as chicken, rice, and egg. These ingredients were procured in bulk in the province by the Provincial Nutrition Officer and then distributed to the different municipalities, also in bulk. The MECCDCs, in turn, accept these supplies at the municipality with the understanding that the BHW would pick them up for the scheduled feeding. Because of the lack of freezer, there was an occasion when chicken were spoiled while eggs were broken due to bad roads. To solve the problem, the province provided a chest freezer.
Renovation of Barangay Nangan Rural Health Unit
Barangay Nangan is one of the six barangays identified by the Provincial Technical Working Committee whose Rural Health Unit has to be renovated/rehabilitated under the ECCD. The cost of repair was PhP63,000 which was directly transferred and to be managed by the Barangay, particularly the Barangay Treasurer. The Barangay Captain supervised the construction. From time to time, the engineer from the ECCD Provincial Office monitored the construction.
To save money for the building materials, the Barangay Treasurer and concerned members of the Barangay Council canvassed the construction materials in Davao City and had them transported to Barangay Nangan. They also accrued savings from buying trees within the barangay and had them sawed into lumber. Their savings amounted to PhP16,000 which they have requested to be used in buying the motor for the water pump and curtains for the RHU.
During the third month of the Table 4.3.3.6.2.1 Comparison between hot meal and choco milk supplemental feeding, the meal Menu Advantages Disadvantages was changed to choco milk Hotmeal Heavy in weight Food storage Different menu Far distance feeding. The daily everyday from the feeding appropriation per child was Easy to conduct center composed of rice, chocoquick, mother’s class Tiresome and B-sugar which was then during the Not easy to cooked similar to feeding prepare Most mothers Delivery of food “champorado”. It is estimated were interested supplies to that the value of meal per child Easy for barangay in was about PhP12. In one rehabilitation of terms of report of the MECCDC, there malnourished transportation was a comparison between the children Chocomilk feeding Easy to prepare hot meal and the choco milk Some of the Division of labor to parents want to feeding (Table 4.3.3.6.2.1). service providers get their share Choco milk feeding was easier (clustering) during weekend to prepare; however, the in order to feed recovery from malnutrition was all their children longer when compared with the at home hot meal feeding. Spoilage Not easy for Parents participated in the recovery feeding program by bringing firewood, dishes, and other utensils as well as in the actual cooking. It was also reported
66
that mothers of 18-month old children were provided with Nestle powdered milk. This was not included in the ECCD work and financial plan.
To monitor the effect of the supplemental feeding, weighing of children were weighed every three months. A comparison Figure 4.3.3.6.2.1 Nutritional Status of pre-school of the nutritional status of children children, Barangay Nangan: 2005 and 2006 during the first quarter of 2005 and 2006 revealed an interesting 90.00 pattern. Overall, there was an 80.00 improvement in the nutritional 70.00 status of children, particularly 60.00 50.00 those in the below normal 2005 40.00 category where the reduction was 2006 most noticeable (Figure 30.00 4.3.3.6.2.1). There was also a 20.00 reduction in the percentage of 10.00 0.00 children in the below normal very Below Normal Below Normal Normal Above Normal low category but not as much as Very Low Nutritional Status that of the below normal low category.
Examining the change in nutritional status by age group also revealed an interesting pattern. The highest improvement in malnutrition occurred among babies where below normal very low nutritional status was completely eliminated in 2006 (Table 4.3.3.6.2.2). This was followed by improvement in the nutritional status among children aged 48-59 months in the below normal very low with 89 percent reduction. Meanwhile, in the below normal low (BNL) status, the highest reduction occurred among children aged 36 to 47 months. What is bothersome is the persistence of the high percentage of below normal very low (BNVL) children aged 60 to 71 months. Another observation was that across age groups, the reduction in the below normal very low was less when compared with the children in the below normal low category. These findings highlight the need for longer supplemental feeding for those children in the BNL category and that Table 4.3.3.6.2.2. Percent change in the hot meal feeding should be preferred nutritional status of children by age, over the choco milk feeding. Or Barangay Nangan: First quarter 2005 and perhaps a different menu should be tried 2006 (in months) specifically for children suffering from Below BNVL. Normal Below Age (in Very Normal months) Low Low Normal The supplemental feeding time also 0-11 -100.00 7.32 0.77 gave opportunity for the service 12-23 -25.84 -48.66 14.20 providers to conduct mothers’ classes. 23-35 -31.40 -24.53 7.38 They have conducted two sessions of 36-47 14.42 -74.91 23.30 mothers’ class during the six months 48-59 -88.64 -65.91 29.02 that supplemental feeding was ongoing. 60-71 96.60 -41.02 4.46 The topics discussed were on immunization, deworming, and family planning.
4.3.3.6.3 Livelihood Component
The livelihood component was composed of two projects: goat dispersal and provision of capital assistance. For the goat dispersal, a household was given a head of goat. Once
67
the goat gives birth, one kid is given to another beneficiary while the mother and the other kids are kept by the original beneficiary. As planned, 92 households were recipients of the goat dispersal project. The accomplishment report mentioned only the dispersal but not the status of the project, although during the most recent monthly reports of the MECCDC, there were reported cases of goats which died due to miscarriage or were just found dead under a coconut tree. Since the appointment of the MECCDCC co-terminates with the feeding program, there is the question of who will monitor the progress of the goat dispersal program. Monitoring is important to ensure that the kid is transferred to the deserving household.
For the capital assistance program, the target beneficiaries were day care parents. The representative from the PSWDO visited the municipalities to consult the Municipal Social Welfare Development Office and the DCW Officer to identify the barangays for the cash assistance project. In Governor Generoso, they decided to award 10 and 12 Day Care Parents of Barangay Sergio Osmeña and Barangay Montserrat, respectively. Also being referred to as ECCD Self-Employment Assistance, a capital of PhP3,000 was given to start a small business. As reported, the economic activity where the capital was used included banana production, sari-sari store, hog raising, fish vending, snack/food vending, and buy and sell of dry goods. There were no updated reports of whether the capital was used in these entrepreneurial activities.
For the first year of implementation, there were nine day care centers for repair and improvement which were identified and eventually completed (Table 4.3.3.6.3 ). These were also provided with materials of cobble hole and big black board. Meanwhile, all the 79 DCCs in the three municipalities were provided with learning materials, kiddie tables, kiddie chairs, and play mat.
4.3.3.6.4 Capacity-building
Several training activities have already been delivered in its first year of implementation. These included the following: training of Trainors (ToT) on the revised day care manual and ECCD checklist; seminar on ERPAT and PES, eight-week curriculum; orientation to vita meal feeding; and training on IMCI and project implementation review.
There were also activities which were not included in the ECCD but were Table 4.3.3.6.4 List of Rehabilitated Day Care implemented in the province. Specifically, Centers, Municipality of Governor the province has created an office under Generoso, 2006 the governor which housed the PECCDC and took charge of the hiring of municipal Municipality/Barangay Day Care Center Baganga Dapnan Hi-way and barangay ECCD coordinators. The Macopa, Mahan-ub payment of salary for the ECCD municipal Tagumay, Saoquigue coordinators and the honorarium of San Jose barangay ECCD coordinators came from Boston Panaohan, Cabasagan Carmen the province outside of its equity. Cagamisan, Surop Governor Generoso Anitap During the second year of implementation Sitio Pasto, Crispin Dela which started in October 2006, the project Cruz covered three municipalities: Lupon, Caraga and Manay, and the City of Mati covering 81 barangays. While most of the activities were implemented in the first and the second year witnessed fewer activities and these could be further affected by the new administration and the forthcoming barangay election. The project distributed health equipment like sphygmomanometer,
68
Salter weighing scale, bathroom weighing scale, and ECCD growth cards. Learning materials for the DCCs have also been distributed.
The DCCs and RHUs for rehabilitation have already been identified and the budget for these have been allocated. Only 12 percent of the targeted DCCs and RHUs have been rehabilitated.
For 2007, it was noted that supplemental feeding, milk feeding, distribution of one kilo rice, and holding of a mother’s class were reported by the Provincial Nutrition Committee for all the barangays and not limited to the targeted barangays under the ECCD. the ECCD was claimed to be a continuation of the earlier supplemental feeding. However, this is unlikely because supplemental feeding was done for all and not to the targeted children BNL and BNVL aged 0 to 6 years old and it was only done for a day. The distribution of one-kilo rice was also not part of the ECCD project.
4.3.4 ECCD Partner
For its second year, the supplemental feeding is done in partnership with the Pondo ng Pinoy (Filipino Fund) of Archbishop Gaudencio Rosales. Filipino Fund implemented an Integrated Nutrition Program for the poor and malnourished children nationwide called HAPAG-ASA feeding the future. The menu for supplemental feeding consisted of vita- meal mixed with rice, chocoquick and brown sugar. A total of 5,000 children were targeted for the second year of implementation. It was reported that 99 percent of supplemental feeding have been accomplished.
In Barangay Nangan, the service providers are composed of the RHMW, barangay health workers, barangay nutrition scholar, day care teacher, kindergarten teacher, and Grade 1 teacher. Except for the Grade 1 teacher, all the service providers are under the supervision of the LGU while the Grade 1 teacher is under the Principal.
Available demographic data reveal that the service providers from the barangay are 50 years old on the average, and had provided service to preschool and Grade 1 students for an average of 21 years (Table 4.3.4.1). Table 4.3.4.1 Demographic profile of service providers, Barangay Nangan, Governor Generoso: 2007 The RHMW had been Service Provider Age Educational Length of in service for 28 years, Attainment Service the longest among the Rural Health Midwife 52 Midwifery 28 service providers Day Care Teacher 58 High School 22 interviewed. Kindergarten Teacher 46 3rd Yr College 13 Grade 1 Teacher 44 BEED 22 Most of the service providers worked for 40 hours a week, that is, eight hours a day from Monday to Friday. The kindergarten teacher had the least number of hours with only three hours a day for five days. Meanwhile, the day care teacher had the longest number of hours with nine hours a day for five days due to handling of three sessions of day care class with a total enrolment of 71. The kindergarten teacher had the least number of students (32). There is an overlap in the age group of pupils enrolled in day care and kindergarten. In the day care center, the ages of pupils ranged from three to six years old while the kindergarten class catered to five to six years old only. Meanwhile, the age of Grade 1 pupils ranged from 6 to 13 years old suggesting older children entering elementary education.
69
The salary/honorarium of the service providers came from the LGU budget with the exception of the kindergarten teacher. The salary of the kindergarten teacher comes from the monthly tuition of PhP50 per student. Among the service providers interviewed, the Grade 1 teacher had the highest salary of PhP13,000 per month while the kindergarten teacher had PhP2,400 per month and sometimes even less depending on the number of students who could pay the monthly tuition.
All the service providers have attended training under ECCD which they reported to be ‘very useful’ in performing their duties and responsibilities. However, they want more capacity-building activities on the Child Assessment Checklist. According to them, this is very important in determining what kind of assistance should be given to children based on the results of the checklist.
In general, the service providers have knowledge about the rights of children, health of mothers and children, and cognitive development of children. The knowledge, attitude, and perception (KAP) ratio was computed by dividing the expected answers and the total number of questions in each category. Among the service providers, the Grade 1 teacher garnered the highest score of 0.94 closely followed by the RHMW with 0.93. The kindergarten teacher had the least score of 0.74.
Table 4.3.4.2. Knowledge, attitude and perceptions of service providers, Barangay Nangan, Governor Generoso: 2007 Maternal Children' and Child Cognitive Service Provider s Rights Health Development Average Rural Health 0.93 Midwife 1.00 1.00 0.80 Barangay Health Worker 1.00 0.81 0.80 0.87 Day Care Teacher 1.00 0.81 0.80 0.87 Kindergarten Teacher 0.80 0.63 0.80 0.74 Grade 1 Teacher 1.00 0.81 1.00 0.94
4.3.5 Integration and Convergence
Integration of services for children means that all the LGUs and relevant organizations should be involved in preparing the plan, implementation, and monitoring of interventions for children zero to six years old. There should be shared ownership of the programs, and projects for children and the planning process. This would ensure achievement of the best possible outcomes for children set out in the plan. In short, there must be a single service system for children.
At the provincial level, integration is very limited. Only four out of the 12 agencies and relevant organizations were actively involved in the PECCDC/TWG in the planning and implementing ECCD. In general, it was the provincial Local Government Executive and the Chair of the Committee on Women and Children who influenced the planning and implementation of the ECCD.
At the municipal level, integration is completely absent. They provided the data required during the initial orientation, submitted a report before the appointment of the MECCD Coordinator, came up with the required MOA, and formed the LCPC. Specifically, the
70
MNO merely received the supplies for the supplemental feeding. Moreover, all the supplies and materials for the DCCs and RHUs and the money for renovation were directly issued to the concerned service provider/official in the barangay.
Coordination Table 4.3.4.1 Service providers and those providing assistance in the with other delivery of services for children: Barangay Nangan, Governor government and Generoso: 2007 non-government Service Provider DepEd LGU MSWD MHO units as well as with the other Rural Health Midwife X X service Day Care Teacher X providers is an Kindergarten avenue for the X integration of Grade 1 Teacher services for X X children. When asked about integration, the response was ‘coordination and unification of the objectives especially on the delivery system for the children.’ This was further articulated when respondents were asked whom they were coordinating with and who were providing assistance. For instance, the RHMW coordinated with the MSWDO for the feeding program and with the MHO for the needed logistics. Meanwhile, the Grade 1 teacher coordinates with DepEd and the LGU (Table 4.3.4.1) while the kindergarten teacher coordinates with the parents because her monthly salary Table 4.3.4.2 Service providers and those providing assistance in the comes from the delivery of services for children: Barangay Nangan, Governor tuition fee of the Generoso: 2007 students. Service Provider BNS BHW Brgy. Day RHMW Parents Officials Care Teacher Among the X X X X Rural Health service providers, Midwife the RHMW Day Care Teacher received the most X X assistance while Kindergarten the barangay X X X officials gave Grade 1 Teacher X X assistance to all the service providers. As shown in Table 4.3.4.2, the RHMW is supported by the BNS in the Operation Timbang; by the BHW in preparing the list of patients by sitio; by the barangay officials in providing the needs of the RHU; and by the day care teacher. On the other hand, the kindergarten teacher and the BHW conduct household surveys. Day care teachers assisted by the parents who helped during the conduct of classes; the RHMW who provided medical services; and the barangay officials who provided financial support for the day care center maintenance. The value of cooperation is clearly illustrated during the supplemental feeding. The parents provided firewood, fetched water, and brought plate, spoon and cup, other households lent the pot and ladle.
As conceptualized by the policy review project, convergence of services should be gauged at the households or through the recipients of the services on health, nutrition, education, and social protection. Thus, a household with children belonging to zero to six years old was interviewed.
71
The household interviewed was composed of the couple and their six-year old son. The mother works as an employee while the husband is a fisherman. They also had income from their farm.
The traditional division of labor exists in the family. The mother makes the decision in reproductive-related tasks. Out of the 12 tasks included in the questionnaire, only two tasks related to teaching the son in doing his homework were jointly decided by the couple. The mother, on the other hand, makes the decision on tasks related to cleaning, buying, and preparing food; immunization and giving of vitamins and iron supplements; and taking care of children.
The mother also follows practices to ensure the nutritional status of her son especially during the early years. These included, breastfeeding her son for two years, cleaning the breast with warm water and massaging around the nipples, starting complementary feeding when the baby was at his seven months old with mashed vegetables (sayote, potato and carrots), and observing proper food storage like keeping the left-over food in the refrigerator. To prevent her child from getting sick, the mother keeps the baby clean by giving him a bath twice a day and by keeping the playthings and clothes of children clean. When the baby got sick she gave him food like noodles, milk, and soft boiled egg. She also spent time playing with her child.
The source of the water for drinking is the deep well; however, it is not clear whether the water was tested for contamination. The family also has a water- sealed toilet.
According to the mother, she brings her child with her in most activities such as attending social gatherings, participating in community meetings, and watching movies. The son also sleeps with the couple.
The mother believes that the child should be rewarded when behaving well or have done something good, though he also needs to be disciplined. She rewards her son with toys and hugs or kisses him whenever he behaves well. This incentive will encourage the child and help him remember to be good always. On the other hand, she disciplined her son for being too playful and too stubborn by beating him as early as three years old.
The mother wants her son to finish his studies and envisions him to have a wholesome family of his own in the future. She wants her child to become independent, and she instills in him the values of being respectful, prayerful, honest, clean, and helpful.
To protect her child from internal and external threats, the mother discourages her son from seeing pornographic materials and games and vices like bingo, mahjong and other forms of gambling because she considers them as wasteful activities. As much as possible, she supports her son to engage in activities that could develop his artistic talent. She also encourages her son to attend religious services with the family and to watch wholesome television programs.
The mother claimed that she has not heard of ECCD. However, she had accessed and availed of some of the services from the health center like prenatal care; vitamin A and iron supplements; and feeding program. She had even attended seminars on nutrition and counseling. Currently, her child is enrolled in the day care center.
The mother thinks that a child should start schooling at age four years because at this stage, children are already eager to attend school. The children are even the ones convincing their parents to send them to school. Some parents want their children to
72
experience early education because they want them to become “early learners”. On the other hand, some parents did not want to compel their children to attend school early if the children were not interested because they might get easily bored of school.
According to the mother, her son was then very eager to attend preschool because he liked the stories read in the class and the new songs; the writing/drawing activities; and playing with his classmates. He was also excited to get his allowance every time he goes to school. The mother had witnessed how her son’s writing skill has improved. She was also informed of the progress of her son by the day care teacher whenever she visited the center. Figure 4.3.4. KAP on children’s rights, maternal and child As a result of sending her health and cognitive development of mother, son to preschool, the Barangay Nangan, Governor Generoso: 2007 mother said it would not be difficult for her to teach her son how to write and that he will easily know how to socialize with people, thus, she intends to enroll her son in Grade 1 the following school year.
Finally, the mother is slightly more knowledgeable on the rights of a child than on maternal and child health and child’s cognitive development (Figure 4.3.4). She got the highest score1 of 0.90 on the rights of the child. Her scores on the maternal and child health and child’s cognitive development were very close at 0.81 and 0.80, respectively.
In conclusion, convergence can be seen in the mother having availed of RHU services before and after becoming pregnant as well as of the day care center where her son is enrolled. Her responses to the different questions suggest that she is a responsible parent and that she exerts efforts to make her son a healthy and well- behaved/responsible adult.
4.3.6 Monitoring System
Based on the key informant interview, the ECCD Assistant Coordinator reported having designed four forms for ECCD implementation and monitoring: Form 1: Barangay Profile contains 15 items characterizing the barangay. Specifically, it contains information on population size by gender, children’s population by age group, employment and sources of income, basic education and health facilities, immunization and nutritional status of children, mortality, morbidity, child abuse, and domestic violence. Form 2: Child Profile Consent Form contains demographic information on the child as well as the other members of the household. More importantly, in this form, the parents allow their qualified children enrolled in the supplemental feeding; promise to participate in the feeding program by bringing their children to the feeding center as scheduled, weighing of children, and bringing their own plate, soon and fork; attend all the mother class
1 Score is computed as the ratio of the total expected answer over the total number of items.
73
sessions; assist in buying, cooking and feeding; and donating in cash or in kind for the supplemental feeding program. Form 3: Master list of Children is a compilation of the children who have participated in the supplemental feeding program.
The hiring/appointment of staff, e.g., engineer at the provincial ECCD Office as well as MECCDC and BECCDC was claimed to be an innovation and reported as one of the best practices in the ECCD implementation. Perhaps, it fast tracked the implementation of the activities during the first year while the presence of MECCDC and BECCDC facilitated the monitoring of the supplemental feeding. However, it has contributed to the non-attainment of the goal of ECCD which is convergence of the delivery of services at the provincial, municipal and barangay levels and sustainability of the interventions. The disadvantages outweigh the advantages. The hiring of its own staff at the ECCD Provincial Office curtailed the different provincial and municipal staff from becoming involved in the ECCD. For instance, instead of the Provincial Engineer doing the coordination and monitoring with the Municipal Engineer for the civil work in the DCC and RHU rehabilitation, the hired ECCD engineer coordinated with the barangay officials. One reason for the non-functioning of the MCPC was that the MECCDC has been performing the tasks which the former should be doing.
Instead of targeting the beneficiaries of the project as indicated in the Implementing Rules and Regulations (IRR) of RA 8980, the provincial government has included all the municipalities and barangays in three batches of implementation. However, this strategy is unsustainable and costly. After the first year of implementation in the three priority municipalities, there were no follow-up activities except for the one-day supplemental feeding. It is very costly in the sense that even the non-targeted beneficiaries in the supplemental feeding were included.
The innovation introduced in the barangay seems to be better than those being claimed by the province. For its supplemental feeding, the BHWs and the parents decided to divide the eight sitios into two clusters to make it easier for parents to bring their children and at the same time to attend the mothers’ class.
4.4 Province of Cagayan Valley
4.4.1 Profile
Classified as a second class city, Tuguegarao is a peninsula located west of the Sierra Madre foothills. It is approximately 450 km north of Manila, 45 minutes by plane and 10 hours by land.
Tuguegarao City as the capital of the province of Cagayan and the Regional Center of the Cagayan Valley Region is the hub of socio-economic growth in the region. The city serves as backbone support to the Regional Agro-Industrial Center in Isabela and to the Cagayan Special Economic Zone and Free Port (CSEZFP) in Santa Ana, Cagayan.
Barangay Capatan is one of the barangays in Tuguegarao City, consisting of six puroks. As of June 2007, it has a total population of 3,148 with 1,734 households. By age bracket, 9 percent belonged to zero to five years old while 24 percent were under the 6 to 17-year old age group. Meanwhile, adults (18 years old and above) comprised 67 percent of the total population. Of the total number of school-going children (3 to 24 years old), 647 were in school while the remaining one-fourth or 180 were out-of-school youths (OSYs).
74
4.4.2 ECCD Structure and Management
4.4.2.1 Planning
The ECCD program was introduced in the province of Cagayan in 2004. The Regional Social Welfare Development Office in Region II briefed the staff of the province on what is ECCD is all about particularly in choosing the target areas.
Originally, the province of Cagayan has prioritized only five municipalities for the ECCD based on infant mortality rate, under-five mortality, and nutritional status based on the results of the Minimum Basic Needs (MBN) survey. These were all covered during the first year of implementation. Then former Governor Edgardo Lara negotiated with the Council for the Welfare of Children to cover all the 29 municipalities during the following year. However, only 82 or 10 percent of the 821 barangays commonly referred to as “Club 82” were the targeted recipients of ECCD. “Club 82” was an initiative of the Governor to assist the most depressed barangays in terms of high poverty incidence, malnutrition, and other health problems.
While the province has set the number of target barangays, the technical working group at the municipalities decided which barangays to include in the ECCD based on the selected indicators. The municipal technical working group was asked to submit the five priority barangays but the final number of selected barangays varies depending on the income class. For instance, four barangays were selected for fifth class municipalities; three barangays for fourth class municipalities; and two barangays for third, second, and first class municipalities.
In the City of Tuguegarao, early childhood care and education was organized as early as when the City Social Welfare Office operating under the Department of Social Welfare organized its barangay day care program 35 years ago. The early childhood care and education program was enriched and strengthened when the city joined the search for the Most Child-Friendly City national contest and has consistently won for three consecutive years earning itself a Hall of Famer award in the child-friendly movement. The ECCD system was launched in May 2006.
At the city level, the ECCD was introduced per agency. For instance, the DepEd staff was briefed about the program during the training on the eight-week curriculum for Grade 1 teachers while the Social Workers had it during one of their meetings. The members of the Council were already aware of the services even before ECCD was introduced.
The MBN assessment results conducted in 2005 was used to formulate the ECCD program goals and objectives in the target barangays of Capatan and Linao West. Each Department head member of the LCPC/ECCDCC prepared his/her respective plans and targets for these barangays. These plans and targets were consolidated and included in the city development plan by the City Planning and Development Officer who is also a council member. The goals set were all in line with the national goals.
LCPC/ECCDCC members participated in a planning workshop facilitated by the Provincial ECCD Coordinator in coordination with the regional sub-Committee for the Welfare of Children on July 14-15 2006. The LCPC prepared the work and financial plans for ECCD based on the MBN assessment and family survey (tool formulated by the local council) results. The families and barangay council members were consulted on priority concerns, plans, projects, and programs for children after a thorough discussion
75
of MBN and family survey results conducted through community assemblies. Facilitating the preparation of local development plans for children, included the availability of updated children’s data; availability of local government and ECCD budget allocation; availability of technical assistance by provincial and regional ECCD coordinators; the interest and willingness of leadership to invest in children; good teamwork among LCPC/ECCDCC members and service providers and presence of enabling law.
The delayed submission of documentary requirements like the WFP was due to their earlier reluctance to participate in the project. This reluctance was because they believed that they have already been involved in ECCD as proven by their Hall of Fame award in the most child friendly city-municipality, a national contest. Officially, ECCD was implemented in Tuguegarao City when the sub-memorandum of agreement was signed between the province and the city in September 2006. This is in addition to all the submitted required documents, e.g., resolution of the Sangguniang Council authorizing Mayor RS Ting to negotiate and sign for and in behalf of the LGU, approved Investment Plan for Children by the Sangguniang Council, approved WFP, and Bank Certification for the initial deposit of the counterpart fund.
In Tuguegarao, the identified barangays for the ECCD implementation were Barangay Capatan, the barangay site for this study, and Linao West. Selecting these barangays followed a similar procedure.
The identification of Barangay Capatan as having the highest incidence of malnutrition was first rejected by the Barangay Captain who requested for another household survey. When the results of the earlier survey were confirmed in the second round, the barangay officials accepted their status as one of the most depressed barangays. In response, the barangay council drafted a resolution promising to work hard to improve the situation, particularly that of the children. Instead of using ECCD funds, the barangay council volunteered to have the repair of the day care center be charged to the Barangay IRA. It should be noted that ECCD is not yet implemented at Barangay Capatan because the fund was released when the election ban was in effect, although an exemption was issued by the Commission on Election.
4.4.2.2 Financial Management
As provided for in the sub-memorandum of agreement, the LGU provides equity for the implementation of the ECCD. Further, the LGU will take over the funding requirement and management of the project after three years. Since the ECCD has been a regular program of the city government, it has already allocated part of its IRA for the program to ensure sustainability. Allocation of funds was based on needs, projects and activities reflected in the WFP of each sector, e.g., health, nutrition, education and protection. The city/municipal government provided 90 percent of the PhP50,000 counterpart fund while the rest was put up by the concerned barangays. This was in addition to the 80 percent of the IRA that the city government allocated for education, welfare and health programs, the bulk of which are for children.
Municipalities that received ECCD funds followed government auditing and disbursing procedures. Project proposals were prepared and submitted based on the submitted WFP for the release of funds deposited in the City Treasurer’s Office. The ECCD program funds had a separate account with the Land Bank of the Philippines.
The unit office/department requesting for supplies, equipment or materials needed were held responsible in preparing for the bidding requirements. The Bids and Awards Committee undertook the bidding process and later on, supervised deliveries of
76
materials or supplies requested by the winning bidders. Each department head and staff in coordination/consultation with the service providers determined the supplies or materials to be procured. Supplies may be ordered from as far as Metro Manila for delivery by the supplier as in the case of educational reading materials delivered to the City Social Welfare Office (CSWO) for the DCC. These were distributed on June 14, 2007 to DCW. The procurement is a long process and becomes longer if there are no local bidders. It runs from two to three months or even longer.
For the City of Tuguegarao, the ECCD fund from PECCDCC was first received in December 2006 after the LCPC submitted all the documentary requirements like WFP, project proposals for the two barangays covered by the ECCD, and MBN results as bases for planning and targeting. Delay in the submission of some requirements deferred the release of funds. Implementation was further delayed by the election ban in May 2007 although an exemption was already approved.
At the province, part of the ECCD fund is released at the beginning while later releases were based on the amount liquidated. This poses a problem because of the uneven capability of the municipalities to expend their allocation. As a result, the province had to use provincial funds first.
4.4.2.3 Delivery System
Club 82, became the conduit to implement ECCD in the province of Cagayan. Club 82 has a provincial management team headed by the governor while all the department heads are members. In addition, Club 82 has a technical working group, composed of technical people from different departments as well as different national offices and NGOs based in the province. This seems ideal as Club 82 facilitated the identification of the needs of the children and that the mechanism and structure were already in place to implement the program. Club 82 targets all the households as well as the community and not just children aged zero to six years old. The functions of the PECCDC were also assumed by Club 82. Only the Provincial ECCD Coordinator was hired to implement the program. All the other tasks were assigned to the regular staff of the province.
In Tuguegarao, the City Council for the Protection of Children also known as LCPC serves as the City ECCD Coordinating Council (CECCDCC) headed by the City Mayor, Randolf S. Ting with membership as prescribed by law. The LCPC/ECCDCC follow the functions as provided for in the law such as to: (1) coordinate and monitor the delivery of services at the barangay level, (2) ensure reporting and documentation of services delivered, and (3) support and complement resources available to barangays for ECCD program improvement like purchasing learning materials and supplies. The city social welfare office acts as informal secretariat whose tasks are only to remind members the submission of reports or to notify members of meetings.
Each department head, i.e., Health, Social Welfare, Nutrition, Education, coordinates and supervises the ECCD programs and services under his/her own department. Each head submits his/her report to the City Planning Officer who collates and packages work and financial plans and reports of accomplishments, not only for ECCD but also for all other programs and services for children beyond six years of age. Reports are prepared twice a year: mid-year and year end.
At the city social welfare office, the ECCD program is handled by several staff. A welfare aide is assigned to handle and coordinate the day care; a social welfare assistant handles children with disabilities of all age groups; and the assistant to the department
77
head takes charge of adoption, foster care for abandoned, surrendered children, children in conflict with the law, and children who are victims of abuse and exploitation. The department heads coordinate all ECCD efforts/programs and services in the department. Incentives come in the form of capability building and attendance to professional association conferences and participation in LGU-sponsored “Lakbay Aral” (educational tours).
4.4.3 Accessibility/Quality of ECCD Programs/Services
From the province down to the municipal level and based on the WFP of Barangay Capatan, it appears that the Councils followed the ECCD services recommended in the CWC guidelines. They did not introduce other services because of their understanding that only those programs indicated in the CWC guidelines will be funded.
It should be noted that the services reported here referred to the whole province as the ECCD was not fully implemented in Tuguegarao City because of the delayed release of funds and the election in May 2007. In Barangay Capatan, services mentioned were those enumerated in their local development investment plan.
Province-wide, the services which have already been delivered included the following: 1) provision of reading and instructional materials and furniture (kiddie tables and chairs), stand fan, video cassette device and outdoor facility for the day care center; renovation of day care centers; 2) supplemental feeding; 3) micronutrient supplementation including vitamin A, iodine supplementation and iron; 4) provision of deworming tablets for children aged one to five years old; 5) distribution of ECCD cards; 6) upgrading and provision of equipment for the rural health center such as weighing scale, sphygmomanometer and stethoscope, and furniture like monoblock tables and chairs, and medicines (Rifampicin and INH syrup; and 7) conduct of Reach Every Barangay or REB, a surveillance program that identifies cases of neonatal tetanus.
The province has also conducted a number of capability building activities for the service providers. These are as follows: 1) Three-day enhancement training for Grade 1 Teachers on the School Readiness Assessment 2006 and the Implementation of the Early Childhood Experience; 2) Basic Course on Integrated Management of Childhood Illness; 3) Training of Trainors on the Revised Day Care Manual cum Orientation of ECCD Checklist: Scoring, Analysis and Interpretation; and 4) Training of Trainors on the PABASA sa Nutrisyon. In addition, several orientation programs on ECCD for the different service providers were also conducted.
Among the services provided for in the ECCD, the implementation of newborn screening was limited due to high cost of service. The local government-managed People’s Emergency Hospital conducts NBS but the city government only subsidizes PhP100.00 of the PhP600 total cost. Others can also avail of the service at full cost from St. Paul University Hospital, a private hospital in the city.
Among the services, only the livelihood component of the ECCD has not been implemented in the province of Cagayan. The livelihood component is intended for families with below normal low and below normal very low children. The provincial ECCD is still conducting livelihood trainings. While the ECCD Program covers children zero to six years old, there were reported activities which also addressed the concerns of older children and adults. Funds for these were not drawn from the ECCD. These included the strengthening of the Pagasa
78
Youth Association of OSYs, orientation on violence against women and children, and provision of toilet bowl molders.
Although not funded by the ECCD, the City of Tuguegarao has services for children in need of special protection. The Stimulation and Therapeutic Activity Center (STAC) and Responsive Shelter of Tuguegarao are innovations by the City. STAC is not specifically for children aged zero to six years but many of the patients at the time of the field visit were of these ages. The STAC provides specialized services like occupational and physical therapy for children with disabilities; referral services for speech and psychological evaluation; and other needed rehabilitation services for these children.
The government provides yearly allocation of PhP21,000,000 for the People’s Emergency Hospital where the STAC is a major hospital program/service for children with disabilities. The substantial ($300,00) financial assistance of Kapisanan ng may Kapansanan Inc. (KAMPI) for three years starting July 2007 ensures sustainability of the STAC until 2010.
In Barangay Capatan with the money being forwarded to the municipality, the services to be provided under ECCD were similar to those for the province. There were also others not listed earlier as follows:
Center-based supplemental feeding for 180 days and for iron syrup for seven malnourished children; Upgrading of barangay health center in terms of improving the facilities, e.g., mason work of toilet and bath and hanging of curtain and height post, and procurement of medicine (ORS, Anti-TB drugs, paracetamol and antibiotics), medicine cabinet, and weighing scale; Purchase of iron tables for lactating and nourishing mothers; Renovation of the day care center through painting of walls and finishing the floor tiles and acquisition of instruction materials, e.g., reference books, workbook and educational compact disks; and Purchase of birth contraceptives like injectables (Depo Provera), oral contraceptives, and condoms;
As reported earlier, the BC of Capatan and the Council has decided to shoulder the cost of renovating the day care center. The money earmarked for this will be spent on other activities.
4.4.3.1 The Service Facilities and Providers
The day care center is located at the ground floor of the barangay hall which is fairly accessible to all the residents of the barangay. It is open for eight hours a day from Monday to Friday. Based on the key informant interview, the day care worker was not knowledgeable on assessing the height and weight of pre-school children. She also did not know what to do with the underweight pre-school children or how to use the data on nutritional status.
Meanwhile, the Barangay Health Center is located near the barangay hall. It is open from 8:00 am to 4:00 pm from Monday to Friday and from 8 am to 1 pm during Saturday. The facility is about 20 square meters which is divided between the consultation room and the waiting area. It is generally clean and orderly, well-ventilated but poorly lit; it does not have a lavatory and water supply. The Center has basic functioning equipment like stethoscope, BP apparatus, thermometer, tape measure, infant and adult weighing
79
scales, syringes, and nebulizer. However, the patients are asked to buy medicine and supplies like gloves. Patients are also referred to the municipality for their medicinal requirement. The Center does not also have a sterilizer for instruments, Maternal and Child Health Manual and Mother and Child Book. Equipments are brought to the city hospital for sterilization.
The referral system in the health center requires patients to bring with them their record to the city hospital where they are being referred for treatment. The records are later picked up by the midwife during their weekly meeting.
At the barangay level, the ECCD service providers comprised the day care worker, the BNS, the BHWs, RHMW, and the Grade 1 teachers (Table 4.5.31). Among the barangay-based service providers, only the midwife has a plantilla position at the municipality, thus, paid a monthly salary of PhP7,062 pesos and a transportation allowance of PhP150. The other service providers receive monthly honorarium from the province, city, and barangay. Meanwhile, the Grade 1 teacher is under the Department of Education. Among the service providers, the BHW has the lowest honorarium while the DCW receives the highest honorarium (Table 4.4.3.1).
Table 4.4.3.1. Remuneration by type of service provider, Barangay Capatan, Tuguegarao City Number Service Provider Salary Honorarium Source (Peso) One (1) BNS - 650 Barangay 200 City 100 Province Five (5) BHW - 250 Barangay 200 City 50 Province One (1) RHMW 7,062 One (1) DCW - 1,450 Barangay 200 Province Two (2) GOT - 9,000+ National
With a population of more than 3,000, Barangay Capatan must have a nurse and a midwife; however, the Rural Health Center is only served by a midwife and assisted by barangay health workers. The midwife is quite young at 24 years old. She has been with the Barangay Capatan for three years. She has also attended several training programs on cold chain management, natural family planning method, renal diseases and EPI but not on IMCI, IMCH, Manual for Midwives, Nutrition and PES. She claimed to have knowledge of ECCD but does not know when it started in the barangay (This has not been implemented).
Of the five BHWs, the BHW interviewed was almost twice older than the RHM. She has been with the barangay for seven years. She reports to the health center once or twice a week depending on their activities. The activities of the BHWs included the following up of patients, home visits, assistance during the annual household surveys, administration of vitamin A supplementation in the day care center, referral of sick patients to health center, and helping the midwife in accomplishing reports. The BHW does not know the
80
ECCD despite the claim of the municipality to have conducted ECCD orientation for all service providers.
The BNS is 55 years old, had completed elementary education and has been servicing the barangay for 17 years. She is not a member of the BCPC. She reports to the health center once a week for one hour and a half. Her regular activities are weighing, inviting mothers for immunization, preparing master list of children 0-24 months, and assisting in the distribution of vitamins and deworming pills. She also conducts OPT once a year for all zero to six years old. She is an active member of the women’s group engaged in making cacao balls.
Among the service providers, the midwife scored the highest with an average score of 0.89 followed by the BHW and last was the BNS with 0.69. The midwife got the highest score on children’s rights and children’s cognitive development with 0.90 score (Table 4.4.3.2). Among the items the midwife missed on maternal and child health were 1) the possibility for a pregnant woman with goiter to give birth to a mentally retarded child, and 2) possibility for one to suspect if a person is anemic from the color of his/her palms. These results were quite unexpected. Albeit, not very different from the other scores, the RHMW’s score was lowest on maternal and child health. In fact, all the three service providers had the lowest score on maternal and child health.
Table 4.4.3.2. Knowledge and attitudes of service providers Item Service Provider BHW RHMW BNS On children’s rights 0.80 0.90 0.60 On maternal and child health 0.63 0.88 0.56 On children’s cognitive development 0.80 0.90 0.90 Average 0.74 0.89 0.69
Despite attendance to training on ECE, the Grade 1 teacher seemed not properly equipped to handle the eight-week curriculum. Some of the observations included insensitiveness of the teacher to the religious affiliation of the students, use of threatening words and shouting at students, and use of inappropriate instruction materials. When she was asked if she was aware of the teacher-child-parent friendly approach and modules in teaching Grade 1, the answer was negative. She also kept the water jug in the toilet; thus, the students kept on visiting the toilet. It was learned that she was not provided with instructional materials during the training and that she only used what was available and other visual aids which she could afford. Thus, not only were the teaching materials inappropriate for the lesson but also small to be clearly visible to the students at the back.
4.4.4 Integration and Convergence
Integration among the service providers involved more of coordination of different personnel. Some service providers thought of integration as attendance to meetings and submission of plans and accomplishments to the Club 82 coordinating council. According to the BNS, she coordinates with the BC and the midwife who sign her report while the midwife coordinates with her city health supervisors. She did not even acknowledge the assistance of the BHW and the BNS. On the other hand, another service provider considered the provision of services to her clients as integration.
At the household level, convergence was lacking based on the response of the mother interviewed. Most of the services availed of were for the children only. For instance, her
81
preschool child received vitamin A capsule, was dewormed, and was regularly weighed. There were no other services availed particularly by the mother. There were no other nutrition-related services received like nutrition education, mother’s class, livelihood assistance, seeds, and feeding. The lack of access to livelihood assistance was expected because ECCD was not yet implemented; however, the other services were already in existence before the ECCD implementation.
In Tuguegarao City, there were partners in the implementation of the ECCD and ECCD- related activities. There were private institutions like the St. Paul University and St. Louis University NGOs, parish councils, and evangelical churches. There was also the Plan International, an international child welfare agency which has been sponsoring formal education and health and nutrition needs of sponsored children specifically in-school children. However, this organization will soon end its operation in the province.
4.4.5 Monitoring System
The yearly search for the most child-friendly city municipality serves as the built-in monitoring and evaluation mechanism for the ECCD program utilizing the same assessment tool. Monitored are the programs and services for children, WFP, facilities for health, education, nutrition and protection of children, law/ordinance for children passed, actual visit to centers, programs and services, review of records, and reactions generated through interviews of parents/service providers conducted by the LGU and Regional Council for the Welfare of Children (RCWC).
Each department head prepares mid-year and year-end reports on the program based on the achievement of the objectives for the year. The result of the child-friendly movement evaluation is discussed among LCPC/ECCDCC members, parents, and service providers. The Child-Friendly Assessment tool has been effectively used since 2001 when the city first joined the contest. These are validated by members of the regional sub-committee for the welfare of children chaired by the DSWD regional director, and co-chaired by the DepEd and DOH representatives. Documentation of service delivery is usually through the mid-year and year-end narrative and statistical reports prepared by the LCPC members. Result of the child-friendly movement is written yearly not only for the two ECCD barangays but for 54 barangays with the same programs and services.
Briefly, each of the agencies involved in the ECCD implementation had its own system of reporting, e.g., where to submit and frequency of reporting, resulting in the difficulty of integrating the reports. For instance, the BNS prepares five reports and submits these to different personalities as shown in Table 4.5.5. Thus, the province came up with a single recording process in each barangay and a single monitoring form for all activities, not only for ECCD but also for all other activities of Club 82. In this manner, everyone who visits the barangay can monitor the successes as well as the difficulties and challenges in its implementation.
82
Table 4.4.5. Report submitted by type, to whom submitted, and frequency by the Barangay Nutrition Scholar, Barangay Capatan, Tuguegarao City Type To whom submitted Frequency Feedback Barangay Nutrition City Nutrition Action Annual The reports are Action Plan (BNAP) Officer (CNAO) checked for correctness during Full weighing report Midwife first then to Biannual evaluation or upon the CNAO submission. Monthly weighing report Midwife first then to Monthly Feedback is the CNAO usually provided Quarterly weighing Midwife first then to Quarterly during the monthly report the CNAO meeting of BNS. BNAP Accomplishment City Nutrition Action Annual Report Officer (CNAO)
4.4.6 Facilitating and hindering factors
Based on the annual report of accomplishments, several factors have positively and negatively influenced the implementation of ECCD in the province of Cagayan. The facilitating factors consisted of the support being extended by the local government executives as well as national agencies; positive attitude of program beneficiaries; organized and functional PECCDC, MCCDC and BCCDC or the local counterpart of the Council for the Protection of Children; and timely submission of the required documents, e.g., local investment plan and work and financial plan. A report ensured timely release of funds.
By contrast, factors that hindered or slowed down the implementation were as follows: late submission of the required documents; the long/stringent bidding process which delayed the purchase of some instructional materials; unavailability of supplies locally; non-availability of transport which limited the visits to the ECCD barangays, particularly the far-flung areas; and performance of other duties aside from ECCD.
4.5. Province of Misamis Occidental
4.5.1 Profile
Misamis Occidental is located near the narrow strip of land between northwestern Mindanao and the north central part of the island. It is bounded on the northeast by the Mindanao Sea; east by the Iligan Bay; southeast by Panguil Bay; and west by the provinces of Zamboanga del Sur and Norte.
Misamis Occidental is a third-class-income province composed of 14 municipalities, 3 cities (Oroquieta City as the provincial capital), 2 congressional districts, and 492 barangays. It has a total land area of 1,939.32 sq. km and total population of 486,723 people (as of May 2000). There is a high dependency ratio caused by the large population of residents aged 0 to 17 years (54%) and the increasing population of 60 year old and above (9.6%).
83
Calamba, a landlocked fourth-class municipality, is located in the northern part of the province along the National Highway leading from Ozamis City to Oroquieta City and to Dipolog City of Zamboanga del Norte. It is one of the smallest municipalities with its estimated land area of 112.54 sq. km. This land area is distributed to 19 barangays. As of 2000, Calamba had a total population of 17,594 or a total population density of 156 persons/sq. km.
Agriculture is the main source of livelihood in the municipality that includes coconut, rice and corn production; vegetable and fruit production; livestock raising (poultry, swine, cattle, carabao and goat); and fishing (tilapia, hito and carp). Coconut is the municipality’s main product. Cassava has been recently introduced to the farmers. Rice and corn milling, as well as cooperatives, are other income sources.
Barangay Siloy is the second largest barangay of the Municipality of Calamba. It is accessible by all types of vehicles through the 9-km provincial road from the highway. Farming is the primary occupation of Siloy residents, majority of whom own the lands they till. After farming, however, most of the farmers have secondary occupations like raising livestock, becoming hired labor, or managing sari-sari (variety) stores in the barangay. There are no big businesses and commercial establishments in Siloy.
There is a small population of Subanens that resides in Barangay. Siloy. About 50 households are members of the Tribal Community Association of the Philippines (TRICAP) of which the Subanen group was organized in 1996. The TRICAP extends lending (financial) facilities to its members and assists, together with the provincial LGUs, in goat dispersal and peanut production projects.
The two cultural traditions that the Subanens of Siloy still celebrate are the Menajak (Love) Festival and the Halad (Offering). The Menajak Festival features various street and ritual dances to the rhythm of the drum and agong as participants don colorful Subanen costumes. This festival is celebrated by Calambahanon every February 14.
Siloy Subanens take part in the halad, an offering of chicken and eggs, usually organized and celebrated in Barangay. Mamalad where more Subanens reside. (Mamalad Subanens even give durian seedlings to the Siloy group.)
Many child-rearing practices in Siloy Subanen households are similar with those of the mainstream. There were suggestions raised to document and utilize Subanen songs, stories and music but this project was never done.
Since the Siloy TRICAP secretary (a Subanen) became ill and passed away in May 2007, the Siloy group has not been active anymore. The secretary had once been in- charge on following up on all the TRICAP projects in the past.
4.5.2 ECCD Structure and Management
4.5.2.1 Planning
The formulation of the Provincial Development and Investment Plans for Children (2004- 2008) was based on the survey data presented during the 2004 workshop on ECCD 2 and consultations with the municipalities. In these plans, the provincial TWG (PTWG)
2 The data used for the 2004 ECCD workshop seemed to be the preliminary outputs of the medium-term strategic objectives set till 2005. As conveyed by the Provincial Social Welfare and Development Officer, these data were the bases for developing the Provincial Development and Investment Plans for Children (2004-2008).
84
identified three major goals--children’s nutrition, health, and education. The pilot municipalities were required to come up with their five-year development and investment plans for children. Annual work and financial plans are also submitted to the provincial LGU, which the latter consolidates to an annual provincial work and financial plan.
Aside from supporting the national goals for children, the Development Plan for Children of Misamis Occidental incorporates the Target 1000 Project of Gov. Loreto S. Ocampos. Target 1000 is the Short-Term Development Plan of the province covering a three-year period (2007-2010) or 1,000 working days of the present leadership and administration. It sets all targets at “1,000” to achieve the province’s goals for CHAMPS—Competence, Health, Agriculture, Maintenance of Peace and Order, Preservation of the Environment, and Social Services. Target 1000 includes targets for health, nutrition and education interventions directly benefiting infants, children and mothers; targets for the promotion of quality family life (substantive and relational aspects); and targets for the development of ECCD support mechanisms. All targets at various system levels (from micro to macro) affect the development of infants and children.
At the Barangay level, based on the MECCDCC’s ECCD work and financial plans, the proposed projects of Siloy are purchase of program materials for the DCC; purchase of health materials and equipment for the BHC; and supplemental feeding. The LGUs refer to the CWC checklist of program materials and equipment which are required for the DCS and health and nutrition programs.
In order to avail of the CWC funds, the BCPC was requested to determine the number of malnourished children before Siloy could benefit from the supplemental feeding activities. For the requested civil works, the BCPC needed to submit a program of work, barangay certification, counterpart manpower or resources (e.g., parents contributed additional vegetables and firewood for the supplemental feeding), and photos of the structures for renovation. Ordinances and resolutions had to be passed as well.
4.5.2.2 Financial Management
Funds are transferred from the CWC to the provincial LGU as stipulated in the Work and Financial Plan. It is by the same process that funds are transferred from the provincial LGU to the municipal LGU. The PTWG is responsible for the disbursement of funds following the procedures set by the COA. No procurement of equipment, supplies and materials for ECCD programs are made at the provincial level.
ECCD funds amounting to P1,100,000.00 per pilot municipality is obtained from the CWC (80 percent), provincial LGU (20%), and municipal LGU (10%). To date, there have been three fund releases and its fund statuses are shown below:
Table 4.5.2.2. ECCP funds released to pilot municipalities. Budget Amount Status/Remarks Source Total 1st P 1,640,680.00 Fund utilization is 78 percent CWC release Total 2nd P 2,483,287.20 Released August 2007 CWC release Total 3rd P 8,039,673.20 For release: Recently CWC release conducted orientation for expansion phase areas
85
There were time differences between the release and utilization of funds depending on the capacity or efficiency of the municipal LGUs. Consequently, succeeding releases were withheld when fund utilization from the previous release has not reached 50 percent.
An annual investment program is submitted to the municipal LGU every year. However, since 2006, the BCPC has not yet received any CWC-supported ECCD fund for its planned projects—the repair/rehabilitation of the BHC; purchase of materials and equipment in the BHC; and purchase of DCS materials.
In 2006, Siloy participated in the six-month supplemental feeding activities initiated by the MECCDCC. The municipal LGU managed the funds, purchased the necessary materials, and delivered these monthly to its eight pilot ECCD barangays.
This year, the municipal LGU released funds amounting to PhP33,000.00 to Siloy’s Day Care Parents group for another supplemental feeding activity. The funds were used to pay for the milk and ingredients the group purchased. Rice came from the NFA through the DSWD and LGUs. After the 42-day feeding activity, the Parents Group submitted a report to the MSWDO.
4.5.2.3 Delivery System dating Organization
The full implementation of ECCD with support from the Council for the Welfare of Children (CWC) began in the third quarter 2005 but the institutionalization of ECCD system as an initiative of the province commenced as early as 1998. The U.P. Education Research Program provided technical assistance then.
The PTWG for ECCD3 was formed in 2004 before the ECCD funds were released. In a workshop, the PTWG and provincial officers selected and prioritized the municipalities and barangays that would be involved in the CWC-supported ECCD system implementation. Criteria used were those stated in the ECCD Act, as well as additional indicators promoted by National Economic and Development Authority (NEDA) and the Child 21 framework.
Some of these indicators were high incidence of poverty; identified high malnutrition rate, infant mortality rate, maternal mortality rate and under-five mortality rate; low level of participation of the three to five years old children in the day care service and preschool programs; and low participation rate in Grade 1 and high drop-out rate among Grade 1 pupils.
The PTWG recommended seven priority municipalities to the Governor who made the final decision. The pilot sites are Baliangao, Calamba, Clarin, Don Victoriano, Jimenez, Lopez Jaena and Tudela.
The Governor heads the management of the ECCD system at the provincial level but the actual management was assigned to the Provincial Social Welfare and Development Officer who is the present ECCD Action Officer. The members of the PECCDC are as follows: Schools Division Superintendent, Provincial Planning and Development Coordinator, Provincial Budget Officer, Provincial Health Officer, Provincial Director of DILG, Provincial Social Welfare and Development Officer (ECCD Action Officer),
3 The PTWG is the same as the Provincial ECCD Coordinating Committee (PECCDCC). The two acronyms are used interchangeably in this report.
86
Provincial Treasurer, Provincial Nutrition Action Officer, President of the Provincial League of Municipalities, and two representatives from NGOs (Himaya and Paglaum).
4.5.3 Accessibility/Quality of ECCD Services Delivered
The ECCD health, nutrition and education interventions in the province are based on the program designs made by and “handed down” from the NGAs. However, there are presently four provincial initiatives or thrusts that contribute to or highlight ECCD goals for education and nutrition.
At the Barangay level, the participation of Siloy in the institutionalization of the ECCD system in Calamba started in 2006. The BC is the officer-in-charge of the BECCDCC while all the BCPC members automatically became the BECCDCC members. There is no additional support staff hired for the ECCD system in Siloy.
The BCPC of Siloy is said to have six committees: education, health, agriculture, environment, peace and order, and sports. The activities of each committee are enumerated in the table below:
Table 4.5.3.1. Activities performed by the six committees of the BCPC, Siloy, Calamba, Misamis Occidental Committee Activities Education . Focuses on the school and helps improve the health conditions of the children; its most recent activity was the supplemental feeding Health . Conducts survey every quarter, e.g., number of households without toilets . Follows up status of residents with illness; convinces them to seek medical advice; gives referrals or recommendations . Implements the 4 o’clock habit for dengue prevention—burn dry leaves to drive away mosquitoes, instructs people to use mosquito nets Agriculture . Implements many projects (Siloy is an Agrarian Reform Community) Environment . Tree planting as anti-deforestation measure Peace and order . Protects or secures the earth dam . Monitors residents conducting illegal fishing activities by the river Sports . Organizes basketball, boxing games, get-together and parties in the barangay
Since Siloy was identified as an ARC many years ago, a lot of agencies and organizations have “come in” to assist the barangay. Church groups and the LGU-based agrarian reform and agriculture offices coordinated with them.
The Siloy Health Center is located beside the DCC (same compound) and across the abandoned and dilapidated Barangay Hall. It is a permanent structure—roof made of G.I. sheets, concrete walls and floor – with a waiting area and consultation rooms inside that are well ventilated, generally clean, and organized. There is no electricity in the center but it remains properly lit because of the natural light that penetrates the numerous jalousied windows. The center has no piped water too. Water is sourced instead from the communal piped water system outside and stored in containers. The surroundings of the center are also clean.
87
4.5.4 Service Providers
For the BHW, “integration” refers to the concern for the needs of children aged zero to six years and their mothers. “Extent of integration” among the various service providers refers to the mothers’ orientation and home visits they are able to conduct. The collaboration between the barangay LGU and CARE Philippines or ZPHEP has assisted her in fulfilling her ECCD responsibilities. The gains of integration have been her monthly honorarium (total P450.00); and the various materials, supplies and equipment essential for the health services.
The RHMW finds the health services provided in the barangays “relevant, appropriate, and socially acceptable.” She was involved in planning and deciding which services needed to be implemented in the communities.
A list of health-related services had been provided by the RHMW (Table 4.5.4.1).The commonly utilized services were the vitamin A supplementation, OPT, and deworming. The least utilized were the family planning services and immunization (due to few number of children).
Table 4.5.4.1 Status of the health-related service provided by the RHM, Siloy, Calamba, Misamis Occidental. Services Frequency Target Served Reasons Pre-natal care Monthly 9 8.3 Target was too high Child birth/delivery As needed 13 9.5 Deliveries mostly handled by hilot Post-natal care As needed 13 9.5 Served only those assisted by RHMW Tetanus toxoid for Monthly 9 10 Target was too high pregnant women percent Vitamin A supplementation 2x/year 13 80 Regular monitoring of for family planning clients percent RHMW Iron supplementation for 13 60% Inadequate supply of iron post partum mothers Family planning—new 4 60% CDH doing family planning acceptors services EPI (fully immunized child) 32 50% Target was too high Nutrition program with Every 6 106 90% Support from the national Vitamin A supplementation months level and BHWs’ for 0-59 month olds commitment in doing their tasks Operation Timbang 1x/year 186 72.2% Target was too high CDD 4 100% Full support of the LGU CARI 3 100% Full support of the LGU
There were no innovations introduced in any of the above-mentioned services. Among these services, the RHMW found the EPI (fully immunized child) program the easiest task to implement because following up on the children basically entailed the RHMW coordinating the schedule of services and list of beneficiaries with the BHWs. Considered the hardest was childbirth and delivery because of the inaccessibility of transportation to the areas and because of the difficult terrain in the far-flung areas.
The day care service sessions in Siloy are conducted five days weekly, three hours daily. The DCW renders another three hours for other related DCS tasks everyday. All 28
88
children enrolled this school year belong to the morning class. Their ages ranged from four to seven years. The table below enumerates the DCW’s tasks:
Among the tasks performed by the DCW, meeting with the DC Parents Group was the easiest for the DCW because the parents were cooperative and supportive—they spend
Table 4.5.4.2. DCW’s tasks, Siloy, Calamba, Misamis Occidental Tasks Freq Innovations Target % served and reasons 1. Conduct DCS Daily Used pictures, 28 80%--due to sickness, sessions reading enrolled dropped out, under aged; materials, field children live far away from the DCC trip 2. Meets up with DC Monthly Parents Group 3. Conducts Daily for 28 90%--absences due to supplemental 42 days children illness feeding for DC children 4. Celebrate Araw ng Yearly Calamba 5. Celebrate Children’s Yearly Month time in the DCC to help the DCW manage the children; respond positively when asked to contribute; and easily understand the DCW’s needs. Conducting the DC sessions was the hardest. Because children’s family life experiences are varied, the DCW found it difficult to adjust or manage the class effectively.
Moreover, since 1996, the provincial LGU had not purchased new program materials for the DC children like drawing books and developmentally appropriate reading materials. The DCW used the curriculum development framework and procedures she was trained on in the early 2000’s. The same were contained in the Revised DCW Manual which provides a step-by-step guide to DCWs on how to develop their DCS curricula. At the start of the school year, the children’s health information or records were given to the DCW so that continued medical assistance (e.g., purgative every two months) can be extended. Children’s birth certificates were also shown or submitted to her.
From 2002 to early 2007, the DCW used the Child Development Checklist (CDC) to assess children’s developmental level. Starting July 2007, she had been administering the ECCD Checklist; the results are to be utilized for curriculum planning. The DCW has attended numerous training programs since 1997 and found these beneficial in enhancing her competencies to provide creative activities appropriate for the children.
The MSWDO was involved in planning and deciding on the relevant and appropriate ECCD interventions in the communities. As the ECCD Action Officer, she directly coordinates with all agencies concerned through the MECCDCC and BECCDCCs. She is also involved in planning, implementing, monitoring, evaluating, and reporting the ECCD projects in Calamba. The target participants are the children, parents, BDCs and the communities.
As an MSWDO, she is directly involved in supplemental feeding, DCS sessions and referrals (Table 4.5.4.4).
89
The recent training programs included child development, ECCD assessment checklist, among others (Table 4.5.4.3).
Table 4.5.4.3. Training activities attended by the DCW’s, Siloy, Calamba, Misamis Occidental Training program/ Topic Dates Training Funding to attend provider Child development June 2007 MSWDO Municipal LGU ECCD assessment checklist June 2007 MSWDO Provincial LGU, National agencies DCW curriculum and instructional May 2002 U.P. ERP Municipal and Provincial materials development seminar- LGUs workshop ECCD Child development monitoring April 2002 U.P. ERP Municipal and Provincial and session planning seminar- LGUs workshop Creative teaching for DC children July 2001 U.P. ERP Municipal and Provincial LGUs Trainers’ training on creative teaching May 2001 U.P. ERP Municipal and Provincial for DC children LGUs
Table 4.5.4.4. ECCD projects in Calamba ECCD Interventions Target Participants Frequency Supplemental feeding malnourished children 6-month duration/ year Day Care Service sessions 3-6 year old children Daily Referrals 3-6 year old children with As the need arises needs and their parents
These services were promoted to the target participants through barangay assemblies, parents’ meetings, and PES sessions. Supplies for these services are oftentimes inadequate because of insufficient funding.
The MSWDO believes that everyone who is concerned with the implementation and delivery of services should follow procedures or processes (protocol) as prescribed, recommended or designed depending on the nature of the services. Training programs are provided anyway. The delivery of ECCD services has improved because of the “convergence of agencies” and the organization of the MECCDCC and BECCDCCs.
The Grade 1 Teacher has been teaching in the Siloy Elementary School for four years now and in the Grade 1 level for one year only. He is a college graduate and is employed on a permanent status by the DepEd District of Calamba. His salary is P10, 939.00 per month.
The Grade 1 class is held five days a week from 7:30 am to 2:00 pm. The 26 children in the GOT’s class were all required to submit their birth certificates and to take the School Readiness Assessment (SRA) when they applied to be admitted before the start of S.Y. 2007-2008. Three dropped out from school since then, due to poor nutritional status, inadequate daily subsistence, and distance from home to school. The table below enumerates the services he provides (Table 4.5.4.5):
90
Table 4.5.4.5. Services provided by the Grade 1 teacher, Siloy, Calamba, Misamis Occidental Services Freq Target Served Reasons R-BEC curriculum Daily All 70- Different levels of 75% thinking Supplemental feeding (Food for Weekly All 100% Children loved it School program of DepEd) Managing children’s illness Acquired sick ones 80% Lack of medicines
The GOT considered the supplemental feeding as the easiest task because the children and assisting adults were all cooperative. The hardest task was managing children’s illness because of the lack of paraphernalia and medicines. To illustrate, the GOT had a Grade 1 pupil who seemed to be hearing-impaired. The GOT found out that the cause was ear infection. He helped clean the child’s ears everyday, applied herbs, and finally referred the child to the BHW. He was disappointed that some of the children’s families were “hard to reach” because they prioritized their livelihood/work over meeting their children’s immediate needs.
Before the start of the school year, Grade 1 entrants took the SRA in order for the school to determine their developmental level in five basic competency areas: Gross and Fine Motor, Receptive and Expressive Language, and Cognitive domains. These domains are critical in tracking Grade 1 learning competencies.
The SRA results of Grade 1 pupils in Siloy elementary school indicated that 95 percent of them were “not ready” for the Grade 1 learning competencies. The GOT explained that children might not have been able to comprehend the SRA instructions which were administered in English as he was instructed to do. It was not clear how the GOT used the eight-week ECD curriculum to help children develop the readiness skills that were lacking. As of data-gathering time, the second SRA consolidated report for the second administration, i.e. after the eight weeks, was not yet available. (The District Reading Coordinator (DRC) of Calamba refuted the GOT’s explanation: the SRA Test (SRAT) Manual states “use the first language/ mother tongue/dialect that is familiar to the child.”)
Of the 22 Siloy elementary school Grade 1 pupils tabulated in the DRC’s consolidated report, 73 percent had ECE experiences under the DCS. The Child Development Checklists of these children were not forwarded to the Grade 1 teacher or to Siloy elementary school. The DRC commented that they are not interested in the end-year assessment results of DC children because according to them there is no link between the DCS and Grade 1 curricula.
The GOT uses the R-BEC curriculum developed by the DepEd. He modifies this from time to time to fit with his pupils’ “level of thinking.” Survey and test measures are the other assessment techniques used in class.
The School-In-Charge directly supervises the GOT’s work and extends technical assistance to teachers particularly in the area of pupils’ achievement. Consultations may be done as the need arises; however, the GOT has not received any feedback for improvement. Table 4.5.4.1.6 shows the list of reports the GOT prepares in order to document different aspects of teaching the Grade 1 class.
4.5.5 Integration and Convergence
For the BHW, “integration” refers to the concern for the needs of children aged zero to six years and their mothers. “Extent of integration” among the various service providers
91
refers to the mothers’ orientation and home visits they are able to conduct. The collaboration between the barangay LGU and CARE Philippines or ZPHEP has assisted her in fulfilling her ECCD responsibilities. The gains of integration have been her monthly honorarium (total PhP450.00); and the various materials, supplies and equipment essential for the health services.
Table 4.5.4.1.6. Reports prepared by the Grade 1 teacher Report Submitted to Freq Receive feedback? Pupils’ test results or achievement S-I-C Quarterly No Reading assessment S-I-C Quarterly No Class attendance S-I-C Monthly No Pupils’ nutritional status Nurse Annually No
For the BNS, “integration” is coordinative in nature, i.e. it refers to the coordination between the BNS and MNAO. The BNS has not collaborated with private and non- government agencies in the conduct of her responsibilities. For the MNAO, “integration” refers to being “integrated in other programs implemented by the LGU to the different sectors” or “the services rendered are not on health alone.” The MNAO believes that ECCD has improved service delivery to children aged zero to six years. The DCW joins the BNS in monitoring the weight and health of children and families through mothers’ classes and home visits. The MNAO has also collaborated with private doctors and civic organizations who conducted outreach services on nutrition.
4.5.5.1 The Siloy Household
The household is a nuclear family composed of five members: the couple and three children aged eight, six and one year(s) old. The sources of household income are farming/livestock raising and hired labor.
4.5.5.1.1 Care and Nurturance of Children
The mother is the main player when it comes to attending to the children’s sustenance. She buys food (ingredients), prepares the meals, and feeds the children. She is also responsible for bathing the children and putting them to sleep. She helps them with their homework or teaches/reviews school lessons (on speaking, reading, writing) in their home. Outside, she accesses services like immunization and vitamin supplementation. She also performs other household tasks like laundering and ironing. Approximately 12 hours per day are spent on caring for her children. The father is involved in feeding the children. Meanwhile, the children are involved in all tasks except for meal preparation.
4.5.5.1.2 Health and nutrition practices
Upon the advice of her parents, the mother availed of the pre-natal services in the barangay during the three pregnancies she had. Only one of her three pregnancies was more difficult because of experienced headaches and dizziness during the first trimester. She consulted the BHW to determine the cause of her discomfort.
All her children were breastfed for more than 10 months. The mother considers breastfeeding very important because the colostrum strengthens the children’s immune system, it saves on cost and it is easier to do/manage. The BHW encouraged her to breastfeed. She breastfeeds the youngest about eight to nine times in day; three times
92
each in the morning, afternoon and evening, with each breastfeeding time lasting about 15 minutes. She cleans her breasts and nipples by washing these gently with soap when she takes a bath.
This started when the (youngest) child was six months old. Foods regularly given were vegetables in soup like squash, upo, and papaya. Feeding happens three times daily. The foods were either prepared in the home or bought and stored in a pot in the kitchen.
Children take a bath once daily and they are sponge-bathed or cleaned up before they sleep in the evening. Eating paraphernalia are washed with soap and foods are stored in pots in kitchen.
When children are ill, the mother feeds them congee, milk and biscuits. It is believed that Royal Tru-Orange soft drink can bring down fever so she serves this also to a feverish child.
The household uses water-sealed toilet. The source of water is the spring, which the mother claims to be safe for drinking.
4.5.5.1.3 Early education practices
The mother believes that disciplining children is a must so that children grow up with good manners, conduct themselves well, and possess values like respect for elders, helpfulness, honesty, and fear of God. The positive discipline techniques include praising the child; hugging, kissing or showing affection; giving gifts like Barbie Doll; or permitting the child to join the DCC’s field trip. The “right ages” to discipline children are between five and ten years when children are “still obedient” and parents are confident that what they say or teach the children will not fall on deaf ears. On the other hand, the negative discipline techniques include reprimanding, reminding, scolding, “lecturing,” or spanking.
While children in the past started schooling at seven years old, children at present are sent at earlier ages because more adults believe these are the formative years. In fact, the mother thinks that children as young as three years old can already enroll in the DCS because the earlier they are exposed to a variety of stimulating learning experiences, the earlier they will likewise develop.
Generally, parents who send their children to ECE programs like the DCS want their children to be prepared for Grade 1 schooling. On the other hand, parents who do not enroll their children reason that the ECE experiences are a waste of time. They are busy with farm work and there are no additional hands to attend to their children’s needs in the DCS or meet the requirements like bringing or fetching them; participating in DCS or parents’ activities take up their time.
Without any difficulties or anxieties, the two older children attended the DCS when they were four to five years of age. Before this, the DCC was already a familiar sight since the children participated in feeding activities conducted in the same area. They would look forward to attending the DC sessions everyday and meeting new classmates. They liked the drawing activities best and the writing activities least.
The mother is not knowledgeable about how the DCW conducted children’s assessment but she was informed about the status of her children’s development (a “paper” was shown to her). For her, the DCS contributed most especially in her children’s social
93
growth—overcoming shyness and gaining confidence. She intends to enroll the youngest one in the DCS someday so that he can become like his older brother. To protect their children from some internal and external threats, the mother shared that they encourage the children and whole family to attend religious activities/services as these are also practiced in school (“religious hour”) and to engage in activities like music, art, sports, and gardening in order to develop or improve their talents and skills; provide safety measures at home to prevent accidents like turning off the main electrical switch when the children are left alone in the house; ensure that children do not have pornographic and violent media materials accessible; do not witness violent conflicts or confrontations between spouses; and they do not engage in gambling activities in the neighborhood. However, the mother allows the children to choose whatever radio program, television program or printed materials they want to listen to, watch or read.
4.5.5.1.4 Aspirations for the children
The mother would like to see her children study and finish school. These would lead them to work and later on to have families of their own and “live a good life.” The mother obtained the highest KAP ratio (1.00) on children’s rights and the lowest KAP ratio on maternal and child health (0.56). Her KAP ratio on children’s cognitive development was satisfactory (0.73).
Among the different ECCD services available in Siloy, the household availed of the following for its members:
Table 4.5.5.1.4. ECCD services available in Siloy Services F M C1 C2 C3 Mother and the unborn child: Reproductive health and family planning / / Pre-natal check visits / Tetanus toxoid immunization / / / Nutrition education program / / /
Infancy: Growth monitoring and promotion / / Birth registration / / / Full immunization / / / Breastfeeding and complementary feeding / / / Micro-nutrient supplementation Food supplementation / /
Early childhood: Day care service 4 yr. 5 yr. old old
4.5.6 Monitoring and Evaluation
The PTWG monitors the ECCD implementation in the pilot municipalities every quarter. In teams of five members, they visit the areas to verify project status, identify hindering factors in implementation, and assess the functionality of ECCD organizational structures at the municipal and barangay levels.
No monitoring forms are referred to but PTWG members use existing program indicators to monitor in the field. Data generated from monitoring visits are utilized by the specific offices (agencies) that provide technical assistance for respective programs (e.g.,PSWDO). The CWC report forms are accomplished. A provincial ECCD
94
management information system (MIS) is likewise maintained but, to date, not all of the consolidated ECCD data from the municipalities and the registry/directory of ECCD service providers have been encoded or updated yet. ECCD service providers monitor the outputs of their respective programs regularly. Through them the BCPC/BDC monitors the projects as well. Survey results, problems, and concerns are presented in the BDC meetings and discussed in the quarterly Barangay General Assemblies.
The barangay office is housed in a dilapidated structure so all the documents pertaining to the operations of the BDC are kept in the homes of the Barangay Secretary and Treasurer. There is no ECCD management information system in Siloy.
5. CONCLUSIONS
5.1 ECCD Situation
While efforts have been made, malnutrition remains to be a problem in the country. Malnutrition exists primarily because it is highly linked with economic development. Developing countries like the Philippines have low income capacity which is a major cause for the inability to secure food. At present, the identified nutritional problems among preschool children are: 1) protein-energy malnutrition, 2) obesity, and 3) micronutrient deficiencies, i.e. vitamin A, iron, iodine and zinc.
There are, however, some encouraging signs of improvement. Given the declining trends in the prevalence of undernutrition in both preschool and school children, the interventions as embodied in the MTPPAN are apparently effective. Notable among these interventions are supplementary feeding; nutrition education including the promotion of breastfeeding and infant young child feeding; and essential child care services which includes immunization, growth monitoring, micronutrient supplementation, and integrated management of childhood illnesses. A major boost in the implementation of interventions is the Accelerated Hunger Mitigation Program (AHMP).
The general health status of Filipino children zero to six years old has been improving for the past decade. However, there is an apparent disparity in the health status of children among the different regions in the Philippines. This is demonstrated by the infant mortality rate wherein the national infant mortality rate has declined rapidly in the past eight years while a wide range of values was observed among regions. Furthermore, efforts to improve the health status do not seem to be sustained as evidenced in the decrease in the rate of decline in the maternal mortality rate in recent years. The same observations were noted in service delivery. For instance, there is disparity in the rate of fully immunized children and in NBS coverage among regions. Immunization rates for individual vaccines have not consistently improved through the years. Thus, there is a need for an integrative approach that will provide a more sustained improvement in health status and a more equitable delivery of services nationwide.
The preschool education services in the country are primarily provided by the government. As of December 2006, if the benchmark is one day care center per Barangay, then the country still needs about 9,208 centers nationwide. Moreover, about 10 percent of the DCCs do not have a Day Care Worker. Because of the limited availability of data for the preschoolers, the review focused on some of the studies conducted on the subject, which has established that the participation rate of children aged zero to six in preschool services has been relatively low because of the economic cost.
95
The statistics indicated that there is an urgent need to address child protection issues. It was estimated that there are about 50,000 street children and based on a sample, about eight percent were between two to five years old. Moreover, one of five children between zero to six have some form of disability. This would have significant implications to the Education for All goals.
5.2 The Policy Framework
The review has established that there are more than enough legislations designed to promote early childhood care and development. Before the year 2000, various statutes were promulgated to cater to sectoral concerns in ECCD including nutrition, health early education, and child protection. The promulgation of the ECCD Law (RA 8980), is again a very significant positive step towards achieving the ideal mechanisms for early child development. However, there is an apparent need to reconcile some of conceptual basis of the previous laws in relation to the provisions of the ECCD Law and to the visions of early child development.
5.3 ECCD Implementation
The main ECCD interventions that were seen in the field across the study sites were reflections of the usual programs implemented under the various statutes promulgated before the ECCD Law. The fact that there is a prospect of funding support from ECCD generated the enthusiasm and commitment from various stakeholders at the field level. In spite of the difficulties encountered, the commitment of the members of the coordinating committees and service providers to provide service kept them going. The implementation of the ECCD program made them realize the importance of their role in caring for children 0 to 6 years old. The support of the local government also helped them in the implementation of the ECCD program. As a result of the ECCD implementation, there had been some expansion of the regular ECCD services, rehabilitation of existing facilities, upgrading of ECE materials and capacity building among the various service providers and stakeholders of the ECCD program.
Access to basic ECCD services is limited mainly due to inadequate resources including manpower and delayed release of ECCD funds. Moreover, the location of the health center or the day care center to some of the households in the barangay may prohibit their access to the ECCD services.
In terms of the quality of ECCD services, there is a need to improve them at the level of inputs (manpower and resources), process, and results. Manpower was found to be insufficient in terms of number (MNAO, BNS, midwife) and capacity to perform the tasks expected of them due to inadequate training. Moreover, the materials and facilities were found to be limited mainly due to the delay in the release of funds. In terms of process, there is a need to strictly follow the protocol and guidelines issued for the implementation of some ECCD services, e.g. conducting a supplementary feeding activity should be 90- 120 days; use of the eight-week curriculum for the new Grade 1 pupils so as to uphold the standards in all ECCD areas and for the full realization of the effect of the services. As to the quality of results, evaluation of the ECCD services is needed to be able to determine their effectiveness.
Integration and convergence are concepts that are not yet internalized at all levels including the household. In fact, the implementation of ECCD services as one integrated program needs to be promoted at the barangay and household levels. Thus, there is a
96
need for new strategies and activities to which these concepts can be elevated from awareness to understanding level at household, barangay, municipal, and provincial levels. Moreover, there is a need to improve the feedback mechanism from the household up to the national level.
The critical challenge of the ECCD implementation is the operationalization of the mandate to provide a system based on multi-sectoral and inter-agency collaboration in the delivery of a comprehensive, integrative, and sustainable ECCD services at various levels from the national to the local levels of implementation.
6 ISSUES
While significant and notable improvements were observed across the various case study sites, there is a need to input the insights generated in the review process to allow for the modification of existing policies and processes in order to promote a more efficient implementation, enhance, and sustain the gains as a result of program interventions.
6.1 Alignment of Previous Laws on Children with RA 8980
While the ECCD Law is a very significant positive step to provide the mechanisms to integrate and harmonize prior ECCD initiatives, there are apparent issues relating to the consistency and alignment of previous laws with the ECCD Law. In terms of scope, most previous laws have mandates covering a broader age group for children. However, the ECCD law was very specific in its intention to cover only children between zero to six years old. This would have very critical implications, particularly in terms of coordination, jurisdiction and monitoring. For instance, in most child protection laws, the scope covers children beyond six years old. Hence, in terms of monitoring, the current system does not allow for an easy decomposition of the clients and their needs in terms of a structured age-group.
The passage of the local government code also has significant implications to the implementation of ECCD. Under the devolution, basic services such as ECE were delegated down to the smallest political administrative unit of the government: the Barangay. As a consequence, the data for ECE had been scanty particularly at the provincial, regional and national levels. This is partly due to the fact that LGUs do not see either the need or the obligation to provide ECE information beyond their immediate level of jurisdiction and mainly due to lack of mechanism to integrate the information beyond the municipal level. In most cases, the level of data aggregation is only up to the municipal level.
6.2 Less Emphasis on Child Protection
In the declaration of policy, the ECCD Law was very explicit in saying that “… promote the rights of children to survival, development and special protection with full recognition of the nature of childhood and its special needs….Section 2”. Further, in the identification of the duties of the Barangay Council for the Protection of Children, child protection was explicitly mentioned. However, in the implementation, most of the services provided for under ECCD were mainstream ECCD programs such as nutrition, health and ECE. Protection and
97
special needs issues are seldom incorporated. For instance, the team has never encountered special learning sessions for disabled children.
Further, the notion of “Protection” as operationalized by BCPC under P.D. 603 has assumed a legalistic character and practice. Children are generally being provided services by government institutions/agencies, when such children become victims of abuse, neglect, and abandonment by parents or guardians. This unbalanced emphasis on the legalistic practice appears rather reactive rather than proactive, in the sense that no prevention strategies have been designed to counter the rising incidence of children in need of special protection.
6.3 Cost-Sharing (Equity) Scheme
As a matter of policy, funding for ECCD interventions is supposed to be done under a cost-sharing scheme. Feedback from the focus group discussions indicated that the sharing was about 70:30, that is, 70 percent of the cost will be funded under the program and the remaining 30 percent will be funded as equity by the LGU. Some local government executives forwarded the argument that the 30 percent equity is very high, particularly for a 5th class municipality. In fact, one of the barangay officials indicated that the barangay may only be able to raise the required equity for a specific ECCD project in three years time.
6.4 Sustainability of ECCD-Hired PECCD Coordinator
In one of the case sites, it was noted that the provincial ECCD coordinating officer was directly hired from the ECCD program management. As a result of the financial incentive, the level of effort of the hired ECCD officer was relatively high. The coordination effort was very good which resulted in the substantive participation of the various agencies involved in ECCD implementation, particularly in the planning stage at the provincial level. However, the sustainability of a directly hired officer under the ECCD framework may be put into the test as soon as funding for the program is terminated.
6.5 The Role of Parents in the Day Care Center Sessions
During the site visits, it was observed that majority of the parents stayed with their children at the premises of the day-care centers during session hours. In one of the sites, about five mothers were with their children inside the day care centers to monitor their children; while the majority of the parents were just outside waiting for the session to end. The fact the parents stayed with their children during the entire course of the day care center sessions defeats the very purpose of the center, which was intended to cater to the need of the working parents. The fact since most of the enrollees now of the day care centers are non-working parents (by virtue of their willingness to stay with the child in the center) may indicate the real targets of the centers, which are the working parents, may have been disenfranchised by the non-working parents.
The other relevant issue associated with the role of the parents in the day care centers was the interest of the parents for their children to acquire added skills that would prepare their children for the formal elementary education. This attitude would not be consistent with the intent of the day care law.
98
6.6 Transition from Day Care Centers to Grade One
In the preceding section, it was noted that parents stayed with their children during the sessions at the day care centers. As a consequence, children were unable to get used to being independent in the class.
The field visits revealed that many parents stayed within the school premises to wait for their new Grade 1 children. This issue was highlighted in one case where a child cried and refused to enter the Grade 1 classroom fearing that her mother would eventually leave her behind as soon as she enters the class room. Hence, the inability of the children to develop independence at the early education stage is carried over during the transition to grade one.
6.7 Inappropriateness and Inadequacy of Instruction Materials for the Eight- Week Curriculum
Grade 1 teachers (GOT) are required to attend the training for the implementation of the eight-week curriculum for GOTs. However, there were no provisions for instruction materials. Thus, GOTs either prepare or buy visual aids which may not conform to the prescribed ones. This was observed in one of the field visits where the Grade 1 teacher used materials with inappropriate examples. Further, while the ECCD law was explicit in the promotion of location-specific learning materials, this has not been operationalized yet at the barangay level. In fact, in one of the sites visited, the learning materials found in the DCC were still learning materials from the developed countries like the United States, United Kingdom, and Australia, among others.
6.8 Insufficient Manpower
Day care activities at the day care center vary from playing to feeding, to other developmental activities. Thus, a day care worker is burdened with many activities especially in the administration of the daily day care learning sessions. A class of about 20 children will be very difficult for a single day care worker.
6.9 Sectioning of the School-Ready and Not School Ready Pupils
In some instances, the number of identified non school-ready pupils was considerably low. To mitigate this situation, the non-ready pupils were separated into another section which was to be handled by another teacher. However, there is no curriculum for the non-school ready pupils. As such, the head teacher simply made the instruction to the teacher-in-charge of the non-school ready to tone down the level of treatment. This was compounded by the fact that the teacher-in-charge of the non-school ready did not attend the training program for the eight-week curriculum. The problem became more complex in cases where there is only one classroom for the new Grade 1 entrants, which would be expected in most of the communities under the ECCD program.
6.10 ECCD Monitoring System
One of the key elements to an effective delivery of ECCD services is an efficient monitoring system. During the field visits, of an effective monitoring system seemed absent particularly at the barangay level.
99
To dramatize the point, in one of the sites visited, there was very minimal nutrition intervention because the Barangay Nutrition Scholar declared that the incidence of malnutrition was insignificant. However, the extent of malnutrition among new school entrants in the same community was relatively high. In fact, the incidence was about 33 percent. This is an anomaly because malnutrition can not just happen overnight. If the extent of malnutrition among zero to six children was practically insignificant, where would the malnourished children among the new Grade 1 entrants be coming from?
6.11 Misconceptions on ECCD Integration
In the true sense of the word, the ECCD services at the time of this review are not yet integrated. The providers and stakeholders view that the services are already integrated because the centers are offering the various ECCD services and that, the process entailed the participation of various agencies of government and NGOs. However, it is argued here that the true essence of an integrated ECCD services can be characterized by convergence. For ECCD services to be more meaningful and effective, such interventions must converge to a specific household which covers both the parents and the children. An ECCD facility can readily report excellent statistics of increased level of reach in PES, IMCI, EPI, OPT, and feeding, among others. But it is not very effective if PES goes to one of the parents in one household, IMCI goes to the first child in another household, feeding to the third child in yet another household, and so on.
6.12 ECCD Visibility and Advocacy
While ECCD has been going on for quite sometime in most of the study sites, the household level discussions revealed that the extent of awareness about ECCD as a Program has been very low. In fact, some of the mothers interviewed never heard of ECCD. In one of the study sites visited, there was not even a single signage that would show the presence of the ECCD program in the community.
6.13 Multi- Tiered Schemes (ToTs)
To deliver the human resource development (HRD) component through training activities, the implementation strategy was to employ the Training of Trainors (ToT) concept. Feedback from the field visits indicated that there has been a significant departure from the standards of the acquired knowledge and skill by the local stakeholders through the ToT concept.
6.14 Overburdened BCPC
The Barangay Council for the Protection of Children was organized as the implementing body at the local level as provided for P.D. 603. This council is basically composed of the BC, School Head, Barangay Midwife, BHW, BNS, DCW, SK Chairman, and a representative from the NGO.
Most of these personalities also constitute the Barangay Agrarian Reform Committee, which is also the implementing arm of one the most significant and controversial rural development programs in the country - the Comprehensive Agrarian Reform Program (CARP). The BCPC was also tasked as the implementor of the programs under RA 9344 or the Comprehensive Juvenile Justice and Welfare Act of 2006.
100
And now, with ECCD, the same personalities are again tasked with the implementation of yet again another significant development intervention of the government. It is agued here that these personalities are now overburdened with the responsibilities of implementing these various significant development programs of the government. Further, the BCPC was conceptualized to operate under the concept of voluntarism; hence, it has been difficult to recruit more competent members to the committee.
Furthermore, at the national, provincial, and municipal levels, the ECCD coordinating committees are supported by an ECCD secretariat. This was not made explicit under the law. Hence, at the Barangay level, there is a coordinating committee but without an ECCD secretariat.
6.15 Sense of Project Ownership at the Community (Barangay) Level
One of the key informants in the study mentioned that while it would have been preferred that the level of authority be lowered down to the Barangay level, the fact that project disbursements are done at the municipal was accepted as a convenient excuse to avoid the accountability associated with fund disbursement. As a consequence, there was a feeling of alienation on the part of the local government unit.
7 RECOMMENDATIONS
7.1 Alignment of the Existing Statutes with ECCD
Prior to the ECCD Law, there were various statutes promulgated to effect the delivery of ECCD services. The problem is such laws had scopes much broader than ECCD, which mainly focused on children zero to six years old. It is suggested that explicit policies should be promulgated to develop a framework within those respective laws so that the implementation can be structured based on the specific needs of children stratified according to a rational age grouping. For instance, the law providing for the protection of children is concerned with child labor. For all practical purposed and intent, this concern may not be very relevant to ECCD. Also, the child-centered development mechanism envisioned for LCPCs and local ECCDCCs is lacking. As a consequence, there was no comprehensive set of data regarding the situation of children aged 0-6 years and their families in Calamba. Whatever available data were not presented according to age ranges and developmental stages so it was not clear which pertained to ECCD and non-ECCD.
To operationalize this, the existing ECD programs under various existing laws can be structured by concerns according to age categories. It should not be very difficult to embrace the idea that there could be health, nutrition, education and social protection concerns according to various life stages from early childhood to young adulthood. For instance, the Child 21 framework for child development should be emphasized to LGUs. This framework uses a life cycle approach in planning, thus, stratifying needs, programs/services, outputs according to age groups—Mother and the unborn child; infancy (0-less than 1); early childhood (1- 6); middle childhood (7-11); and adolescence (12-17).
101
7.2 Establish a Sub-Committee under the BCPC
As argued earlier, the BCPC is also involved in most of the major development programs in the barangay, wherein the scopes are much broader than that of the ECCD. To avoid the problem of delineating the ECCD concerns within the mandate of the previous statutes where the BCPC is also involved, a smaller sub-committee under Barangay Committee on Child Protection can be instituted. This could still be chaired by the “kagawad” (councilor) sitting in the Barangay Health Committee.
To run parallel with the structures from the national down to the municipal level, a secretariat at the barangay level must also be created. This can be headed by the DCW. The other members could be the parent representative and the NGO representative. Two other members of the secretariat can be drawn from the community at large chosen by the BCPC sub-committee on ECCD upon endorsement of the parent representative.
Finally, there is the need to reconsider the concept of voluntarism in the implementation of ECCD programs at the barangay level. It is suggested here that an explicit policy on incentive schemes should be provided in order to enhance the level of effort and commitment among the service providers.
7.3 Apply a Modified ToT
The ToT concept can be best utilized when the trainees themselves are already capable trainors. The essence is to orient the trainor-trainees the perspective on the new subject matter. If the ToT concept is applied to stakeholders who were never trainors themselves, then there are so many avenues for knowledge gaps and effectivity of knowledge transmission. It is recommended that the training should be made directly to the local stakeholders at the Barangay level. If there are logistical constraints, then capable trainors from locally based (Regional/Provincial) academic institutions and NGOs can be tapped as the direct trainors for the local service providers. If necessary, then the trainors from locally based institutions can be the recipient of a ToT for ECCD in their respective areas and must be tasked to train the ECCD service providers.
7.4 School Readiness at Entry to Grade One
The high dropout rate prevalent in Grades 1-2 in our country (Heaver and Hunt, 1995), plus the very low national achievement results of children in the early grades prompted the Bureau of Elementary Education to explore various ways to better prepare children for school. This has also been cause for the emphasis on school readiness, transition from home to school, and keeping children in school. Initially, there was the Summer Preschool Program, which aimed to develop the socialization and “readiness” skills of children aged 6.5 to 7 years entering Grade 1 in the coming school year. The entry age requirement then was 7 years. Overall, this pilot program met with mixed success. However, the drop out rate in the early grades of children who were preschoolers in the program was only 1% compared to the 15% for children who did not have the summer pre-school experience. Complementarily, in 1994-1995, the official age for entry into primary school was dropped to 6 years of age. DepEd justified this policy through a research that showed there was hardly any difference in the competencies of the 6- and 7-year-olds.
102
Furthermore, majority of children entered school then “at a definite disadvantage” because they have not had the opportunity to go to preschools or avail of the DCS at the least). So in a typical Grade 1 class in the public schools, majority of the students did not have prior ECE experiences and were, thus, unprepared for formal education. Hence, in order to mitigate the problem of school readiness upon entry to Grade 1, the following measures are suggested: Orientation and continuing education of DepEd teachers on ECCD, preschool education/teaching strategies and production of teaching devices are called for. District supervisors and coordinators of specialized areas reiterate the same need; Develop and implement developmentally-appropriate curriculum, learning materials and creative activities for Grade 1; The development of Standards for Learning Competencies in ECCD must consider that majority of our children do not access ECE programs prior to entering primary school (despite the delivery of DCS and of the new National Preschool Education program). Therefore, the learning competencies the National ECCDCC sets for the 6 year olds must provide more time for them to acquire such in Grade 1. Many Grade 1 teachers are still apprehensive that the 8-week curriculum would infringe on their budget of time to work on the present Grade 1 curriculum. They often mention the “No read, no move” policy for Grade 1 children; and the total development of children, not preparation for elementary schooling alone, is the imperative of all early education programs, including Early Childhood Experiences in Grade 1.
7.5 Promote a Policy of Child Weaning at the ECE Stage
Field observations revealed that most of the parents stayed with their children during the entire session of the DCCs. As a consequence, children are unable to develop the sense on independence and confidence to do the ECE activities without the presence of their parents. This attitude hampers the smooth transition of the children’s learning process from ECE to Grade 1. It is suggested here that parent should be discouraged from staying within the premises of the Day Care Centers during session hours.
7.6 Technologically Appropriate Monitoring System
For a monitoring system to work efficiently for ECCD, there are three basic elements to be considered: the data requirements; the repository; and the system of processing and retrieval.
For the data requirements, it is critical to structure the data set by the critical age group. Again, the nutrition case can be cited to drive the point. It was established that the initial report of low malnutrition was based on a statistical report of all children between zero to six. It is argued here that aggregating children from zero to six years old would distort that true picture of the children’s nutritional status. The incidence of malnutrition among infants would be very low. This, in effect distorts the true picture by pulling the central tendency measures downwards. This is the reason why the report indicated a low incidence of malnutrition. It is suggested here that the data system should be stratified according to a more reasonable age grouping so as not to distort the general character of the population.
The other is the repository of the data. Since the crucial integration and convergence of ECCD services is at the barangay level, then the barangay
103
ECCD committee should have a handle of the data sets at their level. Hence, a system must be instituted at the barangay level which could be designed for aggregation at the municipal, provincial, and national level.
However, an ECCD implementor must know that a typical rural barangay would be at least five years away from maintaining a computer that could be host to an ECCD monitoring system on a day-to-day basis. Further, the system would need the presence of a qualified staff with functional knowledge on basic database computer applications. A barangay should have the internal capacity to maintain a computer system. Computers made available to remote barangays would have a life-span of about six months. Hence, it is suggested that at an early stage, it may not be necessary or appropriate for a barangay to set up an electronic data system. At the barangay level, an index card system could work. The level of aggregation in electronic form can be done at the municipal level.
Furthermore a monitoring system should encompass indicators to measure both performance and impact. For the former, the data capture instruments should be simple enough to allow for easy and systematic encoding, storage, processing and analysis. For the latter, the system should built-in benchmark indicators that are generated on a longitudinal perspective.
7.7 Tap parents to assist Day Care Workers
It was observed that many parents stay with their children during day care sessions. This pool of manpower resources can be tapped to assist in the day care activities. However, to be consistent with the concept of developing an independent child, the parents can be involved in specific tasks in the day care sessions on a staggered schedule so that only about two to three parents can be involved in any given day care activities.
7.8 Convergence of ECCD Services
One of the critical added values of ECCD relative to the prior ECCD laws is its mandate to affect the convergence of ECCD services. However, at this point, the concept of convergence is still not internalized. Hence, there is no convergence in the implementation of the services.
It is suggested that in the short run, there is a need for a massive reorientation of the service providers and stakeholders on the concept of convergence particularly in relation to and its difference from an integrated ECCD services. There is also a need, in the short run, to organize a referral system so that the ECCD services can converge to a certain child or better still to a specific household. In the long run, a better approach to allow for the convergence of ECCD services is to have an inventory and needs assessment at the household level so that ECCD services can be tailored to fit and converge to a specific household. Also, in facility development, convergence of services can be enhanced if a one-stop ECCD shop can be the basis for the development of ECCD facilities
7.9 Flexible Equity Policy
As with the other programs of the government, the equity of the LGU should be based on its capacity to pay. Most often, high incidence of malnutrition and infant and under-five mortality is high in municipalities belonging to 5th and 6th class
104
municipalities, thus, these are the ones in need of assistance. For them to be able to participate, there is a need to either waive or adjust the equity requirement.
7.10 Tapping Alternative Fund Conduits at the Community Level
To instill a sense of ownership to the program by the local stakeholders, there is a need to engage the community in the identification and implementation of ECCD including the “power of the purse”. However, this has to be done in a way so as not to allow for the political factors to dominate in the decision making process. The “KALAHI” experience can be replicated under ECCD, where peoples’ organizations were established and were utilized as conduits of the interventions under the program.
7.11 Advocacy program for ECCD
There is a need to enhance the information, communication and education activities of the ECCD. This can be done through posting of signages in strategic areas in ECCD communities; development of IEC materials; and holding of slogan, logo, and essay writing contests.
7.12 Provision of Adequate and Development of Appropriate Learning Material
The ECCD law is explicit in its provision that the medium of instruction should be based on the local dialects. Further, the law stipulates that learning materials should be develop based on local situations. It is argued here that while adequacy of learning materials is necessary, it is not sufficient to address the learning constraints. The learning process can be facilitated if the learning competencies and values are embedded into materials based on local anecdotes and folklores.
7.13 Research Agenda
One of the most fundamental issues that was abstracted in the review was the apparent tension between the original guiding principle of the Day Care Center, which was to cater to the needs of the working parents vis a vis the trend in the demand of the non-working parents of day care children to use the center as the transition towards elementary education. This must be investigated systematically in order to draw more precise policy prescriptions.
105
REFERENCES
Bautista, Violeta, A. Roldan. No date. Surviving The Oods: Finding Hope in Abused Children’s Life Stories. UP-CIDS/PST.
Canlas, Dante, Philippines Midterm Progress Report on the Millennium Development Goals. http://www.neda.gov.ph/econreports.dbs/ MDGs/midterm/ Midterm% 20 MDG%20 Progress%20Report.pdf
Department of Health. 2000, Philippine Health Survey. http://www./eccd/ health% 20situation/ immunizable.htm
Department of Health. various years. Field Health Service Information System (FHSIS). Manila.
______2006. Family Planning Survey. Manila.
DOST-FNRI NNS. various years. Regional Updating of the Nutritional Status of Children.
Gordoncillo, PU., CV Barba, C.V., MM. Paunlagui, MT Talavera, NP. Goroncillo, MR Dy, RJ de Jesús, E Solivas, LA Soliven and AE Gana. 2006. The Effects of Early Childhood Intervetions on Children’s Physiological, Cognitive and Social Development: The Endline Indicators Study. UPLB Foundation, Inc.
Kennedy, G., G. Nantel, P. Shetty. 2006. Assessment of the Double Burden of Malnutrition in Six Case Study Countries. FAO Food and Nutrition Paper 84. p. 2- 20
National Statistics Office. No date. Population of preschool children by single age group, Philippines: 2000-2007 (in millions).
Ocampo, D., R. Ruda, R. A. Dario. A Case Study on Integrated Early Childhood Care and Development (IECCD) National Development Processes: The Philippines Experience. Education Research Program UP Center for Integrative and Development Studies
Pedro , MRA, RC Benavides, CVC Barba. 2006. “Dietary Changes and their Health Implications in the Philippines.” In The Double Burden of Malnutrition – Case Studies from Six Developing Countries. FAO Food and Nutrition Paper 84. p.206- 257
Pedro, MRA, RL Cheong, JR Madriaga, and CVC Barba. 2002. The Philippines Vitamin A Supplementation Program: Indicative Impact, Policy, and Program Implications (Draft). FNRI-DOST. Manila.
Tuazon, MAG and RCF Habito. Undated. The National Salt Iodization Program, the Philippines. http://inffoundation.org/pdf/phillipines%20IDD.pdf
UNESCAP. 2006. Population Data Sheet: Education For Every Child.
UNESCO. 2004. Early Childhood and Education in South-East Asia: Working for Access, Quality and Inclusion in Thailand, the Philippines and Vietnam. Bangkok: UNESCO. 102p.
106 Table 3.1.1.5.
Age group/sex
6-11 months 1 year UNICEF. 2002. Ours to Protect and Nurture: The Case of Children Needing Special Protection. DLSU Social Development Research Center, National Project on Street Children 2002 UNICEF Manila Philippines
UP Population Institute. various years. National Demographic and Health Survey: 1993, 1998 and 2003.
107