Association of Professors of Dermatology QUALITY MATRIX ASSESSMENT FORM
Resident: ______Derm Yr: ___
Evaluator: ______Date(s) : ______
Matrix Topic:
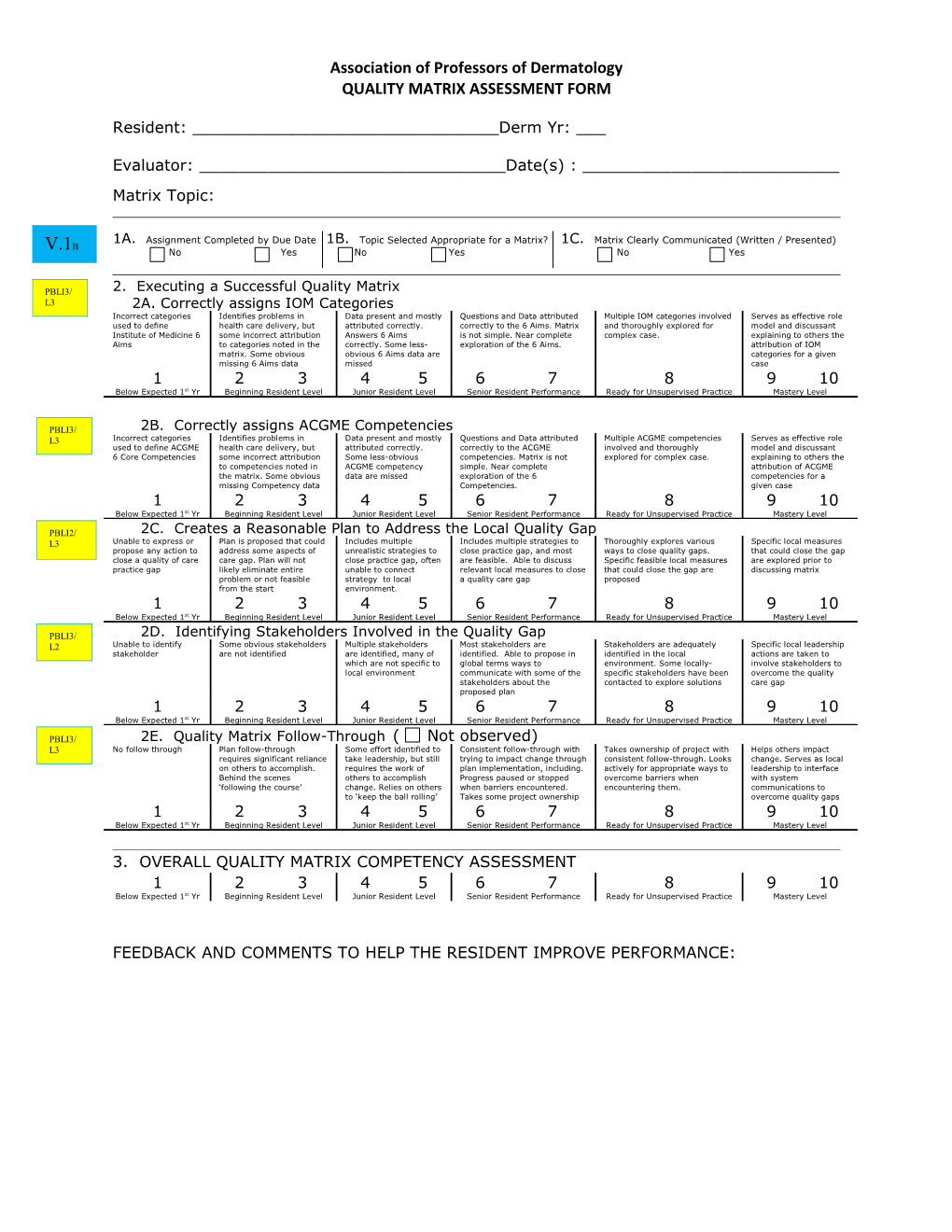
1A. Assignment Completed by Due Date 1B. Topic Selected Appropriate for a Matrix? 1C. Matrix Clearly Communicated (Written / Presented) B V.1 No Yes No Yes No Yes
PBLI3/ 2. Executing a Successful Quality Matrix L3 2A. Correctly assigns IOM Categories Incorrect categories Identifies problems in Data present and mostly Questions and Data attributed Multiple IOM categories involved Serves as effective role used to define health care delivery, but attributed correctly. correctly to the 6 Aims. Matrix and thoroughly explored for model and discussant Institute of Medicine 6 some incorrect attribution Answers 6 Aims is not simple. Near complete complex case. explaining to others the Aims to categories noted in the correctly. Some less- exploration of the 6 Aims. attribution of IOM matrix. Some obvious obvious 6 Aims data are categories for a given missing 6 Aims data missed case 1 2 3 4 5 6 7 8 9 10 Below Expected 1st Yr Beginning Resident Level Junior Resident Level Senior Resident Performance Ready for Unsupervised Practice Mastery Level
PBLI3/ 2B. Correctly assigns ACGME Competencies L3 Incorrect categories Identifies problems in Data present and mostly Questions and Data attributed Multiple ACGME competencies Serves as effective role used to define ACGME health care delivery, but attributed correctly. correctly to the ACGME involved and thoroughly model and discussant 6 Core Competencies some incorrect attribution Some less-obvious competencies. Matrix is not explored for complex case. explaining to others the to competencies noted in ACGME competency simple. Near complete attribution of ACGME the matrix. Some obvious data are missed exploration of the 6 competencies for a missing Competency data Competencies. given case 1 2 3 4 5 6 7 8 9 10 Below Expected 1st Yr Beginning Resident Level Junior Resident Level Senior Resident Performance Ready for Unsupervised Practice Mastery Level
PBLI2/ 2C. Creates a Reasonable Plan to Address the Local Quality Gap L3 Unable to express or Plan is proposed that could Includes multiple Includes multiple strategies to Thoroughly explores various Specific local measures propose any action to address some aspects of unrealistic strategies to close practice gap, and most ways to close quality gaps. that could close the gap close a quality of care care gap. Plan will not close practice gap, often are feasible. Able to discuss Specific feasible local measures are explored prior to practice gap likely eliminate entire unable to connect relevant local measures to close that could close the gap are discussing matrix problem or not feasible strategy to local a quality care gap proposed from the start environment. 1 2 3 4 5 6 7 8 9 10 Below Expected 1st Yr Beginning Resident Level Junior Resident Level Senior Resident Performance Ready for Unsupervised Practice Mastery Level
PBLI3/ 2D. Identifying Stakeholders Involved in the Quality Gap L2 Unable to identify Some obvious stakeholders Multiple stakeholders Most stakeholders are Stakeholders are adequately Specific local leadership stakeholder are not identified are identified, many of identified. Able to propose in identified in the local actions are taken to which are not specific to global terms ways to environment. Some locally- involve stakeholders to local environment communicate with some of the specific stakeholders have been overcome the quality stakeholders about the contacted to explore solutions care gap proposed plan 1 2 3 4 5 6 7 8 9 10 Below Expected 1st Yr Beginning Resident Level Junior Resident Level Senior Resident Performance Ready for Unsupervised Practice Mastery Level
PBLI3/ 2E. Quality Matrix Follow-Through ( Not observed) L3 No follow through Plan follow-through Some effort identified to Consistent follow-through with Takes ownership of project with Helps others impact requires significant reliance take leadership, but still trying to impact change through consistent follow-through. Looks change. Serves as local on others to accomplish. requires the work of plan implementation, including. actively for appropriate ways to leadership to interface Behind the scenes others to accomplish Progress paused or stopped overcome barriers when with system ‘following the course’ change. Relies on others when barriers encountered. encountering them. communications to to ‘keep the ball rolling’ Takes some project ownership overcome quality gaps 1 2 3 4 5 6 7 8 9 10 Below Expected 1st Yr Beginning Resident Level Junior Resident Level Senior Resident Performance Ready for Unsupervised Practice Mastery Level
3. OVERALL QUALITY MATRIX COMPETENCY ASSESSMENT 1 2 3 4 5 6 7 8 9 10 Below Expected 1st Yr Beginning Resident Level Junior Resident Level Senior Resident Performance Ready for Unsupervised Practice Mastery Level
FEEDBACK AND COMMENTS TO HELP THE RESIDENT IMPROVE PERFORMANCE: ASSOCIATION OF PROFESSORS OF DERMATOLOGY Quality Matrix Evaluation Exercise
Instructions:
General principles This tool is designed to help assess the resident’s ability to deconstruct a safety or quality issue and explore the event’s root cause. This is an assessment of the resident’s completed verbal presentation and written “Quality Matrix” using the Quality Matrix principles discussed elsewhere. It is appropriate for incidents occurring in an outpatient or inpatient clinical setting. This tool is generally used after a presentation by the resident discussing the quality or safety issues encountered (not for use during the actual event). The evaluation is used to assess the resident’s reflection and insights into the event, and is not meant to assess the quality matrix-triggering event itself. In general, this evaluation should include 2 parts: a presentation where the resident leads discussion regarding the event, and a completed written quality matrix that gets submitted for review and potential incorporation into the resident portfolio as an exhibit of participation in quality and patient safety curriculum. In general, it is advisable to let the trainee know you will be assessing their performance prior to the matrix presentation. Provide direct, specific constructive feedback to the trainee following the presentation and after review of the final written matrix is submitted.
Specific instructions Skills – Rate the trainee on the milestones scale for each skill. It is important to remember that trainees are not being compared relative to other trainees; they are being rated on a continuum; on a scale designed to assess progression of skills from novice to master. It is common for first year residents to score 3 or 4 out of 10 and still be great first year residents. If a particular skill is not observed, check the “Not observed” box. Feedback and comments – Note specific positives in the encounter and give constructive feedback on how the trainee could improve. The Quality Matrix Template is found on the next page Health Care Matrix: Derm atology Morbidity and M ortality Conference CASE: COMPETENCIES IOM AIMS EFFECTIVE EQUITABLE PATIENT-CENTERED Assessment SAFE (Overuse, TIMELY (Delay in hours, (Outcomes,Evidence- EFFICIENT (Race, Ethnicity, (Preference, Needs, of Care Underuse, Misuse) days, w eeks) Based Care) (Waste of Resources) Gender, SES) Values)
I. Patient Care
II. Medical Know ledge and Skills
IV. Interpersonal and Communication Skills
V. Professionalism
VI. Systems-Based Practice
Improvement
III. Practice-Based Learning and Improvement
Improvement Implementation Pla n III. Practice-Based Learning and Improvement
What are next s teps to m ak e this im provem ent happen?
Who is curre ntly involved?
Who else, if anyone , should be involved?
In w hat tim e fram e should this tak e place?