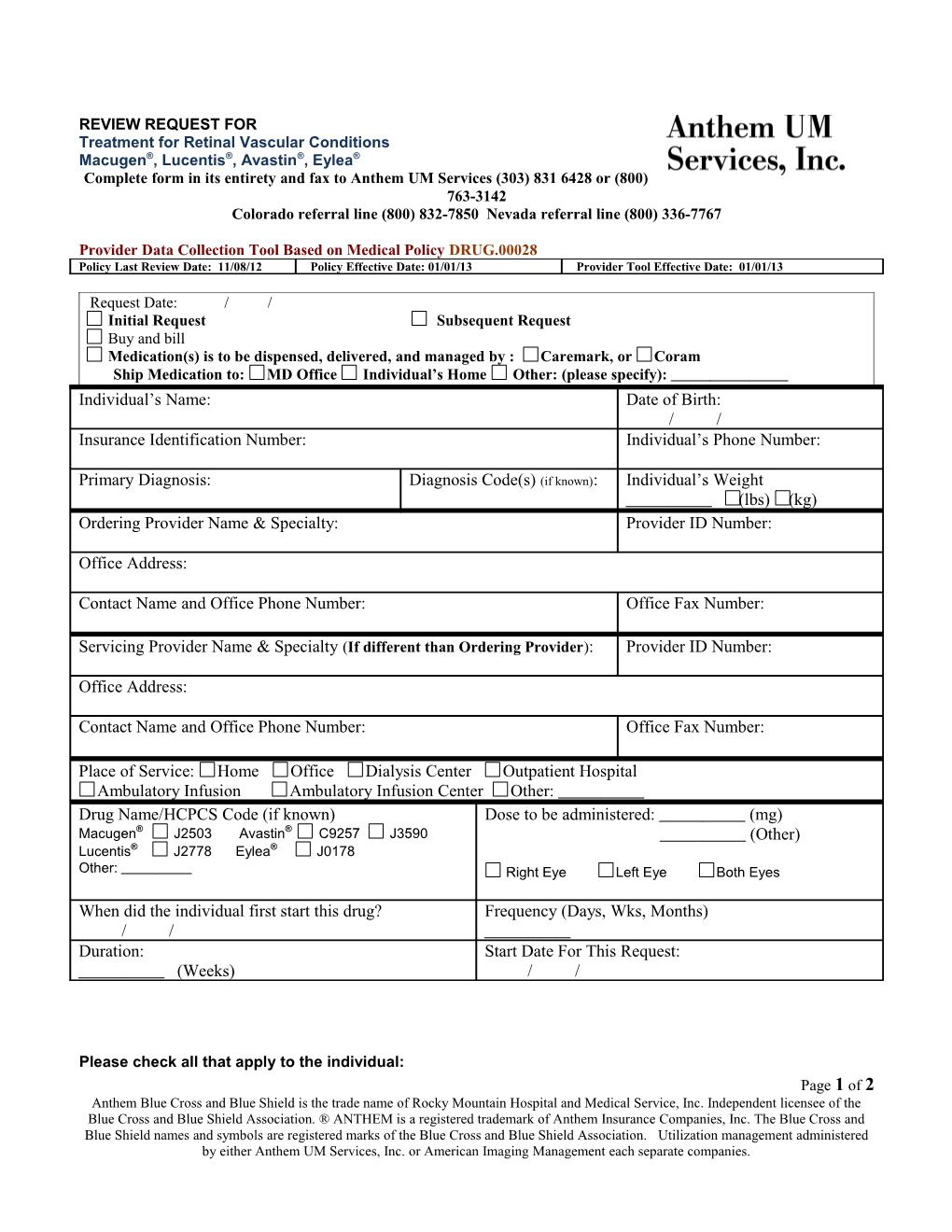
REVIEW REQUEST FOR Treatment for Retinal Vascular Conditions Macugen®, Lucentis®, Avastin®, Eylea® Complete form in its entirety and fax to Anthem UM Services (303) 831 6428 or (800) 763-3142 Colorado referral line (800) 832-7850 Nevada referral line (800) 336-7767
Provider Data Collection Tool Based on Medical Policy DRUG.00028 Policy Last Review Date: 11/08/12 Policy Effective Date: 01/01/13 Provider Tool Effective Date: 01/01/13
Request Date: / / Initial Request Subsequent Request Buy and bill Medication(s) is to be dispensed, delivered, and managed by : Caremark, or Coram Ship Medication to: MD Office Individual’s Home Other: (please specify): Individual’s Name: Date of Birth: / / Insurance Identification Number: Individual’s Phone Number:
Primary Diagnosis: Diagnosis Code(s) (if known): Individual’s Weight (lbs) (kg) Ordering Provider Name & Specialty: Provider ID Number:
Office Address:
Contact Name and Office Phone Number: Office Fax Number:
Servicing Provider Name & Specialty (If different than Ordering Provider): Provider ID Number:
Office Address:
Contact Name and Office Phone Number: Office Fax Number:
Place of Service: Home Office Dialysis Center Outpatient Hospital Ambulatory Infusion Ambulatory Infusion Center Other: Drug Name/HCPCS Code (if known) Dose to be administered: (mg) Macugen® J2503 Avastin® C9257 J3590 (Other) Lucentis® J2778 Eylea® J0178 Other: Right Eye Left Eye Both Eyes
When did the individual first start this drug? Frequency (Days, Wks, Months) / / Duration: Start Date For This Request: (Weeks) / /
Please check all that apply to the individual: Page 1 of 2 Anthem Blue Cross and Blue Shield is the trade name of Rocky Mountain Hospital and Medical Service, Inc. Independent licensee of the Blue Cross and Blue Shield Association. ® ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. The Blue Cross and Blue Shield names and symbols are registered marks of the Blue Cross and Blue Shield Association. Utilization management administered by either Anthem UM Services, Inc. or American Imaging Management each separate companies. Note: To avoid delays, please complete this form in its entirety.
(1) Use of Macugen Individual is diagnosed with established neo-vascular “wet” age-related Macular Degeneration (AMD) Individual is diagnosed with diabetic eye disease Other
(2) Use of Lucentis Individual is diagnosed with one of the following: Individual has diabetic macular edema Individual has established neovascular “wet” AMD Individual has macular edema from branch retinal vein occlusion Individual has macular edema from central retinal vein occlusion
Other
(3) Use of Avastin Individual is diagnosed with one of the following: Individual has diabetic macular edema Individual has established neovascular “wet” AMD Individual has macular edema from branch retinal vein occlusion Individual has macular edema from central retinal vein occlusion Individual has neovascular glaucoma Individual has other rare causes of choroidal neovascularization for one or more of the following conditions: angioid streaks choroiditis (including, but not limited to histoplasmosis induced choroiditis) degenerative idiopathic myopia retinal dystrophies trauma Individual has pseudoxanthoma elasticum Individual has retinopathy of prematurity Other
(4) Use of Aflibercept (Eylea) Individual is diagnosed with one of the following: Individual has established neo-vascular “wet” age-related Macular Degeneration (AMD) Individual has macular edema following central retinal vein occlusion Individual has macular edema following branch retinal vein occlusion Other:
This request is being submitted: Pre-Claim Post–Claim. If checked, please attach the claim or indicate the claim number
I attest the information provided is true and accurate to the best of my knowledge. I understand that the health plan or its designee may perform a routine audit and request the medical documentation to verify the accuracy of the information reported on this form.
/ / Name & Title of Provider or Provider Representative Completing Form Date & attestation (Please Print)* *The attestation fields must be completed by a provider or provider representative in order for the tool to be accepted
Page 2 of 2 Anthem Blue Cross and Blue Shield is the trade name of Rocky Mountain Hospital and Medical Service, Inc. Independent licensee of the Blue Cross and Blue Shield Association. ® ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. The Blue Cross and Blue Shield names and symbols are registered marks of the Blue Cross and Blue Shield Association. Utilization management administered by either Anthem UM Services, Inc. or American Imaging Management each separate companies.