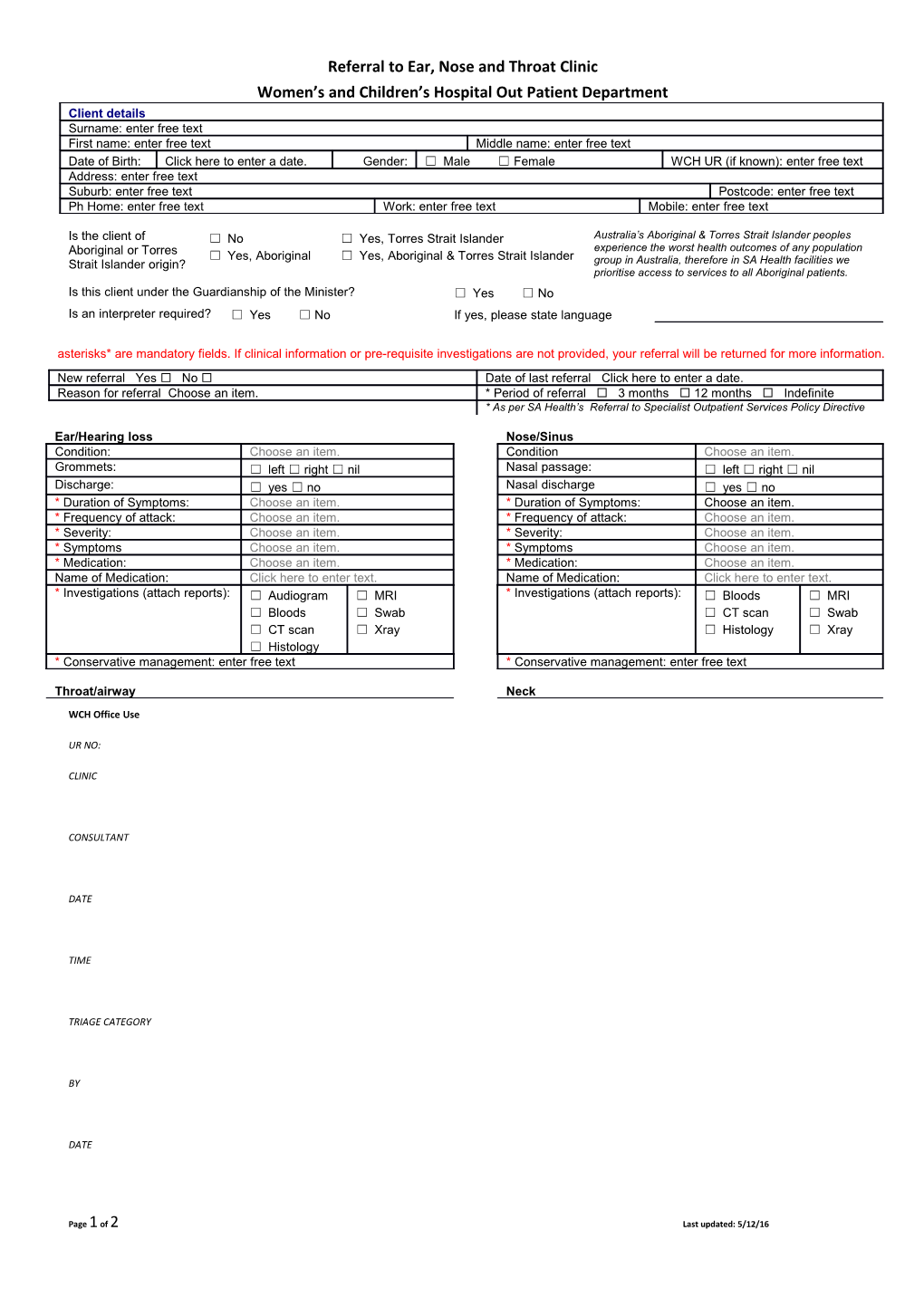
Referral to Ear, Nose and Throat Clinic Women’s and Children’s Hospital Out Patient Department Client details Surname: enter free text First name: enter free text Middle name: enter free text Date of Birth: Click here to enter a date. Gender: ☐ Male ☐ Female WCH UR (if known): enter free text Address: enter free text Suburb: enter free text Postcode: enter free text Ph Home: enter free text Work: enter free text Mobile: enter free text
Is the client of ☐ No ☐ Yes, Torres Strait Islander Australia’s Aboriginal & Torres Strait Islander peoples experience the worst health outcomes of any population Aboriginal or Torres ☐ Yes, Aboriginal ☐ Yes, Aboriginal & Torres Strait Islander Strait Islander origin? group in Australia, therefore in SA Health facilities we prioritise access to services to all Aboriginal patients. Is this client under the Guardianship of the Minister? ☐ Yes ☐ No Is an interpreter required? ☐ Yes ☐ No If yes, please state language
asterisks* are mandatory fields. If clinical information or pre-requisite investigations are not provided, your referral will be returned for more information. New referral Yes No Date of last referral Click here to enter a date. Reason for referral Choose an item. * Period of referral 3 months 12 months Indefinite * As per SA Health’s Referral to Specialist Outpatient Services Policy Directive
Ear/Hearing loss Nose/Sinus Condition: Choose an item. Condition Choose an item. Grommets: ☐ left ☐ right ☐ nil Nasal passage: ☐ left ☐ right ☐ nil Discharge: ☐ yes ☐ no Nasal discharge ☐ yes ☐ no * Duration of Symptoms: Choose an item. * Duration of Symptoms: Choose an item. * Frequency of attack: Choose an item. * Frequency of attack: Choose an item. * Severity: Choose an item. * Severity: Choose an item. * Symptoms Choose an item. * Symptoms Choose an item. * Medication: Choose an item. * Medication: Choose an item. Name of Medication: Click here to enter text. Name of Medication: Click here to enter text. * Investigations (attach reports): ☐ Audiogram ☐ MRI * Investigations (attach reports): ☐ Bloods ☐ MRI ☐ Bloods ☐ Swab ☐ CT scan ☐ Swab ☐ CT scan ☐ Xray ☐ Histology ☐ Xray ☐ Histology * Conservative management: enter free text * Conservative management: enter free text
Throat/airway Neck
WCH Office Use
UR NO:
CLINIC
CONSULTANT
DATE
TIME
TRIAGE CATEGORY
BY
DATE
Page 1 of 2 Last updated: 5/12/16 Referral to Ear, Nose and Throat Clinic Women’s and Children’s Hospital Out Patient Department Condition: Choose an item. Condition Choose an item. Position/side: ☐ left ☐ right ☐ n/a Position/side ☐ left ☐ right ☐ nil * Duration of Symptoms: Choose an item. * Duration of Symptoms: Choose an item. * Frequency of attack: Choose an item. * Severity: Choose an item. * Severity: Choose an item. * Symptoms Choose an item. * Symptoms Choose an item. * Medication: Choose an item. * Medication: Choose an item. Name of Medication: Click here to enter text. Name of Medication: Click here to enter text. * Investigations (attach reports): ☐ Ba Swallow ☐ MRI * Investigations (attach reports): ☐ Ba ☐ MRI ☐ Bloods ☐ Swab Swallow ☐ Histology ☐ CT scan ☐ Xray ☐ Bloods ☐ Xray ☐ Endoscopy ☐ CT scan ☐ Endoscopy *Conservative management: enter free text * Conservative management: enter free text
Other information (eg upcoming appointments in other WCH departments): enter free text
Medical history: enter free text
Referring Clinic Details Referring Doctor Name: enter free text Provider No. enter free text Surgery Name: enter free text Contact No. enter free text Address: enter free text Suburb: enter free text Postcode: enter free text
Signature ______Date ______Please ensure all fields have been completed, sign & date the form then fax to WCH Administration Hub on 8161 6246
WCH Office Use
UR NO:
CLINIC
CONSULTANT
DATE
TIME
TRIAGE CATEGORY
BY
DATE
Page 2 of 2 Last updated: 5/12/16