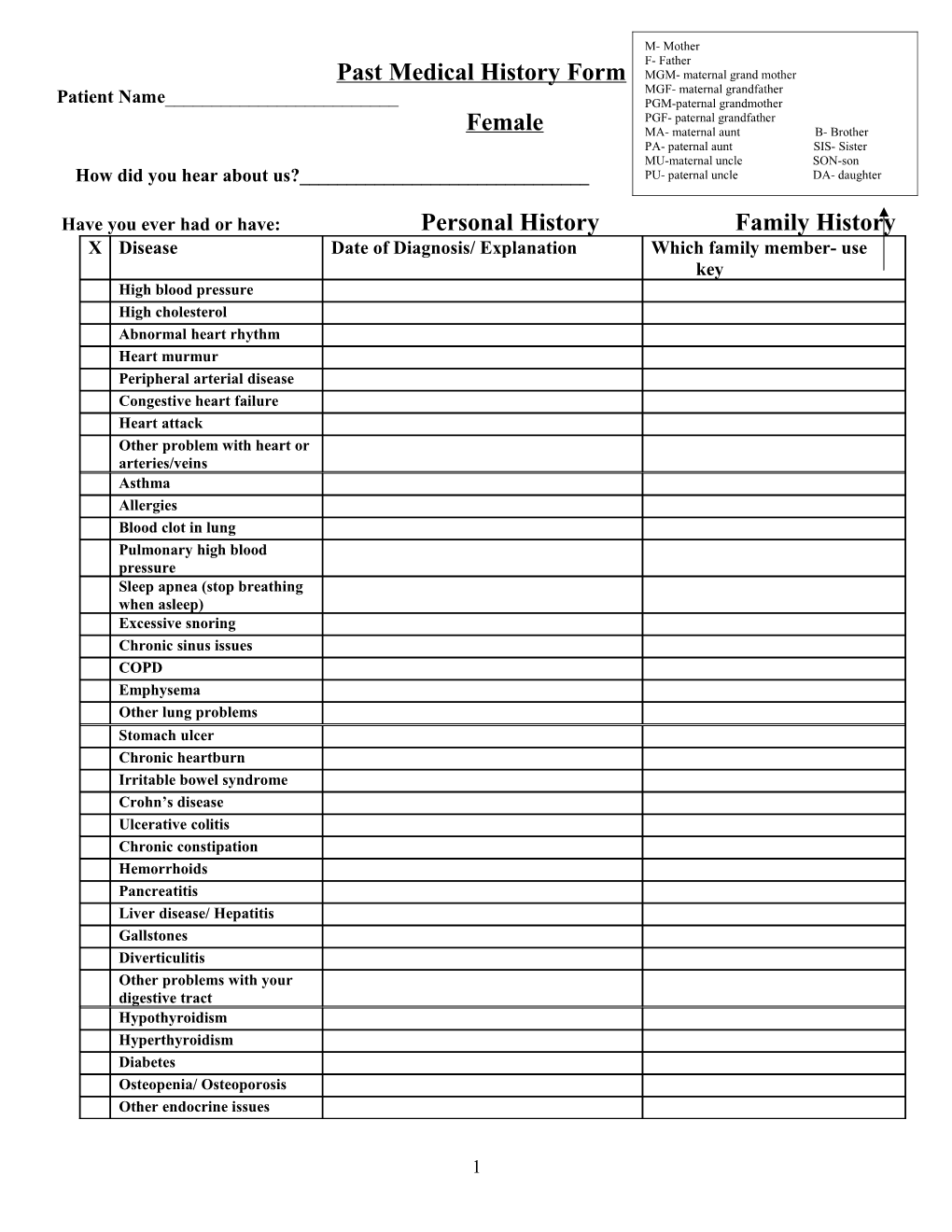
M- Mother F- Father Past Medical History Form MGM- maternal grand mother MGF- maternal grandfather Patient Name______PGM-paternal grandmother PGF- paternal grandfather Female MA- maternal aunt B- Brother PA- paternal aunt SIS- Sister MU-maternal uncle SON-son How did you hear about us?______PU- paternal uncle DA- daughter
Have you ever had or have: Personal History Family History X Disease Date of Diagnosis/ Explanation Which family member- use key High blood pressure High cholesterol Abnormal heart rhythm Heart murmur Peripheral arterial disease Congestive heart failure Heart attack Other problem with heart or arteries/veins Asthma Allergies Blood clot in lung Pulmonary high blood pressure Sleep apnea (stop breathing when asleep) Excessive snoring Chronic sinus issues COPD Emphysema Other lung problems Stomach ulcer Chronic heartburn Irritable bowel syndrome Crohn’s disease Ulcerative colitis Chronic constipation Hemorrhoids Pancreatitis Liver disease/ Hepatitis Gallstones Diverticulitis Other problems with your digestive tract Hypothyroidism Hyperthyroidism Diabetes Osteopenia/ Osteoporosis Other endocrine issues
1 X Disease Date of diagnosis/ Explanation Which Family Member Warts Eczema Psoriasis Abnormal moles Seizures Migraines Chronic headaches Stroke or TIA Dementia Other neurological problems Urinary leakage Endometriosis Fertility Problems Uterine Fibroids Poly cystic ovarian disease Sexually transmitted disease Irregular periods Kidney stones Gout Arthritis Rheumatoid arthritis Fractures Lupus Blood transfusion Clotting/ Bleeding issues Anemia What kind Sickle cell trait/ Disease Thalassemia Anxiety Bipolar Disorder Depression ADD/ADHD Substance abuse/inc. alcohol Cancer What type/ treatment Other medical issues not listed
2 Surgeries
X Surgery Date X Surgery Date Tonsillectomy Hysterectomy Tubes in ears Tubal ligation Appendectomy Cataract R/L Gallbladder removal Cosmetic Back Surgery Heart Surgery Joint Surgery Hernia Joint replacement C-section Other Other
Procedures Have you ever had: X Procedure Date X Procedure Date Heart catheterization Mammogram Colonoscopy Bone Density Scan Upper scope (EGD) Prostate Check or PSA Echocardiogram
Gyn
How old were you with your first period?
Are you (or have you ever been) sexually active? Y N
Age of Menopause Do you have sex with men, women or both? What type of birth control do you use? How many Total pregnancies have you had? Total # (including miscar/abortions)
Deliveries # Miscar # Abortions #
Last Pap Smear: Abnormal Pap? (date and treatment) Do you perform self breast exams regularly? Y N Have you had a mammogram? Y N Last date: Any abnormal mammo? Have you had a bone density scan? Y N Date and result: Have you had Gardasil vaccines? Y N Dates: Date of last tetanus booster?
3 Social
Occupation: Highest level of education: Marital Status: Single Partner(girlfriend/boyfriend) Engaged Married Divorced Widowed Number of children: Biological: Stepchildren: Adopted: Do you live by yourself or with others? Exercise level? None 1-2/week 3-4/week 5-7/week How many alcoholic drinks per week? Never Rare 0-3 4-6 7-10 11-14 >14 Have you ever had a problem with alcohol Y N use? Diet Regular Vegetarian Vegan Gluten-free Other
General Stress Level Low Medium High Have you ever smoked? Current? How much? How long? Past? How much? How long? Smokeless tobacco? Cur/Past? How much/ How long? Regular use of marijuana? Other illicit drugs? Any problems with controlled substances? Past/Present? Like prescription medications? Any problems with drug use? Y N
Do you drink caffeine? How much per Soda? (Diet) # (Sugar)# Coffee # Tea# Energy Drinks# day?
Safety
Do you use seatbelts regularly? Do you use sunscreen regularly? Do you have guns present in the home? If so are they locked away from children? Do you have a smoke alarm at home? Do you wear a bike helmet? Any history of domestic violence? Any history of sexual violence?
Personal
4 Do you have any pets?
What do you like to do for fun or pass time?
Other things that you would like to share about yourself?
Medication Allergies/Food Allergies/Contact Allergies
Medication/Food/Contact Reaction
Current Medications Please list reason for taking each medication
1. ______5. ______
2. ______6. ______
3. ______7. ______
4. ______8. ______
Vitamins/ Supplements
1. ______3. ______
2. ______4. ______
Past Medications
Medication Reason for taking Medication Reason for taking
Health Goals Please list health goals that you would like to reach for yourself
1. 2. 3. 5 4. 5. Female Review of Systems Please circle recent symptoms and use lines below to explain. List #. 1. Constitutional: fatigue, poorly (malaise), fever, night sweats, weight gain or loss that doesn’t make sense
2. Eyes: dry eyes , irritation , vision change , discharge from eyes , foreign body sensation in eyes
3. Ears: ear pain, ear congestion, ears popping, discharge from the ears, difficulty hearing
4. Nose: nasal congestion, nasal discharge, post-nasal drip, maxillary sinus pain, frontal sinus pain
5. Mouth/Throat: sore throat, snoring, mouth ulcer, teeth abnormalities
6. Cardiovascular: chest pain, shortness of breath when lying down, rapid or irregular heartbeat (palpitations), excessive sweating
7. Respiratory: cough, wheezing, shortness of breath
8. Gastrointestinal: heartburn, nausea, vomiting, diarrhea, constipation, abdominal pain, bloating
9. Genitourinary: pain with urination, urine leakage, foul-smelling urine, increased urinary frequency, blood in urine, abnormal vaginal discharge, abnormal periods
10. Musculoskeletal: muscle aches, muscle weakness, joint pain, back pain
11. Skin: abnormal moles, rash, abnormal skin lesions, breast lump, change in the breast skin
12. Neurologic: headaches, dizziness, weakness, numbness
13. Psych depression , anxiety , sleep disturbances , mania , feeling unsafe in relationship , alcohol or substance abuse , difficulty falling asleep , early morning waking , not feeling rested after adequate sleep, loss of interest in activities , loss of pleasure from usual activities , inappropriate feelings of guilt , decreased energy , decreased motivation , decreased concentrating ability , abnormal appetite, feeling like hurting self, feeling so badly that you wouldn’t mind if you died in your sleep, feeling actively suicidal, feeling emotionally detached , feeling unique and all-powerful (grandeur) , disturbing or unusual thoughts, feelings, or sensations , decreased need for sleep , impulsive behavior , pressured speech , causing anger in friends and family
14. Endocrine: change in weight distribution , increased hair loss , excessively dry skin , change in color of skin , feelings of weakness and fatigue , feeling more hot or cold than others , hot flashes , abnormal hair growth ,
15. Hematologic/Lymphatic swollen glands, abnormal bruising
16. Allergies: runny nose, sinus pressure, itching, hives, frequent sneezing
6 Allergy Questionnaire - Intake Questions To Be filled Out By Patient
Patient Name______Date______
Reviewed by______
1. Do you experience any of these symptoms more than twice per year: Cough, cold, congestion, difficulty breathing, headaches, wheezing, runny nose, sore throat, itchy/irritated eyes, sinus pain, ear pain, unexplained fatigue, skin irritation, snoring? Yes No
2. Have you ever been diagnosed with asthma or bronchitis? Yes No
3. Do You experience symptoms or allergies? Yes No
7 Name______DOB ______I give Highlands Health For Life permission to access my medication history electronically from the pharmacy.
_____I do not give Highlands Health For Life permission to access my medication history electronically from the pharmacy.
8 Highlands Health For Life Whitney Kennedy M.D.
Please Print: How did you hear about us?______
Patient Name______Birth Date______
Present Address______Apt#______
City______State______Zip______
Telephone______Cell______Marital Status______
Can we leave medical messages on your voice mail? Yes No Which Phone?______
E-mail______Patient Soc. Sec. #______
Occupation______Employer______
Work Phone______Pharmacy phone #______
In case of emergency please notify:
Emergency Contact Name______Relation______
Telephone 1)______2)______
Parent or Guardian (if patient is a child)______
Telephone______Cell______Work#______
Insurance Info
Insurance Company______Secondary Insurance______
9 Name of policy Holder (specify primary or secondary insurance)______
Birth Date of Policy Holder______
SSN# of Policy Holder______
Relationship to Patient______
Highlands Health For Life Whitney Kennedy M.D.
Name of Practice: Highlands Health For Life
Name of Patient: ______Date of Birth: ______
Acknowledgement of Notice of Privacy Practices
I hereby acknowledge that I have read Highlands Health For Life’s Notice of Privacy Practices
______Signature of patient or patient representative Date Documentation of Good Faith Efforts To obtain patients acknowkedgement that they received provider’s Notice of Privacy Practices
(For use when patient cannot obtain acknowledgement)
The patient presented to the office on ______and was provided with a copy of Highlands Health For Life’s Notice of Privacy Practices. A good faith effort was made to obtain from the patient a written acknowledgement of his/her receipt of the notice. However, such acknowledgement was not obtained because of the following reason:
Patient refused to sign
Patient was unable to sign or initial because:
10 The patient had medical emergency, and an attempt to obtain the acknowledgement will be made at the next available opportunity
Other reason:
______
Signature of Employee Completing Form Date
Highlands Health for Life Payment Terms and Agreements
I, the undersigned, in consideration for services rendered to the patient by Highlands Health for Life, understand and agree to the following:
1. I understand that payment for charges is due on the date of service with the exception of insurance carriers for which Highlands Health for Life is under contract to file directly.
2. I understand that my insurance coverage may not provide payment for all charges incurred in obtaining treatment from Highlands Health for Life. I will be responsible for any co-payment, deductible or service not covered by my insurance provider. If I do not have insurance coverage for services rendered by Highlands Health for Life, I agree to pay all charges resulting from such services.
3. I hereby authorize Highlands Health for Life to file with my insurance carrier and I assign payment of medical benefits to Highlands Health for Life.
4. I authorize release of any and all medical records and information necessary to process any claim generated by services I receive in this office. 11 5. I will keep my account current as to charges for which I am responsible. In the event that I fail to pay charges, Highlands Health for Life is entitled to take whatever action necessary to collect such charges and I will be responsible for reasonable attorney’s fees and costs incurred as a result of such collection.
My signature below indicates that I have read and agree to the terms set above.
Patient Name: ______
Signature: ______
Date: ______
HIGHLANDS HEALTH FOR LIFE IS PLEASED TO INTRODUCE OUR NEW INTERNET SERVICE – THE PATIENT PORTAL!
The Patient Portal is a secure web portal on our web site home page that gives patients a new and efficient internet-based method of communicating with their doctor’s office. Patients can log on to www.highlandshealthforlife.com and: Send and receive secure and confidential messages with our office
Request Appointments
Request Prescription Refills
View Upcoming Appointments
12 Update Your Personal Information
Print Useful Paperwork and Forms
See Your Lab Results
IT’S SIMPLE AND EASY TO ACCESS YOUR PATIENT PORTAL: 1) Log onto our website at: www.highlandshealthforlife.com
2) Click on the Patient Portal link
3) Register. Make sure to use your primary phone number that we have in your chart when registering
4) Log in and follow the directions
(If you experience difficulty when registering, please call our office at 303-381-3700 during normal business hours for assistance.)
Highlands Health for Life
As a courtesy to our patients and to improve the speed and quality of our testing process, our office uses ResultsCall to deliver your confidential Test Results.
13 Once your results are reviewed, our system will notify you that your test results are available for retrieval. At that time you do not need to call our office to pick up the results of your tests; simply follow the instructions below to access your test results any time of the day or night.
To Access Your Test Results by Phone:
1) Dial the ResultsCall toll-free access number: 877-290-5950
2) Enter your 5-13 numeric digit PIN (This is the number you created while registering for the Patient Portal)
3) When prompted for your four-digit date of birth, enter two digits for the month and two digits for the day. (Example: September 4th would be entered 0904)
4) When prompted for your phone number, enter your 10 digit telephone number, which includes your area code. This should be the same number we used to notify you that your results are ready for retrieval.
5) If you have tried to retrieve your test results before being notified by ResultsCall and the system does not recognize your PIN or other personal identifier numbers, this means your test results are not ready for retrieval. Please try calling a bit later. Retrieving your results via the Internet:
Go to our website at www.highlandshealthforlife.com and log on/ register for the Patient Portal
To Log In:
1) Enter your 5-13 numeric digit PIN. (This is the number you created while registering for the Patient Portal)
2) Enter your eight-digit date of birth, using two digits for the month, two digits for the day, and four digits for the year. (Example: September 4th, 1980 would be entered 09/04/1980)
3) Enter your 10-digit telephone number, which includes your area code. This should be the same number we used to notify you that your results are ready for retrieval.
4) Click the Login button. To Register:
1) Click on New User Registration
2) Enter your First Name, Last Name, Date of Birth, and Primary Phone Number, and proceed as directed. Your Test Results will be available as a message on your Portal Welcome screen, as well as within the Lab Results section of My Health – Labs/Imaging
We hope you will find this new system helpful. If you encounter any problems with the system, please call our office at 303-381-3700.
Thank you
14 Highlands Health for Life Notice of Patient Privacy Practices (Condensed Version)
This notice describes how medical information about you may be used and disclosed and how you can get access to this information. Please review it carefully. Use and Disclosures: Highlands Health for Life is permitted to use and disclose your private and confidential health information for treatment, payment and healthcare operations of the practice. Fro example, the practice may disclose your protected health information to other physicians to facilitate treatment, and the practice may use health information about you so that the practice may bill and collect payment from an insurance company, health plan, or other third party payor. The practice may disclose your health information to review treatment and services to evaluate performance of practice staff and other management and administrative purposes. In addition, the practice may use or disclose your protected health information, which is incident to a permitted use of disclosure. “Protected Health Information” is information about you that may identify you and relate to your past, present, or future physical or mental health or condition and related health services. Use and disclosures requiring an opportunity for you to agree or object: The practice may use and disclose your health information in the following instances. In each of the examples, you have the opportunity to agree or prohibit or restrict the use or disclosure. If you are not present or able to agree or object to the use or disclosure, the practice may determine whether the disclosure is in your best interest. Emergency disclosures may also be made- due to your incapacity or emergency treatment situation- if disclosure is consistent with your prior expressed preference and in your best interest as determined by the practice. Family Members: Unless you object, the practice will disclose your health information to a family member, other relative, close friend, or other person you identify; such information disclosed will be directly relevant to such person’s involvement with your health care. If you are unable or unavailable to agree or object, the practice may disclose information necessary if the practice determines it is in your best interest. The practice may use or disclose information to notify, or assist in the notification of (including identifying or locating) a family member, your personal representative or other responsible person for your care, your address or phone number, general condition, or death. Disclosures made without your authorization or consent: The following is a description of other purposes for which the practice is permitted or required to use or disclose your protected health information without your consent, authorization or your opportunity to object; this is not a complete list of all possible disclosures.
1. By the practice for training or to defend itself in a legal action or other proceeding brought by you. 2. For public health activities, social service or protective service agencies, and to a health oversight agency for oversight activities. 3. In the course of any judicial or administrative proceeding and for law enforcement purposes. 4. For identifying a deceased person, and to organ procurement organizations. 5. As authorized to comply with laws relating to workers; compensation, or similar programs, that provide benefits for workplace injuries.
Other uses and disclosures will be made only with your written authorization, and you may revoke such authorization at any time, provided that the revocation is in writing, except that (i) the practice has taken action in reliance thereon; or (ii) if the authorization was obtained as a condition of obtaining insurance coverage, other law provides the insurer with the right to contest a claim under the policy or the policy itself. Certain Uses Or Disclosures: The practice may contact you to provide appointment reminders or information about treatment alternatives or other health-related benefits and services that may be of interest to you. Individual Rights: The following are statements of your privacy rights. In each case, you may exercise these rights by filing a written request to the privacy contact listed below.
A. You have the right to request restrictions on certain uses and disclosures of your protected health information; the practice is not required to agree to a requested restriction. B. You have the right to receive confidential communications of your protected health information. C. You have the right to inspect and copy your protected health information. D. You have the right to amend your protected health information. E. You have the right to receive an accounting of certain disclosures of your protected health information. F. You have the right to obtain a paper copy of this notice from the practice. Practice Duties:
A. The practice is required by law to maintain the privacy of your protected health information and to provide you with this notice of its legal duties and privacy practices with respect to protected health information. B. The practice is required to abide by the terms of the privacy notice currently in effect. C. The practice reserves the right to change the terms of its privacy notice and to make the new notice provisions effective for all protected health information that practice maintains. Any such revised notice shall be provided to individuals in the same manner this notice is given. Complaints and Contact: If you believe that your HIPAA privacy rights have been violated, you may make a written complaint by delivery to the practice. You will not be retaliated against if you file a complaint. You should file your complaint at the following address and you may also request further information by written request to:
Whitney Kennedy M.D. Highlands Health For Life 4104 Tejon St. Denver, CO 80211 Effective Date: This Privacy Notice is effective April 14, 2003 *** The Notice of Privacy Practices in its entirety is available upon request. 15 16