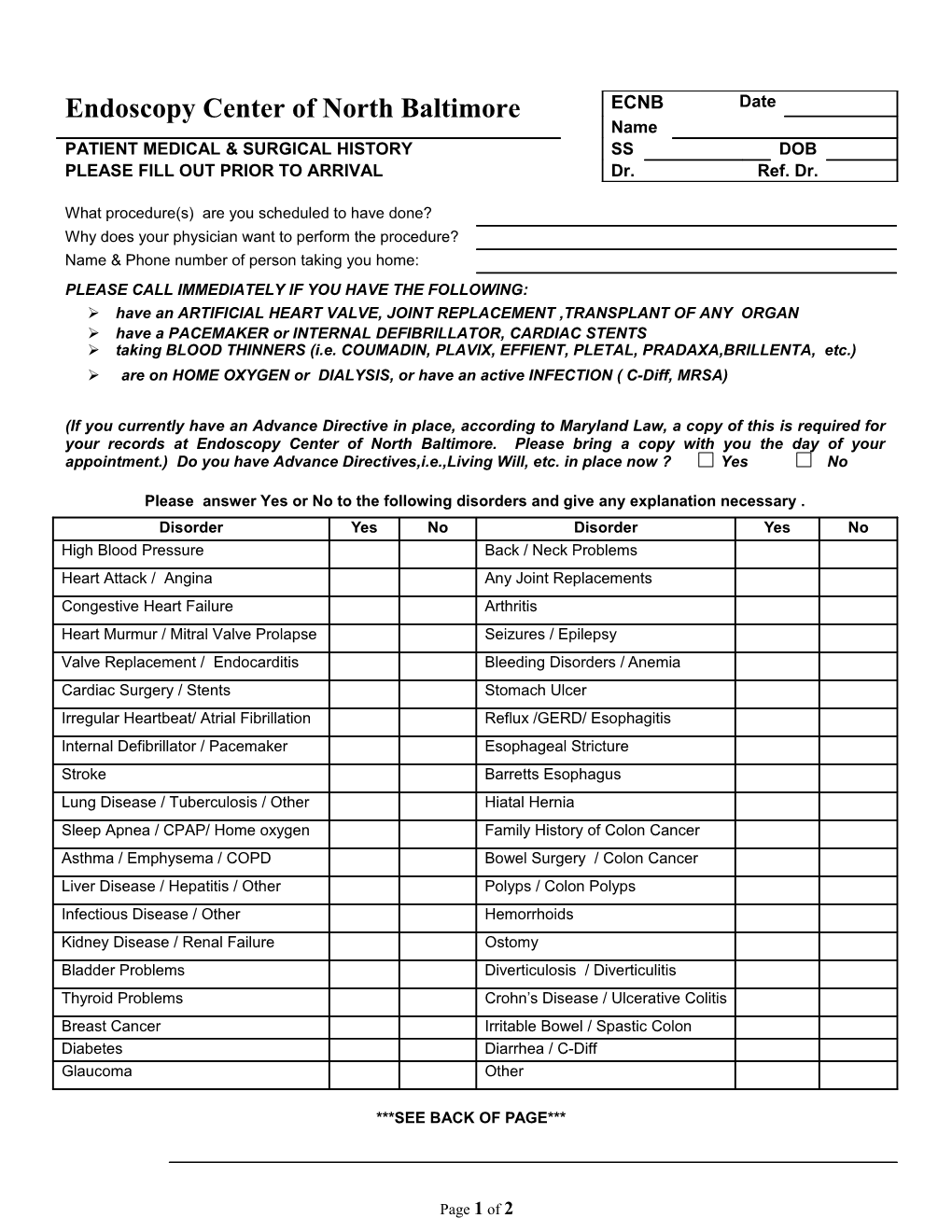
Endoscopy Center of North Baltimore ECNB Date Name PATIENT MEDICAL & SURGICAL HISTORY SS DOB PLEASE FILL OUT PRIOR TO ARRIVAL Dr. Ref. Dr.
What procedure(s) are you scheduled to have done? Why does your physician want to perform the procedure? Name & Phone number of person taking you home: PLEASE CALL IMMEDIATELY IF YOU HAVE THE FOLLOWING: have an ARTIFICIAL HEART VALVE, JOINT REPLACEMENT ,TRANSPLANT OF ANY ORGAN have a PACEMAKER or INTERNAL DEFIBRILLATOR, CARDIAC STENTS taking BLOOD THINNERS (i.e. COUMADIN, PLAVIX, EFFIENT, PLETAL, PRADAXA,BRILLENTA, etc.) are on HOME OXYGEN or DIALYSIS, or have an active INFECTION ( C-Diff, MRSA)
(If you currently have an Advance Directive in place, according to Maryland Law, a copy of this is required for your records at Endoscopy Center of North Baltimore. Please bring a copy with you the day of your appointment.) Do you have Advance Directives,i.e.,Living Will, etc. in place now ? Yes No
Please answer Yes or No to the following disorders and give any explanation necessary . Disorder Yes No Disorder Yes No High Blood Pressure Back / Neck Problems Heart Attack / Angina Any Joint Replacements Congestive Heart Failure Arthritis Heart Murmur / Mitral Valve Prolapse Seizures / Epilepsy Valve Replacement / Endocarditis Bleeding Disorders / Anemia Cardiac Surgery / Stents Stomach Ulcer Irregular Heartbeat/ Atrial Fibrillation Reflux /GERD/ Esophagitis Internal Defibrillator / Pacemaker Esophageal Stricture Stroke Barretts Esophagus Lung Disease / Tuberculosis / Other Hiatal Hernia Sleep Apnea / CPAP/ Home oxygen Family History of Colon Cancer Asthma / Emphysema / COPD Bowel Surgery / Colon Cancer Liver Disease / Hepatitis / Other Polyps / Colon Polyps Infectious Disease / Other Hemorrhoids Kidney Disease / Renal Failure Ostomy Bladder Problems Diverticulosis / Diverticulitis Thyroid Problems Crohn’s Disease / Ulcerative Colitis Breast Cancer Irritable Bowel / Spastic Colon Diabetes Diarrhea / C-Diff Glaucoma Other
***SEE BACK OF PAGE***
Page 1 of 2 History/Condition Yes No History/Condition Yes No Any past major surgeries? Allergies/Sensitivity to Please List Below Medication? Please List Below Other medical conditions? Allergies to latex? Female only: Are you pregnant? Allergies to contrast? (IVP Dye) Explanation of above
PLEASE LIST ALL YOUR CURRENT MEDICATIONS. INCLUDE ALL OVER THE COUNTER MEDICATIONS (VITAMINS/ HERBAL) taken on a regular basis. Include if you take ASPIRIN or IBUPROFEN of any kind. Name of Dose Frequency Last Resume after List New Medications added Medicine and Dose procedure? Y/N after procedure Route 1. 1.
2.
3.
4. 2.
5.
6.
7. 3.
8.
9. Copy of Medication List given to patient: Height Weight Have you had any problems with Anesthesia or Intravenous sedation? Yes No Describe On a scale of 0-10 (with 0 being no pain and 10 being very severe) how would you define your level of pain? today? Check if you use any of the following: Alcohol Yes No Quantity per day Tobacco Yes No Quantity per day Narcotics Yes No Quantity per day You will be called 24-72 hours post-procedure. If you are unavailable, may we leave a message on your answering machine or with another party at that number? YES NO By signing this form you acknowledge that ECNB has allowed you full access to all forms of disclosure required by Maryland state law and by any and all organizations requiring various types of disclosure to include, but not restricted to, a Patient’s bill of Rights/Responsibilities, Advance Directives, Disclosure of ownership by our doctors, etc. You also acknowledge that the information you provided on this form is complete and accurate.
Patient Signature: Signature of Reviewing RN: Date
Page 2 of 2