IN-SCHOOL ADOLESCENT GIRLS’ ACCESS TO AND USE OF HEALTH INFORMATION AND ATTITUDE TOWARDS REPRODUCTIVE HEALTH PRACTICES IN LAGOS STATE,
NIGERIA
BY
STELLA NGOZI I. ANASI MATRIC. NO. 69718
A Ph.D POSTFIELD SEMINAR PRESENTED AT THE DEPARTMENT OF LIBRARY, ARCHIVAL AND INFORMATION STUDIES, UNIVERSITY OF IBADAN, IBADAN
SUPERVISOR: DR. K. I. N. NWALO ABSTRACT Adolescent girls in developing countries are known to have inadequate access to reproductive health information which could influence their attitude towards reproductive health practices. This study therefore investigated the relationship between access to and use of health information among in-school adolescent girls and their attitude towards reproductive health practices in Lagos State, Nigeria. The study adopted the descriptive survey research design. A multistage sampling technique was used to select 1800 in-school adolescent girls in six Local Education Districts in Lagos State that constituted the sample. A questionnaire tagged Reproductive Health Information and Attitude of Adolescents Questionnaire (RHIAQ) complemented with focus group discussion, observation and oral interview were instruments used to collect data. Eight research questions and five hypotheses tested at 0.05 level of significance were postulated for the study. Descriptive and inferential statistics were used to analyse the data. The findings revealed that access to reproductive health information correlated significantly with attitude towards reproductive health practices (r = 0.107; P< 0.05). There was no relationship between use of reproductive health information and attitude towards reproductive health practices (r = -.009; P value > 0.05). However, access to and use of reproductive health information correlated significantly with attitude towards reproductive health practices (R= 0.108; P value < 0.05). There was no significant difference in access to reproductive health information between girls in single sex and those in coeducational school (t =1.256; df =1365; P>0.05). There was no significant difference in use of reproductive health information between girls in single sex and those in coeducational school (t = –.496; df =1365; P>0.05). Nevertheless, the results affirmed that only access to reproductive health information predicted attitude towards reproductive health practices ((B =0.054, P< 0.05). The study found that access to and use of reproductive health information is significantly related with in-school adolescent girls’ attitude towards reproductive health practices in Lagos State, Nigeria. Based on the findings of this study, the following recommendations are suggested to improve access to and use of reproductive health information among in-school adolescents. . Regular workshops, seminars, symposia, lectures and talks aimed at promoting access to and use of reproductive health information should be organized for parents, teachers and students. . Multi-media approach should be adopted for the dissemination of reproductive health information in public schools in Lagos State. A blend of interactive strategies geared towards helping adolescent girls to feel comfortable with sexuality-related topics while limiting potential intimidation and embarrassment should be promoted. . The National Comprehensive Sexuality Education curriculum should be implemented in all public secondary schools and this should reflect in the school timetable. The state government should also make specific annual budgetary allocation for the developing and maintaining of the school libraries in all public secondary schools in the state. These libraries should be stocked with current reproductive health materials in print and non-print formats. These materials should be accessible to in-school adolescent girls in order to improve their attitude towards reproductive health practices. Keywords: Information access, Information use, Reproductive health practices, Adolescent girls.
Word count: 489
2 CHAPTER ONE INTRODUCTION
1.1 Background to the Study Adolescents’ sexuality and reproductive health information needs and services have been a major concern and challenge to the international community for over a decade. This is as a result of the growing awareness of young peoples’ relatively high risk of exposure to inaccurate or incomplete information about reproductive health issues such as sex, HIV and other sexually transmitted infections (STIs), pregnancy, abortion, maternal complications, female genital mutilation and so on (World Health Organization, 2002). This is in spite of the generally acknowledged fact that adolescents are a central resource for their countries health and development in the present as well as in the future. Even more important, the United Nations (1989) Convention on the Rights of the Child (CRC) emphasised the need for young people to have access to information and services that will promote their total well being. Articles 17 and 24 of the CRC recognise that young people have a right to information and highest attainable standard of health. In fact, Article 17 stressed that states parties shall ensure that the young people have access to information and materials from a diversity of national and international sources especially those aimed at the promotion of their well being and health. This includes the right to receive information and services necessary to protect themselves from reproductive health related infections, unintended pregnancies and their associated outcomes. Adolescents, according to the World Health Organization (2002), are young people between the age of 10 and19 years, and they constitute about a fifth of the world’s population. Of these, about sixteen per cent live in Africa. In fact, in many countries in Africa, adolescents constitute approximately thirty-three per cent of the population (International Clinical Epidemiology Network, 2006; Olukoya and Ferguson, 2002). In Nigeria, thirty-four per cent of the population are adolescents (Population Reference Bureau, 2006).Adolescence is the transition from the world of childhood to the world of adulthood. It is a period of physical and emotional development almost as rapid as the first decade of life. At this time, the body matures and the mind becomes more questioning and independent (World Health
3 Organization, 2002). The physiological changes which take place during this period of transition from childhood to adulthood result in the formation of sexuality and present the first challenge to healthy adolescent growth. During this period adolescents engage in sexual exploration and experimentation without adequate knowledge of reproductive health issues, information sources and services that are available (International Clinical Epidemiology Network, 2006). According to Olukoya and Ferguson (2002), evidence from World Health Organisation case studies on sexual relations among adolescence in developing countries indicate that sexual activity seems to start during adolescence, and among a significant number of these adolescents much of the activity is often risky, and contraception and condom use is erratic. According to Marie Stopes International Worldwide (2002) the health risks which these adolescents are exposed to include sexually transmitted infections, unplanned pregnancies, unsafe abortions, and untimely death. Adolescent mothers are more likely than older women to suffer from serious complications during delivery, resulting in higher morbidity and mortality for both mother and infants (National Population Commission, 2000). Similarly, health statistics show that more than 13% of all maternal deaths occur among adolescents (ages 10 – 19), representing approximately 69,000 maternal deaths annually. In Africa, maternal mortality among adolescents account for up to 40% in some countries (Olukoya, 2004). A community based study of abortion prevalence among Nigerian women found that one-third of those who obtained abortions were adolescent girls ( Otoide, Oronsaye and Okonofua 2001). A hospital based studies also indicated that up to 80% of patients with abortion-related complications were adolescent girls ( Otoide, et al, 2001). Health reports indicate that more than a third of all people living with HIV/AIDS are under the age of 23, and almost two-thirds of them are female. In Sub-Sahara Africa, among young people aged 15 to 24, two girls are infected for every boy and for adolescents ages 15 to 19, five or six girls are infected for every boy in worst affected areas (UNICEF, 2006). In Nigeria, one of the first cases of AIDS in 1984 was in a sexually active 13 year old girl ( Fawole, Asuzu and Odunta, 1999). Otive-Igbuzor, (2003) stressed that girls within the age-group 12 – 24 are
4 mostly infected with HIV/AIDS. In fact, HIV/AIDS increasingly is becoming a disease of the young girls in Africa. These startling revelations indicate that adolescent girls are more vulnerable to reproductive and sexual health risks than adolescent boys. Reproductive health was defined at the 1994 International Conference on Population and Development (ICPD) as: “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity, in all matters related to the reproductive system and to its functions and processes. Reproductive health therefore implies that people are able to enjoy a satisfying and safe sex life, and that they have the capability to reproduce and the freedom to decide if, when and how often to do so” (Akumadu, 1998:p.35). Important issues affecting adolescent reproductive health are forced and early marriage, premarital sex, early and unwanted pregnancy, unsafe abortion, sexually transmitted diseases/AIDS, female genital mutilation, and so on (Olukoya and Ferguson, 2002, Bodiang, 2000). And a number of studies indicate that adolescent girls are involved in harmful reproductive health practices such as teenage marriage, premarital sex, abortion, female genital mutilation, and so on (Oloko and Omoboye ,1993; Otoide, et al, 2001). At the International Conference on Population and Development (ICPD the Programme of Action specifically backed the right of adolescents to reproductive health care. The conference called for the provision of information and services to adolescents that can help them understand their sexuality and protect them from unwanted pregnancies, sexually transmitted diseases and subsequent risk of infertility. Governmental and non-governmental organisations also were charged with the responsibility of meeting the special needs of adolescents by establishing appropriate programmes to respond to those needs (WHO, 2002; Marie Stopes International Worldwide, 2002). Following the international commitment, the Nigerian Government during the 48th session of the National Council on Education on August 17th, 2001 approved the National Comprehensive Sexuality Education Curriculum for upper primary, secondary schools and tertiary institutions. A non-governmental organisation based in Lagos–Action Health Incorporated, the Nigerian Education Research and Development Council (NERDC) and the Federal Ministry of Education jointly designed this curriculum. It is aimed at providing in-school adolescents appropriate
5 factual information on human sexuality and family life from childhood to adulthood. This appears to be a major step towards breaking the silence associated with sexuality discourse which hitherto promoted ignorance and vulnerability to diseases among this age group (Otive-Igbuzor, 2003). Undoubtedly, access to health information is not only strategic to the achievement of reproductive health; it is the foundation of public health. It is, therefore, imperative that reliable, relevant and timely health information is made available to everyone especially adolescent girls. Godlee, Pakenham-Walsh, Cohen and Paker (2004) proposed that World Health Organisation (WHO) should take the essential lead in championing the goal of “universal access to health care information by 2015” or “Health information for All’ as a prerequisite for meeting the Millennium Development Goals (MDGs) and achieving Health for All. They suggested that strategies for attaining global access to health information should include funding for research into information needs and barrier to use of information; evaluation and replication of successful initiatives; support for local information cycles and communities of practice; and the formulation and establishment of national public policies on health information. Regardless of their geographic, racial, educational and social differences all adolescent girls need access to an array of reproductive health information. Research suggests that there are a number of potential impediments between the recognition of a need to be informed and the activation of a search for information. These are called intervening variables. These include personal barriers, economic barriers, social/interpersonal barriers, and environmental/situational barriers. According to Wilson (1997), the personal variables which can intervene may be either demographic or psychological. These particularly at the level of the person, may act to prevent the initial emergence of a coping strategy, or may intervene between the acquisition of information and its use. Maclnis and Jaworski (1991) proposed that the more knowledgeable the individual, the easier he would find it to encode information thereby making information acquisition and use easier. Among the adolescent girls the most prevalent personal variable that will affect their access and use of reproductive health information are their knowledge base or their level of education. Generally, most of them do not have adequate knowledge of reproductive health and this will make the utilisation of reproductive health information difficult.
6 Information use is defined by Wilson (2000) as the physical and mental acts humans employ to incorporate found information into their knowledge base or knowledge structure. But Dervin (1992) submits that information use is a process condition where the user tries to make sense of discontinuous reality in a series of information use behaviors. Uhegbu (2000) noted that information use varies among individuals and organizations depending on their information needs and socio- economic dictates. Nevertheless, the use of information is dependent upon the context of use just as information need is dependent upon the situation under which it arises. A study of factors affecting users of clinical hospital information systems by Lee and Pow (1996) found that the desire and tendency to use or not to use a particular information channel is affected by the channel’s information access behaviour. They affirmed that if a channel type does not include the access characteristics that the user requires, the user might not use that particular channel type and so might turn to alternative sources of information. The study concluded that information accessibility and delivery affects usage. Therefore, the characteristics of reproductive health information sources will determine their use as well as their effect on the attitude of the information user (adolescent girl). Attitudes are predisposition towards action and can be about or towards people and things. It is evaluative of people, objects and ideas. The Oxford Advanced Learner’s Dictionary (2000) defined attitude as the way an individual thinks and feels about somebody or something; the way one behaves towards somebody or something that shows how one thinks and feels. However, an individual’s attitude towards an object or issue can be deduced from his behaviour in situations involving that object. If a person has negative attitude towards an issue, the expected outcome is unpleasant feeling. It may also be inferred from his disagreement or agreement with statement expressing beliefs and or feelings about that object. A number of studies revealed that access and use of health information could influence adolescents’ attitudes toward reproductive health practices. Odujinrin and Akinkuade (1991) examined adolescents’ knowledge of AIDS, their attitudes, beliefs and preventive measures adopted by them. The study affirmed that accurate information could lead to attitude change and behaviour modification. Out of the 398 in-school adolescents 40.7% changed their life style and behaviours once they
7 heard about AIDS. Most of the adolescents indicated that they refrained from having sexual intercourse with prostitutes. Similarly, Okwilagwe (1993) in his study of bibliotherapeutic influence on sexual attitude of Nigerian female students found that out of the 303 female students 203 (67%) of them indicated that the use to which they have put the knowledge gained from reading books on sex and other related issues have helped them to avoid unwanted pregnancies. Lagos State is one of the 36 states in Nigeria. It was created on 27 t h May, 1967. Until 12 t h December, 1991, when Nigeria’s political capital was relocated to Abuja, Lagos was the nerve centre of the Federal Republic of Nigeria. It is made up of 20 local government areas which were further divided into 57 development areas by Governor Bola Tinubu’s administration. Lagos State, according to 2006 census, has a population of 9.014 million. However, according to 1999 UN study, the city of Lagos is expected to hit the 24.5 million population mark and thus becomes one of the most populous cities in the world by the year 2015. As a cosmopolitan city, the state attracts Nigerians from all ethnic, religious, social and economic backgrounds as well as foreigners (Wikipedia, 2006; National Population Commission, 2006). Studies indicated that adolescents in Lagos State, especially girls enrolled in schools, engage in risky sexual practices. Oloko and Omoboye (1993) in their study of sexual networking among students in Lagos State found that more girls than boys in secondary schools had experienced sex at the age of ten years. About 75% of sexually active in-school adolescent girls and boys had more than two partners. Moreover, ten (4%) of them indicated that they were being treated of sexually transmitted infections. The study conducted on premarital sex among adolescents in Lagos State by Adegbola and Babatola (1999) affirmed early sexual initiation among adolescent girls in the state. This portends great danger for the spread of sexually transmitted diseases since their sexual encounter is largely unplanned and unprotected. This is in spite of the fact that HIV prevalence rate in Lagos State in 1999 was 6.7 per cent, and in 2001 it increased to 7.4% (Federal Ministry of Health, 2001; Ayankogbe, Omotola, Inem, Ahmed, and Manafa, 2003). The state in 2003 had the highest prevalence rate of 4.7% in the South West zone and some local government areas such as Ikeja had 7.7%, Badagry 6.3% and Epe 4.2% prevalence rate (Federal Ministry of Health, 2003). However, in 2005 the HIV prevalence rate
8 in the state dropped from 4.7% to 3.3%, yet a part of Lagos, Lagos Island have a prevalence rate of 9%. And in Lagos State alone, about 600,000 persons are HIV positive (Alaka, 2006). Equally, the study of knowledge, attitudes, beliefs and behavioural practices among secondary school students in Lagos State by Ayankogbe, et al (2003) affirmed that there was little awareness creation about HIV/AIDS among the students. These studies on adolescents’ knowledge, attitude and reproductive practices at secondary school level in Lagos State did not reflect the critical impact of reproductive health information access and utilisation on their attitude to reproductive health practices. Yet, information is the purveyor of knowledge. It is access to relevant information and the application of the learned information, voluntarily or habitually by the receiver that bring about a change in behaviour. Access to information aids meaningful feedback, which helps in the discovery of the actual and potential barriers to the expected positive health behaviours.
1.2 Statement of the Problem Access to appropriate reproductive health information by adolescent girls is crucial to the achievement of the Millennium Development Goals of reducing maternal and child mortality by 2015 and halting and reversing the spread of HIV among the most vulnerable by 2010. Yet, literature has shown that adolescent girls have inadequate access to reproductive health information due to socio-cultural values, religious beliefs, economic factors, inadequate information resources and facilities. Perhaps the adolescent girls’ inadequate access to reproductive health information could have promoted ignorance of basic reproductive health practices and may be responsible for the commonly reported reproductive health problems. In other words, can inadequate access to reproductive health information among teenage girls which promoted gaps in knowledge be linked to unhealthy reproductive health attitudes and practices exhibited by them? However, a literature search revealed that no existing study examined the relationship between reproductive health information access and utilisation with attitude towards reproductive health practices among in-school adolescent girls. It is against this backdrop that this study investigated the relationship between access to and use of health information and in-school adolescent girls’ attitude towards reproductive
9 health practices. 1.3 Objectives of the study The major objective of the study is to examine the extent to which access to and use of health information relates to in-school adolescent girls’ attitude towards reproductive health practices. The specific objectives of the study are to: 1. investigate the state of the school libraries and level of reproductive health materials available in the schools; 2. investigate reproductive health information needs of the in-school adolescent girls in Lagos State; 3. determine the level of the in-school adolescent girls’ access to reproductive health information sources; 4. examine the in-school adolescent girls’ extent of access to reproductive health information; 5. determine the frequency of use of reproductive health information by the in- school adolescent girls; 6. determine the in-school adolescent girls’ attitude towards reproductive health practices; 7. ascertain constraints to access and use of reproductive health information among the in-school adolescent girls; and 8. determine the relationship between access and use of reproductive health information and the in-school adolescent girls’ attitude towards reproductive health practices. 9. investigate if there is any difference in access to and use of reproductive health information among girls in single sex and co-educational schools in Lagos State. 10. investigate the relative effect of access to and use of health information on attitude towards reproductive health practices. 1.4 Research Questions The study has the following research questions: 1. What is the state of the school libraries and the level of reproductive health materials available in the schools? 2. What are the reproductive health information needs of in-school adolescent girls in Lagos State? 3. What is the degree of in-school adolescent girls’ access to reproductive
10 health information sources in Lagos State? 4. To what extent do in-school adolescent girls have access to reproductive health information? 5. What is the frequency of use of reproductive health information by in-school adolescent girls in Lagos State; 6. What is the attitude of the in-school adolescent girls towards reproductive health practices? 7. What are the constraints to access and use of reproductive health information among in-school adolescent girls?
1.5 Hypotheses The study tested the following null hypotheses at 0.05 level of significance:
Ho 1 : There is no significant relationship between in-school adolescent girls’ access to reproductive health information and their attitude towards reproductive health practices.
Ho 2 : Utilization of reproductive health information and in-school adolescent girls’ attitude towards reproductive health practices are not significantly related.
Ho 3 : Access to and use of reproductive health information and their attitude towards reproductive health practices are not significantly related. Ho4: There is no significant difference in access to reproductive health information among girls in all girls’ schools and those in co-educational schools. Ho5: There is no significant difference in the use of reproductive health information among girls in all girls’ schools and those in co-educational schools. Ho6: There is no significant relative effect of access to and use of health information on attitude towards reproductive health practices. 1.6 Scope of the Study Though adolescents are young people between the ages of 10 and 19 years the study focuses on in-school adolescent girls ages 13-20. It is believed that adolescent girls in the senior secondary classes fall mostly within the 13-20 age bracket. The study will cover access to and use of electronic media, print media, oral and institutional sources of health information that are relevant to adolescent girls health needs. The adolescent reproductive health issues that are of interest in this study include teenage marriage, premarital sex, early and unwanted pregnancy, unsafe abortion, sexually transmitted diseases, HIV/AIDS and female genital mutilation. All the 280 senior secondary schools madeup of 23 girls and 257 co-educational public secondary schools in Lagos State were involved in the study.
11 1.7 Significance of the study The findings of this study will help policy makers and stakeholders who are involved in the provision of reproductive health information and services to adolescents to understand the relationship between access to reproductive health information and the attitude of in-school adolescent girls towards reproductive health practices. This will enable them to design and adopt more appropriate policies and intervention strategies that will enhance the general well being of in- school adolescent girls. The result of the study will bring to fore the reproductive health information needs of adolescent girls in Lagos State in particular and elsewhere especially in Nigeria and the Third World. This is expected to provoke government and non-governmental agencies to make concerted effort towards meeting these needs. The outcome of this study may be a basis for reviewing and improving the quality of existing National Health Information Policy, National Health Management Information System and National Sexuality Education Curriculum. Lastly, this study will contribute to knowledge and literature on adolescent reproductive health information which no doubt will be of immense benefit to researchers in the field of adolescent health in Nigeria. 1.8 Definition of Terms Adolescents: Adolescents in this study refer to girls between ages 13 to 20 (the common age bracket for senior secondary schools). Access: Access refers to the degree of proximity, closeness or nearness to sources, and ease of locating and obtaining reproductive health information from the sources. Attitude: Attitude refers to what adolescent girls think about, feel about, and their behaviour towards reproductive health practices Health Information: This includes information for staying well, preventing and managing diseases, and making other decision related to health and health care. It may be in the form of data, text, and/or video. It may involve enhancement through programming and interactivity. Information: This refers to news, facts, messages, opinions, processed data, images that are capable of improving the reproductive health knowledge of in-school adolescent girls. Information Source: The point of origin or a supplier of information; a point of emanation of information; first hand document; primary reference work; an individual; institution or media from where a message originates. Reproductive Health: It refers to a state of complete physical, mental and social well- being and not merely the absence of disease or infirmity, in all matters related to the reproductive system and to its functions and processes. Reproductive Health Information use : the application of reproductive health information; that is how in-school adolescent girls in this study apply reproductive health
12 information received from various sources for decision making, prevention and curative purposes. Reproductive Health practices: It refers to reproductive and sexual health related actions or behaviours such as early marriage, premarital sex, early and unwanted pregnancy, abortion, female genital mutilation.
13 CHAPTER TWO REVIEW OF RELATED LITERATURE
2.0. Introduction This chapter reviews literature relevant to the study. The related literature is reviewed under the following sub-headings: 2.1 Adolescent girls’ reproductive health 2.2 Reproductive health information needs of adolescent girl 2.3 Reproductive health information sources 2.4 Adolescents’ access to reproductive health information 2.5 Adolescents use of reproductive health information 2.6 Constraints to health information access and use 2.7Adolescents’ attitude towards reproductive health practices 2.8 Reproductive health information provision in schools 2.9 Theoretical framework 2.10 Conceptual model of the study 2.11 Appraisal of literature review 2.9 Theoretical Framework There is no single theory that can adequately capture the relationship between the variables under study. However, some theories that are relevant to the study were employed to anchor the study and to guide the analysis and understanding of the linkages between adolescent girls’ attitude to reproductive health practices and their access to and use of information. In his Expectancy-value Theory Raynor (1982) explained that a person adopts a particular attitude position based on the demerits and merits, or perceived value of the goal to be achieved. As rational beings, adolescent girls know what will benefit them and they are able to evaluate and choose between alternatives based on their perceived benefits. Musoke (2000) highlighted the fact that the meaning information made to people after being accessed, used and interpreted and its significance and role as perceived and experienced by the user were the value people attributed to information. The expectancy-value theory therefore explains the fact that access to and use of reproductive health information and benefits derived from its use will result in change in knowledge, values, beliefs, behaviours and attitudes towards reproductive health practices. A general theory in psychology which is helpful in explaining the proximate causes of information behaviour is Dervin’s (1992) sense making theory. The theory
14 states that people seek information when they have identified gaps in their knowledge that prevent them from making sense of a situation in which they find themselves, solve a problem at hand or make an informed decision. Sense-making tasks usually involves seeking for information that are relevant for a purpose and extracting and reformulating relevant information in order to understand a situation. This theory suggests that an adolescent girl at the onset of menarche will most likely seek information about menstruation in order to understand, interpret or make sense of the situation. A teenage girl who suddenly stops menstruating will definitely seek information on possible causes or factors that could be responsible and what steps to take to resolve the situation, (that is restoring menstruation). Another theory relevant to the study is the information richness theory developed by Daft and Lengel. Information richness according to Daft and Lengel (1986) is the ability of information to change understanding within a time interval. The theory states that the richness of a medium is a function of the medium’s capacity for immediate feedback, the number of cues and channels available, language variety and the degree to which intent is focused on the recipient. This theory is an attempt to guide user on how to select the medium that fits their purpose. The in-school adolescent girls are likely to select and utilize information sources and resources that meet their reproductive health needs based on how rich the sources are. The richness of the information sources is dependent on the content relevance of information, authority of information content, recency and timeliness of information delivery. Opeke (1984) argued that the decision to select a certain information source is a perceived evaluation of the probable or expected value of that source. Thus the decision to use certain information sources is influenced both by the attributes of the source in terms of accuracy, expected benefit and the cost of acquiring the source and the nature of the format, form, timeliness and the physical availability of the information source. Therefore, the characteristics of reproductive health information sources will determine their use as well as their effect on the attitude of the information user (adolescent girl). Similarly, the characteristics of the message (reproductive health information), the order of its presentation, the extent of analysis, the use of logic and emotions contribute to the impact on the attitude of the adolescent girl to reproductive health practices Information utilization capacity theory postulated by Curras (1986) is also relevant to the study. This theory indicates that the utilization of information is dependent on the ability of the users to access information. According to Wilson (1999) personal characteristics such as beliefs held by a person, interests, needs or existing attitudes, personal cognitive need (knowledge base) may constitute barriers to access and use of
15 information. Likewise, the environment may impose barriers of an economic, political, geographic or other nature. This implies that the characteristics of the adolescent girls, their level of intelligence, their previous experience, their knowledge of reproductive health could influence their access to and use of reproductive health information.
Education - Formal Schools - Non-formal Literacy classes Association/Meeting n Seminars/Symposia o i t - Informal a Reading books m r Watching films o f Discussions n Intervening variables I
Observations. o t s s e c
A c Intervening variables
t A - Government policies t Communication i Information Attitude t (Information Flow) - Social economic status u - Components Premarital Sex d Premarital Sex - Means - Level of education/ e Teenage knowledge base t Teenage Marriage Interpersonal o
Marriage w Group - Socio-cultural values Family planning Family planning a HIV/STDs Mass media - Environmental variables r - Religious beliefs HIV/STDs d FGM - Methods s FGM Oral r Unsafe abortion etc abortion etc e Written p r Electronic o
d
u
c
t
i
v
e
h
e
a
l
t
h
Use of information - Components - Premarital Sex - Teenage Marriage -Family planning Adapted From NCPFP (1992), and Wilson (1997) -HIV/STDs -FGM, unsafe abortion etc
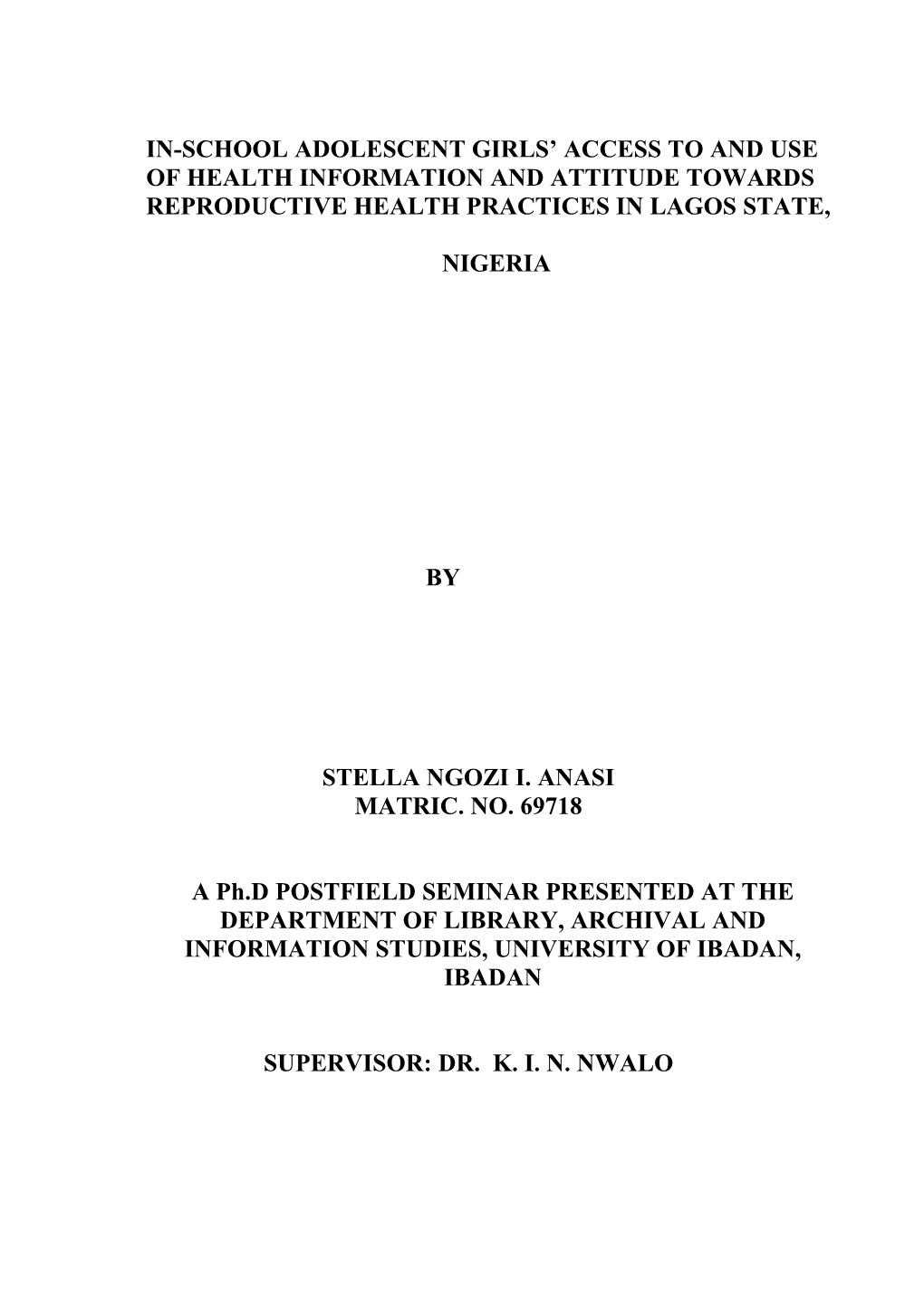
FIG. 1: Conceptual Model of Access to and Use of Information and Attitude towards Reproductive Health Practices
16 2.10 Conceptual Framework The model constructed in Figure 2.1 has been adapted from Information, Education and Communication (IEC) model developed by National Committee for Population and Family Planning (1992), and a revised General Model of Information Behaviour produced by Wilson (1997). The three related components in the Information, Education and Communication model have the major aim of promoting access to information. The information, education and communication model developed by National Committee for Population and Family Planning (1992) is a holistic comprehensive package of all three processes in a coordinated, complementary and strategic fashion that deals with social process by which people are sensitised about their health needs and problems and are influenced towards behavioural changes. The IEC strategies ensure that adolescent girls have access to IEC materials and channels. In the context of this study, the adolescent girls (information user) are expected to use the information acquired or knowledge gained from the IEC resources to equip themselves with negotiation and life skills necessary for making informed decisions. Similarly, the primary role of the three processes of (IEC) health information, health education and health communication is to develop knowledge in order to effect a change in adolescent girls’ health attitudes and habits. A revised general model of information seeking developed by Wilson (1999) fits into this framework. Wilson (1999) suggests that information behaviour comprises of the concepts of information need, intervening variables in the search for information, information acquisition behaviours and information processing and use. The concept of intervening variables indicates that the characteristics of the information source may constitute a barrier to the search for information or to information processing. Such barriers to information search and use, according to Wilson (1999) include personal characteristics; economic barriers; social or interpersonal barriers; and environmental/situational barriers. The intervening variables are barriers to reproductive health information access and use. These include personal characteristics, socio-cultural values, economic variables and environmental variables (Wilson, 1997). The intervening variables determine whether reproductive health information will be accessed and utilised, and also whether there will be a positive or negative change of attitude. The conceptual model in Figure1 proposed linkages and relationship between
17 information access and information use (independent variables) and attitude towards reproductive health practices (dependent variable). Simply put, accessibility and utilisation of reproductive health information could influence attitude to reproductive health practices. In other words, attitude towards reproductive health practices is a function of access to and use of reproductive health information. 2.11 Appraisal of Literature Review The literature reviewed has shown that adolescent girls in developing countries in general and Nigeria in particular have inadequate access to reproductive health information. The identified constraints to access and use of reproductive health information include socio-cultural values, religious beliefs, lack of national health information policy, lack of institutional commitment and political will, economic factors, inadequate information resources and facilities. Several studies carried out at secondary school level in Nigeria in general and Lagos State in particular examined adolescents’ knowledge, attitude and sexual practices. A literature search failed to identify any study that correlates reproductive health information access and utilisation with attitude towards reproductive health practices among in-school adolescent girls. Yet, information is the purveyor of knowledge. It is access to relevant information and the application of the learned information by the recipient that bring about a change in behaviour. It is this gap that this study seeks to bridge.
18 CHAPTER THREE
RESEARCH METHODOLOGY
3.0 Introduction This chapter discusses the research design, population of study, sampling procedure and sample, research instrument, data collection and data analysis. 3.1 Research Design The descriptive survey research design of the correlational type was adopted for the study. The major variables in this study are access to reproductive health information, use of reproductive health information, and attitude to reproductive health practices. 3.2 The Population of Study The target population of this study are girls in SS1-SS3 in public senior secondary schools in Lagos State. There were 23 girls and 257 co-educational public secondary schools making a total of 280 schools in Lagos State. These schools are located within the 20 local government areas in Lagos State which are stratified into six Local Education Districts (LED). Total population of girls in SS1-SS3 in these schools was 127,491 (Lagos State Ministry of Education, 2008).This is shown in Table 3.1. The reason for the selection of adolescent girls in senior secondary schools as participants for this study is based on the fact that these classes are likely to have the age range (13 – 20) defined as adolescents for the purpose of this study. All the 280 guidance counsellors of these schools also formed part of the population for the study. The population of the study is presented in Table 3.1
19 Table3.1: Population of Female Students in Public Secondary Schools in Lagos State District Name of L. G. A. No. of Girls’ No. of co-educational No. of SS1-SS3 female secondary schools secondary schools Students in both schools Agege 2 5 8881 1 Ifako/Ijaiye - 4 3822 Alimosho - 16 11656 Ikorodu - 24 4144 2 Kosofe - 11 8976 Shomolu 2 3 7114 Epe - 24 3341 3 Eti-osa 3 12 4718 Ibeju-Lekki - 9 787 Lagos Island 1 8 2636
Apapa - 6 3703 4 Lagos mainland 3 7 5500 Surulere 7 19 11098 Ajeromi/Ifelodun - 20 8896 5 Amuwo-Odofin 1 17 4992 Badagry - 13 4363 Ojo 1 11 7231 Ikeja - 9 5923 6 Mushin 1 13 8587 Oshodi/Isolo 1 26 11123 Total 20 23 257 127,491 Source: Lagos State Ministry of Education, 2008
3.3 Sample and Sampling technique The multi-stage sampling technique was adopted for this study to achieve a good representation of the population. All the public secondary schools in Lagos State are stratified into 6 Local Education District (LED). First, one local government that has both all girls and coeducational senior secondary schools was randomly selected by balloting from each local education district. Thus any local government area that does not have single gender girls’ schools was not selected. The six local government areas selected are Agege, Shomolu, Eti-osa, Lagos Mainland, Amuwo-Odofin and Mushin. Secondly, two co-educational schools and one all girls’ school was randomly selected by balloting in each of the six randomly selected local government area for the study. Thus a total of 18 schools were selected as indicated in Table 3.2. Thirdly, one intact arm in SS 1, SS 2 and SS 3 was randomly selected by balloting
20 from the schools. The sample size of this study consists of 12 per cent of 14,884 in-school adolescent girls randomly selected from 18 public senior secondary schools in Lagos State, Nigeria. Therefore, a sample of 1800 in-school adolescent girls was used for the study. A representative sample of 1800 out of a population of 14,884 was considered adequate for generalisation based on Krejcie and Morgan (1970) who posited that for a population of 200,000 one could use a sample size of 384. The sample selected for the study is presented in Table 3.2. Table 3.2: Population and Sample Selected for the Study Name of L.G. A. Name of Schools Population of SS1-SS3 Sample Size of students female Students Agege *Girls Senior High School 2258 189 **Dairy farm sec schl 690 61 **Sango Sec. School. 995 72
Shomolu *CMS Girls Grammar School 2 2455 141 **Angus Mem.High Sch l 1552 83 **Gbagada Senior Gram. Schl 2 829 71 *Girls’ Senior Grammar Schl. 632 249 Eti-osa **Kuramo College 359 85 **Falomo High School 285 84
Lagos Mainland *Wesley Girls’Sec. Schl. 1315 227 **Eletu- Odibo High Schl. 294 74 **Fazil Omar High Schl. 227 38 Amuwo-Odofin *Festac Girls Secondary School 425 92 **Agboju Sec School 258 90 **Amuwo-Odofin High Schl. 424 40 Mushin *Ansar-ud-deen Girls High Sch. 985 87 **Ilupeju Grammar Sch. 487 74 **Estate Grammar Schl. 413 43 6 18 14884 1800 * Single sex girls’ schools ** Coeducational schools
3.4 Data Collection Instrument Six types of instruments were used for data collection in this study. They were three questionnaires which were complemented with focus group discussion, observation and interview. The first questionnaire tagged “Reproductive Health Information Needs of Adolescent Girls” had two parts. Part A elicits information on the background of the respondents. These include information on age, class,
21 religion, ethnic group and so on. Part B is on the information needs of the adolescent girls. Eighteen (18) items were presented on a 4 point likert scale with 4,3,2,1 point values attached to them respectively. The second questionnaire tagged “Reproductive Health Information Access and Use” was made up of four parts. Part A elicits information on access to reproductive health information sources. Part B dwells on access to reproductive health information. Eighteen (18) reproductive health information items in likert scale format were presented in this part. Part C has to do with the frequency of utilization of the reproductive health information. Part D elicits information on constraints to access and use of reproductive health information. The third questionnaire tagged “Attitude towards Reproductive Health Practices Scale” contains fourteen (14) items to ascertain in-school adolescent girls’ attitude towards reproductive health practices. The items were presented in 5 point scale with 0, 1, 2, 3, 4 values attached respectively. Focus Group Discussions was also employed to collect data. The focus group discussion held in three schools. These are CMS Girls Grammar School 2, Wesley Girls’ Secondary School and Angus Memorial High School l. The participants for the FGDs were made up of six to seven students selected from SS1, SS2, and SS3. Group discussion is expected to give the participants the opportunity to air their views, opinions, perceptions and reactions on the issues relating to reproductive health information access and use as well as attitude to reproductive health practices. The fifth instrument used was observation. The researcher visited the schools to observe the state of the school libraries and the resources available in the schools which promote access to reproductive health information. The interview was the sixth instrument used for data collection. The interview schedule consists of thirteen questions. The interview was conducted for the guidance counsellors in the schools.
3.5 Validity and Reliability of Instrument The instruments were given to experts at the Library, Archival and Information Studies and Teacher Education departments to ascertain its face and content validity. The research instrument was trial tested at Marywood Grammar School, Ebute-Metta and Eva Adelaja Girls Secondary School using 40 respondents who are
22 in SS 1 – SS 3. These schools were not part of the final sample for the study. Cronbach alpha technique was used to determine the reliability of the instrument. The value of 0.72 for reproductive health information needs of the adolescent girls, 0.71 for reproductive health information access and use and 0.72 for attitude towards reproductive health practices respectively.
3.6 Data Collection Procedure A total number of 1800 copies of questionnaire were administered to the same number of in- school adolescent girls in senior secondary schools in Lagos State as shown in Table 2. The researcher administered with the aid of four trained research assistants the questionnaire on the respondents. The questionnaire was completed in class time under the supervision of the researcher and the research assistants. The advantage of administering the questionnaire in a group situation included greater surveillance to ensure that the subjects’ opinions are truly independent and to avoid non-completion. The reliability of the data collected may be questioned if the students were allowed to complete the questionnaire elsewhere or outside a controlled situation. However, the questionnaire had no identification mark. The focus group discussion held in three schools. These are CMS Girls Grammar School 2, Wesley Girls’ Secondary School and Angus Memorial High School l. The participants for the FGDs were made up of six to seven students selected from SS1, SS2, and SS3. A tape recorder was used for recording the FGD. These started with the researcher speaking on the purpose of the FGDs. This was followed by a very brief self-introduction by every participant after which the discussion began. The researcher and the research assistants solicited for an interview with eleven (11) guidance counsellors as some of the selected schools had no guidance counsellors. Before the interview the objective of the study was made known to the respondents. One-to-one interview was conducted in the schools. While the interview was on the researcher recorded the responses on a tape recorder and also notes were taken. These interviewees are considered active participants in reproductive health issues and are likely to have in-depth knowledge of reproductive health information provision, access and use in their schools and how it has influenced the girls’ attitude to reproductive health practices. They may be regarded as the information gatekeepers in their various schools. The researcher and the research assistants visited the schools and the school
23 libraries to observe the resources and activities in the schools which promote access to reproductive health information. The researcher also wrote down her observations. 3.7 Method of Data Analysis Descriptive statistics such as frequency counts, percentages, mean and standard deviation was used to analyse the research questions. Multiple regression analysis was used to determine the composite effect of access to reproductive health information, use of reproductive health information (independent variables} on attitude (dependent variable} of in-school adolescent girls. Pearson Product Moment correlation coefficient was also employed to test relationship between each of the two variables at 0.05 level of significance . T-test was employed to analyze hypothesis four. Due to the nature of the data, interpretation was both descriptive and analytical. Information from the qualitative data was used to substantiate and corroborate quantitative data.
CHAPTER FOUR DATA ANALYSIS, INTERPRETATION OF RESULTS AND
24 DISCUSSION
4.1 Introduction This chapter presents the findings of data analysed, and the interpretation of the results. The results of the demographic characteristics of respondents and research questions 1-8 were analysed using descriptive statistics of frequency counts and percentages, mean and standard deviation while the hypotheses of the study, which were tested at 0.05 level of significance, were presented using regression analysis. This study investigated the relationship between in-school adolescent girls’ access to and use of reproductive health information and attitude towards reproductive health practices in Lagos State, Nigeria. A total of 1800 students were randomly selected from 18 schools. One single sex girls’ school and two co-educational schools were selected from each of six local education districts. Out of the 1,800 copies of the questionnaire, 1367 were fit for statistical analysis, representing a response rate of 76%. Profile of Senior Secondary Schools Selected for the Study The schools for the study were randomly selected as stated in Table 4.1.
Table 4.1 Profile of Selected Senior Secondary Schools in Lagos State for the Study
25 District Name of L.G. A. Name of Schools Sample Size of students
1 Agege *Girls Senior High School 189 **Dairy farm sec schl 61 **Sango Sec. School. 72 2 Shomolu *CMS Girls Grammar School 2 141 **Angus Mem.High Sch l 83 **Gbagada Senior Grammar Schl 2 71 3 Eti-osa *Girls’ Senior Grammar Schl. 249 **Kuramo College 85 **Falomo High School 84 4 Lagos Mainland *Wesley Girls’Sec. Schl. 227 **Eletu- Odibo High Schl. 74 **Fazil Omar High Schl. 38
5 Amuwo-Odofin *Festac Girls Secondary School 92 **Agboju Sec School 90 **Amuwo-Odofin High Schl. 40 6 Mushin *Ansar-ud-deen Girls High Sch. 87 **Ilupeju Grammar Sch. 74 **Estate Grammar Schl. 43
Total 6 18 1800 * Single sex girls’ schools ** Coeducational schools
4.3 Demographic Characteristics of Respondents.
The background data collected from the respondents revealed that majority of the respondents 564(41.2%) were in SS2, 478 (35.0%) of the respondents in SS1 while 325 (23.5) of the respondents were in SS 3. A breakdown shows that of 941 (68.8%) of the respondents were within the age range of 15-17 years; 272 (19.9%) were within the age range of 13-14 years while 154) (11.3%) were within the age range of 18-21 years. The survey also showed that majority of the respondents 884(64.7) were Christians, 474 (34.7) were Muslims, 7 (0.5%) were traditionalists while 2 (0.1%) belong to other religion. As regards ethnic group, 894 (65.4%) of the respondents were Yorubas, 309 (22.6%) were Igbos, 32 (2.3%) were Hausas while 132 (9.7%) belong to other ethnic groups. The result indicates that 392 (28.7%)of the respondents belong to Science Club,121(8.9%) were members of HIV/AIDS club, 233 (17.0%) were members of Debating Society, 115 (8.4%) belong to Sports Club,81 (5.9%) belong to Red Cross Society, 15 (1.1%) were members of
26 Historical Society while 330( 24.1%) belong to other Clubs such as Health and Life Planning Club, Princess Club and so on. 4.4 Presentation of Result on the Research Questions. 4.4.1 Research Question 1 What is the state of the school libraries and level of reproductive health materials available in the schools? Table 4.2 reveals the state of the libraries and the level of reproductive health materials available in the schools surveyed. From observation, only two out of the 18 schools had a place that could be referred to as a library. Many were mere empty reading space than a library considering the types of books and the volumes in stock. The two school libraries were fairly spacious, well furnished but had inadequate and outdated learning resources. The library at Ansar-Ud-deen Girls High School was furnished through Education Trust Fund in 2003. However, at Festac Girls Secondary School, there was an attempt at developing an e-library. The library was equipped with one computer, one television, a video player and diskettes. The poor state of the libraries in Lagos public secondary schools implies that Lagos State Government is not committed to the development of school libraries as entrenched in the National Policy on Education, 1981. None of the libraries visited had a qualified school librarian. In all the schools visited the level of available reproductive health materials was very poor. Only a few copies of biology, and integrated science textbooks with relevant information on reproduction were available. A few posters and stickers that convey reproductive health information were pasted around some of the schools. Details of the findings are presented in Table 4.2.
Table: 4.2: The State of the School Libraries and Level of Reproductive Health Materials Available in the Schools
27 Name of Schools Location State of the library Level of reproductive health materials. Girls Senior High School Agege A reading room with few dusty old books Very poor on the shelves Dairy farm sec schl Agege A fairly spacious library with no furniture, Very poor very few dusty old books Sango Sec. School. Agege No library due to reconstruction None CMS Girls Grammar School 2 Bariga Very few books, the library serves as both Very poor reading room and staff room Angus Mem.High Sch l Shomolu No library Very poor Gbagada Senior Grammar Schl 2 Gbagada No library None Girls’ Senior Grammar Schl. Obalende A reading room with a few dusty old books Very poor on the shelves Kuramo College Victoria A fairly spacious library with no furniture, Very poor Island very few books
Falomo High School Falomo No library None Wesley Girls’Sec. Schl. Sabo No library None Eletu- Odibo High Schl. Abule Oja No library due to reconstruction None Fazil Omar High Schl. Onike No library due to reconstruction None Festac Girls Secondary School Festac Town A fairly spacious reading Very poor room, with one computer, one television, one video player, discs
Agboju Sec School Agboju A fairy stocked library, well arranged with Very poor good furniture Amuwo-Odofin High Schl. Mile 2 No library None Ansar-ud-deen Girls High Sch. Mushin A fairly spacious library with furniture, Very poor many dusty and outdated books Ilupeju Grammar Sch. Oshodi A reading room with a few books Very poor Estate Grammar Schl. Oshodi A reading room / staff room with a few Very poor dusty old books .
4.4.2 Research Question 2 What are the reproductive health information needs of in-school adolescent girls in Lagos State? The results of the reproductive health information needs of the respondents are presented in Table 4.3. The means score computed indicates that the in-school adolescent girls’ most important reproductive health information need is how to
maintain healthy friendship with men without sex ( X = 3.22). This was closely followed by information on how to avoid HIV/AIDS and other sexually transmitted
infections ( X =3.04), how to control sexual desire ( X =3.02), where to go for HIV test ( X =2.92), how to identify signs of HIV/ AIDS ( X =2.89), how to avoid premarital sex ( X =2.86), and how to identify signs of sexually transmitted infections ( X =2.83). Others are information on how to refuse teenage marriage ( X =2.72), health effects of female circumcision ( X =2.55), and different methods of
28 pregnancy prevention ( X = 2.50). The reproductive health information that in- school adolescent girls least desired were information on how to terminate
pregnancy safely ( X =1.90) and where to buy condom ( X =1.66). The overall mean of 2.59 indicates that in-school adolescent girls greatly desired reproductive health information. The results of their responses are shown in Table 4.3. Table: 4.3 The Reproductive Health Information Needs of the Respondents Information needs Very Greatly Occasionally Not at all No Mean greatly needed needed response needed HIV/STDs Freq % Freq % Freq % Freq % Freq % prevention/management How to maintain healthy 759 58.2 268 19.6 140 10.2 137 10.0 27 2.0 3.22 friendship with men without sex. How to avoid HIV/AIDS 704 51.5 297 21.7 136 9.9 178 13.0 52 3.8 3.04 and other sexually transmitted infections. How to control sexual 673 49.2 324 23.7 146 10.7 179 13.1 45 3.3 3.02 desire. Where to go for HIV test 630 46.1 290 21.2 195 14.3 218 15.9 34 2.5 2.92 How to identify signs of 629 46.0 303 22.2 156 11.4 211 15.4 68 5.0 2.89 HIV/AIDS. How to avoid premarital 658 48.1 252 18.4 135 9.9 256 18.7 66 4.8 2.86 sex How to identify signs of 573 41.9 329 24.1 193 14.1 208 15.2 64 4.7 2.83 sexually transmitted infections Health consequences of 554 40..5 294 21.5 152 11.1 279 20.4 88 6.4 2.69 STDs/AIDS. Negative effects of 402 29.4 273 20.0 213 15.6 366 26.8 113 8.3 2.35 casual sex Correct use of condom 341 24.9 148 10.8 171 12.5 671 49.1 36 2.6 2.06 Where to buy condoms 170 12.4 133 9.7 196 14.3 794 58.1 74 5.4 1.66 Teenage marriage How to refuse teenage 568 41.6 274 20.0 186 13.6 254 18.6 85 6.2 2.72 marriage Health effects of teenage 463 33.9 273 20.0 218 15.9 348 25.5 65 4.8 2.53 marriage Genital mutilation Health effects of female 502 36.7 262 19.2 190 13.9 310 22.7 103 7.5 2.55 circumcision. Family planning Different methods of 509 37.2 211 15.4 161 11.8 433 31.7 53 3.9 2.50 pregnancy prevention How to use different 366 26.8 255 18.7 195 14.3 442 32.3 109 8.0 2.24 methods of pregnancy prevention Unsafe Abortion prevention Health consequences of 341 24.9 226 16.5 217 15.9 516 37.7 67 4.9 2.19 unsafe abortion How to terminate 271 19.8 159 11.6 152 11.1 732 53.5 53 3.9 1.90 pregnancy safely
29 4.4.3 Research Question 3 What is the degree of in-school adolescent girls’ access to reproductive health information sources in Lagos State? The study sought from respondents their degree of access to reproductive health information sources. The mean scores in Table 4.4 revealed that very easily
accessible sources of reproductive health information were parents ( X =3.45), textbooks ( X =3.36), television ( X =3.31), siblings ( X =3.19), music and songs ( X =3.10) drama ( X =3.09) radio ( X =3.08), friends ( X =3.06), and school teachers ( X =3.05) in that order of importance. The result indicates that interpersonal means of communication and mass media were the sources through which the respondents access reproductive health information. The last four least sources of reproductive
health information were librarians and libraries ( X =2.14), leaflets ( X =2.11), non- governmental agencies ( X = 1.93) and the Internet ( X =1.87). The over all mean of 2.73 reveals that most reproductive health information sources were easily accessible to the in-school adolescent girls. The finding is presented in Table 4.4.
Table 4.4: Access to Reproductive Health Information Sources by the Respondents
Information Sources Very easily Easily Accessible Not No Response Mean
30 accessible accessible accessible Freq % Freq % Freq % Freq % Freq % Parents 971 71.0 152 11.1 154 11.3 66 4.8 24 1.8 3.45 Textbooks 842 60.3 283 20.7 201 14.7 45 3.3 14 1.0 3.36 Television 817 59.8 264 19.3 197 14.4 64 4.7 25 1.8 3.31 Brothers/sisters(siblings) 815 59.6 214 15.7 188 13.8 76 5.6 74 5.4 3.19 Music/Songs 691 50.5 291 21.3 249 18.2 106 7.8 30 2.2 3.10 Drama 700 51.2 263 19.2 267 19.5 101 7.4 36 2.6 3.09 Radio 667 48.8 300 21.9 267 19.5 109 8.0 24 1.8 3.08 Friends 633 46.3 332 24.3 270 19.8 110 8.0 22 1.6 3.06 School teachers 636 46.5 322 23.6 280 20.5 97 7.1 32 2.3 3.05 Other family members 617 45.1 306 22.4 270 19.8 106 7.8 68 5.0 2.95 (cousins, uncles, aunts, etc.) Religious 595 43.5 302 22.1 284 20.8 139 10.2 47 3.4 2.92 leaders/institutions Newspapers 535 39.1 340 24.9 327 23.9 148 10.8 17 1.2 2.90 Magazines 515 37.7 343 25.1 303 22.2 176 12.9 30 2.2 2.83 Neighbours 492 36.0 369 27.0 326 23.8 142 10.4 38 2.8 2.83 Novels 612 44.8 228 16.7 207 15.1 268 19.6 52 3.8 2.79 Health workers /Health 486 35.6 334 24.4 313 22.9 184 13.5 50 3.7 2.75 centres Films/Home videos 433 31.7 332 24.3 307 22.5 248 18.1 47 3.4 2.63 Posters 325 23.8 268 19.6 385 28.2 335 24.5 54 4.0 2.35 Symposium/Talks 312 22.8 276 20.2 382 27.9 310 22.7 87 6.4 2.30 Pamphlets 287 21.0 308 22.5 328 24.0 322 23.6 122 8.9 2.23 Billboards 263 19.2 281 20.6 374 27.4 391 28.6 58 4.2 2.22 Libraries/Librarians 277 20.3 253 18.5 267 19.5 521 38.1 49 3.6 2.14 Leaflets 231 16.9 260 19.0 392 28.7 402 29.4 82 6.0 2.11 Non-governmental 228 16.7 213 15.6 339 24.8 414 30.3 173 12.7 1.93 organizations Internet 168 12.3 211 15.4 295 21.6 656 48.0 37 2.7 1.87
4.4.4 Research Question 4 To what extent do in-school adolescent girls have access to reproductive health information? The respondents were asked to indicate their degree of access to different reproductive health information items. From the mean scores in Table 4.5, the most prevailing reproductive health information items that the in-school adolescent girls had access to were in the following order: how to maintain healthy friendship with
men without sex ( X =2.76), how to avoid HIV/AIDS and other sexually transmitted infections ( X =2.60), Where to buy condoms ( X =2.55), how to avoid premarital sex ( X =2.51), and how to identify signs of HIV/AIDS ( X =2.47). However, the in-
31 school adolescent girls had less access to information on how to identify sexually
transmitted infections ( X =2.43), health consequences of HIV/AIDS ( X =2.41), how to control sexual desire ( X =2.32) different methods of pregnancy prevention ( X =2.25), how to refuse teenage marriage ( X =2.22) and negative effects casual sex ( X =2.19). On the whole, the overall mean of 2.23 is low and indicates that the in- school adolescent girls have limited access to reproductive health information. The results are presented in Table 4.5.
Table 4.5: Access to Reproductive Health Information by the Respondents
Information on Very Easily Accessible Not No Response Mean easily accessible accessible accessible HIV/STDs Freq % Freq % freq % Freq % Freq % prevention/management How to maintain healthy 586 42.9 235 17.2 254 18.6 218 15.9 74 5.4 2.76 friendship with men without sex. How to avoid HIV/AIDS 532 38.3 247 18.1 230 16.8 260 19.0 107 7.8 2.60 and other sexually transmitted infections. Where to buy condoms 509 37.2 226 16.5 241 17.6 289 21.1 102 7.5 2.55 How to avoid premarital 485 35.5 230 16.8 242 17.7 315 23.0 95 6.9 2.51 sex How to identify signs of 459 33.6 229 16.8 256 18.7 345 25.2 78 5.7 2.47
32 HIV/AIDS. How to identify signs of 410 30.0 286 20.9 247 18.1 328 24.0 96 7.0 2.43 sexually transmitted infections Health consequences of 404 29.6 272 19.9 268 19.6 329 24.1 94 6.9 2.41 STDs/AIDS. How to control sexual 368 26.9 276 20.2 235 17.2 397 29.0 91 6.7 2.32 desire Negative effects of casual 327 23.9 245 17.9 259 18.9 428 31.3 108 7.9 2.19 sex Where to go for HIV test 290 15.3 140 10.2 178 13.0 741 54.2 99 7.2 1.72 Correct use of condom 260 19.0 146 10.7 186 13.8 692 50.6 80 5.9 1.86 Family planning Different methods of 393 28.7 213 15.6 217 15.9 435 31.8 109 8.0 2.25 pregnancy prevention How to use different 340 24.9 238 17.4 229 16.8 478 35.0 82 6.0 2.20 methods of pregnancy prevention Teenage marriage How to refuse teenage 397 29.0 178 13.0 225 16.5 464 33.9 103 7.5 2.22 marriage Health effects of teenage 279 20.4 232 17.0 267 19.5 490 35.8 99 7.2 2.07 marriage Genital mutilation Health effects of female 326 23.8 210 15.4 250 18.3 454 33.2 127 9.3 2.11 circumcision Unsafe Abortion prevention Health consequences of 237 17,3 189 13.8 237 17.3 597 43.7 107 7.8 1.89 unsafe abortion How to terminate 196 14.3 158 11.6 178 13.0 758 55.4 77 5.6 1.74 pregnancy safely .
4.4.5 Research Question 5 What is the frequency of use of reproductive health information by in-school adolescent girls? Respondents were asked to indicate whether or not they have ever used reproductive health information. In all, 786(57.5%) answered in the affirmative while 581 (42.5%) had never used reproductive health information. Another question was asked to find out how frequently they use various reproductive health information, the mean value in Table 4.6 shows that information on where to buy
condom ( X =2.75), correct use of condom ( X =2.70), and how to terminate pregnancy safely ( X =2.51), were the most frequently used. While information on how to discourage female circumcision ( X =1.99), how to maintain healthy
33 friendship with men without sex ( X =1.93) and how to avoid HIV and other sexually transmitted infections ( X = 1.76) were the least used information items. The overall mean of 2.19 is low and shows that most of the reproductive health information items are used annually by the in-school adolescent girls in Lagos State. The finding is presented in Table 4.6.
Table 4.6: Respondents’ use of Reproductive Health Information
Information on Daily Weekly Monthly Quarterly Annually Never Mean
HIV/STDs prevention Freq/% Freq/% Freq/% Freq/% Freq/% Freq/% /management Where to buy condom 503 (36.8) 64 (4.7) 34 (2.5) 46(3.4) 31(2.3) 85(6.2) 2.75 Correct use of condom 485 (35.5) 55 (4.0) 36 (2.6) 64(4.7) 37(2.7) 92(6.7) 2.70 Where to go for HIV 248 82 66 110(8.0) 93 140 2.06 test (18.1) (6.0) (4.8) (6.8) (10.2) How to identify signs 233 83 62 106(7.8) 85 199 2.01 of HIV/AIDS (17.0) (6.1) (4.5) (6.2) (14.6) How to identify signs 222 90 61 102 (7.5) 104 189 2.00 of sexually transmitted (16.2) (6.6) (4.5) (7.6) (13.8) infections How to maintain 209 109 62 63 68 267 1.93 healthy friendship with (15.3) (8.0) (4.5) (4.6) (5.0) (19.5) men without sex.
34 How to avoid HIV and 170 81 62 93 76 297 1.76 other sexually (12.4) (5.9) (4.5) (6.8) (5.6) (19.5) transmitted infections. Unsafe Abortion prevention How to terminate 406 68 48 81 64 95 2.51 pregnancy safely (29.7) (5.0) (3.5) (5.9) (4.7) (6.9) Family planning How to use 369 61 51 78 67 92 2.33 contraceptives (27.0) (4.5) (3.7) (5.7) (4.9) (6.7) Different methods of 331 75 37 120 68 146 2.31 pregnancy prevention (24.2) (5.5) (2.7) (8.8) (5.0) (10.7) Genital mutilation How to discourage 230 90 75 96 64 179 1.99 female circumcision (16.8) (6.6) (5.5) (7.0) (4.7) (13.1) Teenage marriage Right time for a girl to 171 167 74 82 56 218 2.00 marry (12.5) (12.2) (5.4) (6.0) (4.1) (15.9) Note: (Figures in parenthesis are in percentages)
4.4.6 Research Question 6 What is the attitude of in-school adolescent girls towards reproductive health practices? To determine the attitudes of in-school adolescent girls towards reproductive health practices, they were given 14 items on attitude to which they were asked to agree or disagree. Their attitude was measured on a 5-point Likert scale by asking them to score each statement as follows: undecided, = 0, strongly Disagree = 1, Disagree = 2, Agree = 3, strongly agree = 4. The mean scores of each item on Table 4.7 revealed that the respondents had positive attitude towards reproductive health practices. A look at item 3 on Table 4.7 reveals a mean score of 3.08 which is agreement on the scale. This implies that the response to the item is significant and the attitude is positive. Similarly, positive attitudes to reproductive health practices were recorded on items like “it is
good to resist pressures of premarital sex”( X =2.63;SD= 1.41); “I hate the idea of having sex with many men/boys” ( X =2.87; SD=1.31); “I feel the idea of terminating an unplanned pregnancy is not good at all ( X =2.70; SD=1.36); “I hate female circumcision because it is dangerous ( X =2.63; SD=1.35). One can therefore conclude that the respondents were favourably disposed to reproductive health practices. The analysis of the data on the attitude of the respondents is presented in Table 4.7. Table 4.7: A summary of Responses of in-school Adolescent Girls’ to items on attitudes
35 towards Reproductive Health Practices Information on Mean SD Decision
Family planning I think girls who engage in casual sex should use 2.56 1.33 Agree contraceptives I believe girls should have casual sex without 1.52 1.06 Disagree contraceptives. HIV/STDs prevention/management I feel abstinence is best for young girls until 3.08 1.24 Agree marriage It is good to resist pressures of premarital sex. 2.63 1.35 Agree I hate the idea of having sex with many men/boys 2.87 1.31 Agree I will like to take HIV/AIDS test. 2.56 1.33 Agree I feel premarital HIV/AIDS test should be 2.63 1.35 Agree compulsory. I will like to have casual sex without condom. 1.46 1.07 Disagree Teenage marriage I believe girls should marry before they are 1.44 0.93 Disagree 18years. In my opinion girls should not marry until they 2.56 1.33 Agree are at least 18 years. Unsafe Abortion prevention I feel the idea of terminating an unplanned 2.70 1.36 Agree pregnancy is not good at all. I believe a girl should terminate an unplanned 1.49 1.03 Disagree pregnancy anywhere she likes. Genital mutilation I hate female circumcision because it is 2.63 1.35 Agree dangerous. I feel female circumcision should be encouraged. 1.94 1.32 Disagree
4.4.7 Research Question 7 What are the constraints to access to and use of reproductive health information among in-school adolescent girls? From the findings, the factors which hinder the respondents from accessing reproductive health information were: lack of time to seek relevant information 855 (62.5%), unwillingness of my parents to discuss reproductive health issues with me as an adolescent 825 (60.4%), lack of awareness about sources of reproductive health information 798 (58.4%), reproductive health information is not easy to obtain 744 (54.4%), poverty and low socio-economic status 729 (53.3%), unwillingness of my teachers to discuss reproductive health issues with me as an adolescent 723 (52.9%) and reproductive health information resources sand facilities are not available 722 (52.8%). Others followed as presented in Table 4.8.
36 Table: 4.8 Constraints to Respondents’ Access to Reproductive Health Information Constraints to Access Yes No No of % No of % Respondent Respondent Lack of time to seek relevant reproductive health 855 65.5 512 37.5 information Unwillingness of my parents to discuss 825 60.4 542 39.6 reproductive health issues with me as an adolescent Lack of awareness about sources of reproductive 798 58.4 569 41.6 health information Reproductive health information is not easy to 744 54.4 623 45.6 obtain Poverty and low socio-economic status 729 53.3 638 46.7 Unwillingness of my teachers to discuss 723 52.9 644 47.1 reproductive health issues with me as an adolescents Reproductive health information resources and 722 52.8 645 47.2 facilities are not available Lack of school library 631 46.2 736 53.8 Radio/T.V/Newspapers are not readily available 631 46.2 736 53.8 to me Materials on reproductive health are very 603 44.1 764 55.9 expensive I am not interested/ I don’t think I need it 579 42.4 788 57.6
Table 4.9 shows that among the constraints to the use of reproductive health information, 898 (65.7%) of the respondents indicated inability to get reliable and accurate information, followed by fear of embarrassment in the event of using the information 877 (64.2%), in adequate knowledge of reproductive health 835 (61.1%), negative attitudes of health care providers 756 (55.3%), religious beliefs and retrogressive cultural values 651 (47.6%). The least constraints to the use of reproductive health information were that reproductive health terms are difficult to understand 618 (45.2%) and that reproductive health practices are only for married people 545 (39.9%). Table 4.9: Constraints to Respondents’ Use of Reproductive Health Information Constraints to Use Yes No Freq % Freq % Inability to get reliable and accurate information. 898 65.7 469 34.3 Fear of embarrassment in the event of using the 877 64.2 490 35.8 information Inadequate knowledge of reproductive health 835 61.1 532 38.9 Negative attitude of health care providers 756 55.3 611 47.1 Religious beliefs/Retrogressive cultural values 651 47.6 716 52.4 Reproductive health terms are difficult to understand 618 45.2 749 54.8 Reproductive health practices are only for married people 545 39.9 822 60.1
37 4.5 Test of Hypotheses
Five hypotheses were formulated and tested at 0.05 level of significance. 4.7.1: Hypothesis 1
Ho 1 : There is no significant relationship between in-school adolescent girls’ access to reproductive health information and their attitude towards reproductive health practices. The result of the relationship between in-school adolescent girls’ access to reproductive health information and their attitude towards reproductive health practices is presented in Table 4.10. Table: 4.10: Correlation between Access to Reproductive Health Information and Attitude towards Reproductive Health Practices
Parameter Value Pearson Correlation coefficient (r) 0.107 N 1367 P value .000 α =0.05
Table 4.10 shows that the Pearson Correlation Coefficient (r) indicating the relationship between in-school adolescent girls’ access to reproductive health information and their attitude towards reproductive health practices is 0.107; P< 0.05. Since the P value is less than 0.05 level of significance, then the null hypothesis one was therefore rejected. This means that there is significant relationship between in-school adolescent girls’ access to reproductive health information and attitude towards reproductive health practices. 4.5.2: Hypothesis 2
Ho 2 : Utilization of reproductive health information and in-school adolescent girls’ attitude towards reproductive health practices are not significantly related. Result of correlation analysis to test this hypothesis is presented in Table 4.13. Table 4.11: Correlation between Use of Reproductive Health Information and Attitude towards Reproductive Health Practices Parameter Value Pearson Correlation coefficient (r) - .009 N 1367 P value .739
α =0.05
38 Table 4.11 shows the Pearson Correlation Coefficient (r ) indicating the relationship between in-school adolescent girls’ use of reproductive health information and attitude towards reproductive health practices is -.009; P value > 0.05. Since the P value is greater than 0.05 level of significance, then the null hypothesis two was therefore not rejected. Hence utilization of reproductive health information and in-school adolescent girls’ attitude towards reproductive health practices are not significantly related. 4.5.3 Hypothesis 3
Ho 3 : Access to and use of reproductive health information and in-school adolescent girls’ attitude towards reproductive health practices are not significantly related. Summary of the regression analysis is presented in Table 4.12. Table: 4.12 Regression Summary among Access, Use and Attitude
R = .108 R square = .012 Adjusted R square = .010 Std. Error of Estimate = 7.27887 Source of Sum of Df Mean F-Ratio Sig. of P variation Squares Square Regression 850.378 2 425.189 8.025 .000 Residual 72267.337 1364 52.982 Total 73117.715 1366
Table 4.12 shows that the multiple regression correlation coefficient (R) indicating the linear relationship among access to, use of reproductive health information and attitude towards reproductive health practices is .108; R square equals 0.012 while the adjusted R square equals 0.010. This implies that the two independent variables (Access and Use) contributed only 1 per cent to the variation in-school adolescent girls’ attitude to reproductive health practices. The remaining unexplained 99 per cent could be due to other factors that were not considered in this study. Further verification, using Regression ANOVA produced F ( 2, 1 36 4 ) ratio equals 8.025; P < 0.05. Since P value is less than 0.05 then the null hypothesis three was therefore rejected. Hence there is significant linear relationship among access to, use of reproductive health information and attitude towards reproductive health practices.
39 4.5.4: Hypothesis 4 Ho4: There is no significant difference in access to reproductive health information among girls in all girls’ schools and those in co-educational schools. Details of the analysis are shown in Table 4.13. Table 4.13 T-test Comparison of Access to Reproductive Health Information between Single sex and Co-educational Schools N Mean SD Df Tobs. Pvalue Decision Single Sex 739 41.10 14.73 1365 1.256 .209 NS
Coeducational 628 40.11 14.25 NS= Not Significant at 0.05 alpha level
Table 4.13 shows that the mean scores of the two groups are almost alike, differing by only1.01points. In addition, the t (1365) observed indicating the difference in access to reproductive health information between girls in single sex and those in coeducational school is 1.256; P>0.05. Since the P value is greater than 0.05 alpha level, then the null hypothesis 4 is therefore not rejected. This implies that there is no significant difference in access to reproductive health information among girls in single sex and co-educational schools. 4.5.5 Hypothesis 5 Ho5: There is no significant difference in use of reproductive health information among girls in all girls’ schools and those in co-educational schools. Result of the analysis is presented in Table 4.14. Table 4.14 T-test Comparison of Use of Reproductive Health Information between Single sex and Co-educational Schools N Mean SD Df Tobs. Pvalue Decision Single Sex 739 2.21 2.44 1365 -.496 .620 NS
Coeducational 628 2.28 2.48 NS= Not Significant at 0.05 alpha level
Table 4.14 shows that the mean values of the two groups are almost the same, differing by only 0.07 points. The t (1365) observed indicating the difference in use of reproductive health information between girls in single sex and those in coeducational school is –.496; P>0.05. Since the P value is greater than 0.05 alpha level, then the null hypothesis 5 is therefore not rejected. This means that there is
40 no significant difference in use of reproductive health information among girls in single sex and co-educational schools. 4.5.6 Hypothesis 6 To ascertain the relative contribution of each independent variable to predict in-school adolescent girls’ attitude towards reproductive health practices in Lagos State, Nigeria, all the independent variables investigated in this study were entered into a regression analysis. The result is presented in Table 4.15. Table 4.15: Coefficients indicating Relative Effects of Access to and Use of Reproductive health information on Attitude towards Reproductive health Practices Variable Unstandardized Standardized T Sig Decision Coefficients coefficients B Std. Error Beta (Constant) 28.839 .603 47.830 .000 Access to .054 .014 .108 3.992 .000 S information Use of -.048 .080 -.016 -.597 .550 NS information
According to Table 4.15 the Beta of access to reproductive health information to the prediction of attitude towards reproductive health practices is ( β =.108). This implies that access to reproductive health information contributed 10 per cent to the prediction of attitude towards reproductive health practices of in-school adolescent girls. Similarly, the Beta of use of reproductive health information to the prediction of attitude towards reproductive health practices is ( β = -.016). This means that use of reproductive health information contributed 2 per cent to the prediction of attitude towards reproductive health practices. Table 4.16 reveals that use of reproductive health information is not a significant predictor of in-school adolescent girls positive attitude towards reproductive health practices ( B = -.048; t = -.597; P > 0.05), but access to reproductive health information has a significant relative effect on attitude towards reproductive health practices ( B= .054; t = 3.992; P < 0.05) and statistically significant.
4.6: Discussion 4.6.1 Demographic Characteristics of the Respondents Majority of the respondents are in SS2 class and also in their middle adolescence (ages 15-17). At this age the girls in many countries are undergoing
41 rapid sexual and reproductive transitions, as well as changes in other aspects of their lives (Lloyd, 2005, cited in Dixon-Mueller, 2008). Although labeled “children” by the Convention on the Rights of the Child, 15-17 year olds are not considered children in other international agreements, for example, the 1973 Minimum Age Convention of the International Labor Office. At this age and their level of schooling many of them are experiencing pressures from the opposite sex for premarital sex which can result in unwanted pregnancy that leads to school drop out. In some cultures, middle adolescence is also a period when girls experience intense pressure from their parents to enter an arranged marriage (Dixon-Mueller, 2008). All these make access to and use of comprehensive sexuality information by in-school adolescent girls imperative. The respondents represent adolescents from different ethnic and religious groups in Nigeria. This makes generalization of the findings possible. 4.6.2 State of the school libraries and level of reproductive health materials available in the schools The finding of the study on the state of the school libraries and level of reproductive health materials available in the schools revealed that most of the schools have no functional libraries. Where libraries exist at all, they are in a deplorable state and the level of reproductive health materials is very poor. All the participants at the Focus Group Discussion maintained that they do not have functional libraries and therefore rarely have access to reproductive health materials through the libraries. Again, the guidance counselors maintained that most of the schools have no functional school library and that the libraries are not providing adequate reproductive health materials. Therefore in most cases the students make decisions not based on adequate and accurate information on reproductive health issues. This supports the findings of Okiy (2004) that most schools in Nigeria lack libraries and the few that are available are poorly funded, lack adequate collections and accommodation. The finding is consistent with the observation of Hart (2000) that the materials in the libraries in Swaziland were outdated and not useful and the libraries as agents of social change and information providers were not participating actively in the dissemination of reproductive health information to the communities. The result is also similar to what was found by Ayankogbe, et al (2003) that only 4.5% of students got HIV information from their schools. They reported that this is rampant all over Africa and a perennial problem
42 in Nigerian schools in general and Lagos schools in particular. In Uganda, Batambuze (2003) also reported that school libraries are lagging behind in the provision of HIV/AIDS information. Yet, Alegbeleye (1981) averred that libraries are the means not only of obtaining access to required information but also of giving the user independent access to all kinds of ideas and information. 4.6.3 Reproductive Health Information Needs The major reproductive health information needs of the respondents were information on how to maintain healthy friendship with men without sex, how to avoid HIV/AIDS and other sexually transmitted infection, how to control sexual desire, where to go for HIV test, how to identify signs of HIV/AIDS and sexually transmitted infections, how to refuse teenage marriage , health effects of female circumcision and information on different methods of pregnancy prevention. The finding here is to be expected as the respondents seem to be aware of the fact that unwanted pregnancy, HIV acquisition or early marriage can disrupt their school career (Grant and Hallman, 2008; Juarez, LeGrand, Lloyd, and Signh, 2008). HIV/STDs Prevention and Management In this study the in-school adolescent girls greatly desired information on the prevention and management of HIV and sexually transmitted diseases. Opeke (2004) corroborated this by making assertion that with the growth of the HIV/AIDS epidemic, the hunger for HIV/AIDS information has increased. Similarly, the respondents’ desire for information on how to avoid HIV/AIDS and other sexually transmitted infections and how to avoid premarital sex is in line with the findings of other studies on information needs of different user groups as reported by Mabawonku (1998) who in her study revealed that the respondents expressed that they need information on how to protect themselves from contacting HIV/AIDS. The participant at the Focus Group discussion indicated that they need reproductive health information to guide their actions and decisions. A Focus Group participant at CMS Girls Grammar School 2 stated that: “We need reproductive health information so that we know the right things to do at the right time for now I know that what I should do is to focus on my studies. No boy friend, no sexual intercourse and all that”
Opeke (2004) maintained that information has the role of educating, mobilizing and sensitizing them about issues contained in HIV/AIDS for effective and constructive participation in the process of its eradication. The in-school adolescent girls’ least
43 desired reproductive health information is information on where to buy condom. The fact that condom is conspicuously displayed and sold everywhere in the chemist shops may have contributed to their response. This is consistent with the results of the study conducted by Otoide, et al (2001) which revealed that young people generally felt that the services offered by patent medicine dealers were sufficient to meet their contraceptive needs as these dealers are located on street corners. Teenage Marriage According to Dixon Muller (2008) adolescence is a time when girls in some cultures experience intense pressure from their families to enter an arranged marriage. They therefore need legal and social support to either refuse to marry or to participate fully in the choice of partner, the timing of marriage, and the terms of exchange. In-school adolescent girls need information on health effects of teenage marriage and skills to resist pressure to enter into early marriage. The findings revealed that majority of in-school adolescent girls are in dire need of information on how to refuse teenage marriage and health effects of teenage marriage. This finding is not surprising as early marriage might likely disrupt their educational career as experience has shown that despite the promises by men to their prospective wives that they will be allowed to pursue an education after marriage, the young bride would inevitably need to drop out of school to nurse her babies and run her home (Uwais, 2010).
Female Genital Mutilation International organizations and agencies have increasingly recognized female genital mutilation as a health and human rights issue with serious socio-cultural implications (Umoh, 2005). From the analysis many of the respondents indicated that they need information on the health effects of female genital mutilation. Access to such information will empower the respondents to insist on their rights and also advocate for its eradication. Their protest might prompt the community leaders to have a rethink and publicly decry the practice. Family Planning Data collected revealed that majority of the respondents need information on different methods of pregnancy prevention and how to use them. This finding is supported by the study conducted by Sedgh, Rubina, Akinrinola and Susheela
44 (2007) which reported that almost 50 per cent of unmarried sexually active adolescent in Sub Saharan Africa have an unmet need for contraception. According to Biddlecom, et al cited by Juarez, LeGrand, Lloyd and Susheela (2008) high levels of unwanted pregnancy and abortion are evidence of the large unmet need for family planning among adolescents. Unsafe Abortion The in-school adolescent girls’ least desired reproductive health information is information on how to terminate pregnancy safely. Perhaps, they take safe way of terminating pregnancy as common knowledge. Previous studies indicated that adolescent girls resort to non-physicians such as patent medicine dealers who are located on street corners for their abortion needs and therefore they felt that they do not need such information (Olukoya and Ferguson, 2002; Olukoya, 2004).Their response may also be a reflection of their ignorance of the consequence of unsafe abortion. 4.6.4 Access to Reproductive Health Information Sources The finding that the respondents relied on information from parents, siblings, friends, school teachers on the one hand, and television and radio on the other for reproductive health information underscored the relevance of the two-step and multi-step flow models of the communication process to health information access. Studies conducted elsewhere in Africa by Bosompra (1989) and Musoke (2005) had similar findings. The result on the degree of access to reproductive health information sources indicates that the Internet, libraries and librarians were among the least accessible sources of reproductive health information. This is in consonance with the work of Odusanya and Bankole (2006) who reported that libraries (11.8%) and Internet (10.5%) were the least sources of HIV/AIDS information among secondary school students in Ogun State, Nigeria. That libraries were among the least used sources by the sampled girls is also in consonance with the findings of a study by Okiy (2004) which indicated that library was least used by the women sampled in South Senatorial District of Delta State, Nigeria. The libraries in the schools surveyed were in a sorry state and none of them had internet connectivity. Interestingly, the most accessible sources of reproductive health information mentioned by the students were parents, textbooks, television, siblings, radio, friends, school teachers, music and songs. This result corroborates the findings of
45 Ijatuyi (2004) and Mabawonku (1998) that interpersonal means and mass media are the leading sources of information among women in Nigeria. That parents are the leading accessible source of reproductive health information is in line with the current thinking as expressed in Christian Women Mirror (2009) that parents should start early to discuss sex and sexuality with their children. This finding conforms with that of Bammeke and Nnorom(2006) who reported that 57.55% of female adolescents spoke more with parents than friends (42.5%). A Focus Group Discussion Participant (FGD) CMS Girls Grammar School 2 also stated that: “My parents (especially my mother) shares with me her life experiences from that I get a lot of reproductive health information that are helping me in my relationship with boys. As I get closer to them some things that I don’t know they will explain them to me”.
However, this is contrary to the findings of Rani, et al (2003), Mohammadi (2006) and Odusanya and Bankole (2006) who reported that peers were the most important sources of reproductive health information. Text books were mentioned as the second most accessible source of reproductive health information. Another Focus Group participant at Wesley Girls’ Secondary School indicated that: “I prefer getting reproductive health information from text books because what I read I understand more and I can go back easily to it at any time. And from text books I see everything clearly.”
This is consistent with the report of Li, et al (2004) that in Northeastern Heilongjiang Province, China textbook on sex education was used to teach children in primary and secondary schools about sexuality. The interview revealed that government agencies scarcely organize programmes that are geared towards the provision of reproductive health information. But Action Health Incorporated- a non governmental agency occasionally organizes a programme tagged Teenage Festival of Life for the students. This annual programme creates room for reproductive health information dissemination among the students. The Action Health Incorporated also established Health and Life Planning Club in schools especially in Shomolu Local Education Districts. The Health and Life Planning Club holds regular weekly meetings during
46 which the peer educators address the students on issues related to sexual and reproductive health. During the activities of other clubs, the peer educators also disseminate reproductive health information through talks, dramas and role play. Other clubs such as Science Club, HIV/AIDS Club, and Princess Club create avenues for teachers to address issues related to reproductive health with the students. Regular morning assembly is another opportunity for teachers to provide reproductive health information to the students. The teachers sometimes engage the students on one-to-one counseling. 4.6.5 Access to Reproductive Health information Generally, the respondents’ opinion reveals that they had limited access to reproductive health information. HIV/STDs Prevention and Management In this context, the results revealed that information on HIV and sexually transmitted diseases prevention and management is easily accessible this may be as a result of the on-going campaigns by various groups in the country. This finding is consistent with earlier studies by Fawole, Asuzu and Oduntan (1999), Asuzu (1994) and Alao and Olaseha (1993) which reported a high level of awareness of AIDs among secondary school students in Nigeria. However, Cherie, et al (2005) contended that adolescents are often exposed to theoretical knowledge without exposing them to the skills in negotiating sexual relations and condom use. But this is contrary to the finding of Ayankogbe, et al (2003) who reported that there was little awareness creation about HIV/AIDS among secondary school students in Lagos State. As observed from the result, the most accessible reproductive health information is how to maintain healthy friendship with men without sex. Generally the prevention of unwanted pregnancy is the concern of most parents especially the mothers. The participants at the focus group discussion indicated that they do not have adequate access to reproductive health information. A Focus Group participant at Angus Memorial High School l stated that: “My mother will say … if a boy touches you, you will get pregnant, if a boy touches your vagina you will get pregnant and they will not give you full information, if my mother hears that any of my friends or some body I know is pregnant and may be dies, my mother will tell me have you heard it, if you like, go and get pregnant”
This finding is corroborated by Bammeke and Nnorom (2006) who found that more
47 female adolescents than males learn of the consequences of premarital sex amidst warnings to avoid the opposite sex from their parents especially mothers. Conformity to traditional norm which forbid sexual friendship among young unmarried person is the reason for passing such information. Mothers warn their daughters to avoid premarital sex and unwanted pregnancy because of the shame such brings to the girl and her family. But adolescents need comprehensive information on sexuality which promote their overall well being and prevent them from engaging in risky sexual behaviour. Family Planning In this study the respondents had limited access to information on different methods of pregnancy prevention and how to use them. Access to accurate information is necessary in decision making regarding health issues. Rolison (1998) affirmed that access to health information promotes healthy lifestyle choices and that prevention rather than cure had emerged as the way forward for public health. But some opined that providing adolescent access to information on different methods of pregnancy prevention and how to use them might promote sexual promiscuity and encourage the frivolous use of contraceptive (Akumadu, 1998; Baldol, 1993) This finding is in agreement with the reports of Amazigo, et al (1997) and Okonofua (1995) that a significant number of adolescents did not know about contraception.
Teenage Marriage The Child’s Right Act 2003 section 21 prohibits marriage of young people under the age of 18. The Act states that a person: (a) Who marries a child; or (b) to whom a child is betrothed; or (c) who promotes the marriage of a child; or (d) who betroths a child, commits an offence and is liable on conviction to a fine of N500,000 or imprisonment for a term of five years or to both such fine and imprisonment. But the result indicated that in- school adolescent girls in Lagos had limited access to information on how to refuse teenage marriage and health effects of teenage marriage. Inadequate access to such information then could be conceived as a violation of their rights.
48 Female Genital Mutilation Female genital mutilation deprives women and female children of their rights to sound health and physical well-being. The result revealed that in-school adolescent girls had limited access to information on effects of female genital mutilation. This is in spite of the fact that female genital mutilation poses serious physical and mental health risks for women and young girls (Population Reference Bureau, 2010). Besides, the hazardous health effects, female genital mutilation also has been known to be one of the most offensive means of violating the fundamental rights of women and female-children so recognized by various domestic and international legal instruments. Yet the respondents did not have adequate information on the medical complications arising from female genital mutilation which includes bleeding, pains, urinary infections, urine and vaginal leakages, chronic pelvic inflammatory diseases and HIV infections. Umoh (2005) observed that due to ignorance of the health implications of female genital mutilation young girls and women submit to such obnoxious cultural practices. He advocated that women and youths, who are not only the most likely victims but also change agents in the community, should be empowered through information that will give them the needed self-confidence to abandon such practice.
Unsafe Abortion From the result, it is disturbing to note that information on health consequences of unsafe abortion and how to terminate pregnancy safely is not easily accessible to in-school adolescent girls. The dearth of information on health consequence of unsafe abortion among in-school adolescent girls is worrisome based on the fact that previous studies by Otoide, et al, (2001), Sunmola, et al, (2003) and Olukoya (2004) reported high rate of morbidity and mortality from unsafe abortion among them. According to Smyke (1991) the most distressing fact about abortion-related deaths and illness is that the vast majority of the complications are preventable. She opined that maternal mortality and morbidity attributable to unsafe abortion could be minimized if all adolescents have access to family planning information and services. Olukoya (2004) also affirmed that the provision of information, life and livelihood skills, safe and supportive environment
49 are key in primary prevention of unsafe abortion. 4.6.6 Use of Reproductive Health Information It is obvious that the frequency of reproductive health information use is low. Similarly, Ayankogbe, Omotola, Inem, Ahmed and Manafa (2003), Glover, et al, (2003), Otoide, et al (2001), Laza (2000) and numerous others reported that although information on abortion and contraception was high, utilization of contraceptive and other risk reduction practices were low. This is in consonance with the observation of Wilson (1997) who pointed out that the fact that sources of information is accessible and processed (i.e. incorporated into the user’s frame work of knowledge, beliefs or values) is no guarantee that the information will be used. On the whole, most of the reproductive health information items were used annually. The implication of the finding is that the use of reproductive health information among in-school adolescent girls in Lagos State is erratic. HIV/STDs Prevention and Management Condom-related information appears to be the most used of all the reproductive health information. The result shows that the respondents use condom- related information quarterly. However, the Focus Group Participants expressed different views on the use of condom. Some spoke against the use of condom while others were favourably disposed to using it.
A focus group discussion participant at CMS Girls Grammar School 2 said that: “… I don’t think adolescent girls should use condom because they are still in school they are not suppose to use pregnancy prevention devices at all because it can prevent them from becoming pregnant later in life”.
Earlier studies on adolescents’ use of condom and contraceptives reported by Olukoya and Ferguson (2002) also indicated that condom use among adolescents is erratic. The use of other HIV-related information among the respondents is very low. This means that access to information should be backed up with skills in negotiation, critical thinking, decision- making and communication and incentives to adopt safe behaviours (UNICEF, 2002). Family Planning In this study the respondents indicated that they use pregnancy prevention information annually. The finding is consistent with the report of Bammeke and
50 Nnorom (2006) that although more than half of the respondents have heard of the term contraceptive before and have a good idea of its meaning, their knowledge and usage of specific ones is abysmally low. The fear of embarrassment and the potential negative consequences of contraceptive use on reproduction later in life accounts for low utilization of pregnancy prevention information. This result is also supported by the assertion of Otoide, et al (2001) that a plausible potential explanation for the low use of modern contraceptive methods among Nigerian adolescents arise from their perceived risk of side effects which includes interference with fertility. From their findings Aziken, et al (2003) attributed the low levels of contraceptive use among adolescents to inadequate knowledge and spontaneity of adolescent sexual activity. Teenage Marriage Teenage marriage undermines reproductive health of the adolescent girl. It places the adolescent girl at greater risk of teenage pregnancy, HIV and other sexually transmitted infections. Studies conducted in Kenya and India have shown that young women who were married to men much older than them were infected with HIV (UNICEF, 2002). Oftentimes teenagers are married to men much older than them and as young brides they lack the power to negotiate safe sex practices, this makes them to be vulnerable to HIV/AIDS and STIs than unmarried girls (UNICEF, 2002). Similarly, Nwagbara (2003) observed that the trend in most part of Nigeria moves towards teenage marriage in spite of the fact that under-aged wife stands greater health risks during pregnancy and child-birth than older women. The health hazards include obstructed labour which may result in vesico-vaginal fistulae, recto vaginal fistulae, infant and maternal mortality (Oyediran, 2006). From the analysis, the respondents’ use of information on the right time for a girl to marry is low. Perhaps, they are concentrating on their studies and are not under pressure to marry. It could also be that they are ignorant of the implications of teenage marriage. Female Genital Mutilation The respondents’ use of information on female genital mutilation is very low. This finding may be due to the fact that all the respondents reside in Lagos State where this cultural practice is rarely observed and some of them hardly travel to their states where adherence to this traditional practice is mandatory. Despite the low utilisation of this information item in-school adolescent girls need to be fully
51 informed of such practices and their negative health implications. 4.6.7 Attitude of in-school Adolescent Girls’ toward Reproductive Health Practices The study revealed that majority of the respondents has a positive attitude toward reproductive health practices as shown by the majority agreement with all the positive statements and disagreement with all the negatively worded statements. This implies that the respondents have a good understanding of reproductive health practices. A positive attitude towards reproductive health practices revealed by the study may probably be as a result of high level of access to reproductive health information sources which enabled the adolescent girls become knowledgeable of reproductive health practices. It is generally believed that knowledge of reproductive health practices should engender and promote attitudinal and behavioral change and this is consistent with the assertion of Amoakoh-Coleman (2006) that there is a considerable degree of positive correlation between knowledge, attitude and practice. This result therefore tallies with the findings in some studies conducted elsewhere among adolescents (Ocansey, 2006; Mohammadi, et al, 2006). The impact of access to information on their attitude to reproductive health practices according to the focus group participants has been positive. A Focus Group Discussion participant at Wesley Girls’ Secondary School stated that: “It (reproductive health information) has affected my attitude towards reproductive health practices. It has helped me to avoid some boys who speak nonsense and helped me to give them the right answer, than for me to fall for them easily.”
Another participant at Angus Memorial High School l affirmed that: “Yes, it (reproductive health information) is very useful. I practice assertiveness by saying No to sex and bad influence. It has helped me to prevent pregnancy to know my health status, to practice sexual abstinence and to have self esteem”
They also express negative attitude towards abortion, teenage marriage, female genital mutilation and premarital sex. A member of Roman Catholic Church among the participant at Wesley Girls’ Secondary School said that sex before marriage is not acceptable in her church. They maintained that abortion can destroy a girl’s womb and this may cause infertility later in life. Some opined that female circumcision and teenage marriage can lead to prolonged labour and death among
52 girls. The guidance counselors interviewed also maintained that access to reproductive health information has positive impact on the attitude of some of the students as cases of negative sexual behaviour among the students are minimal.
4.6.8 Constraints to Access to Reproductive Health Information The finding about lack of time to seek relevant information as major constraint to information access agrees with that of Kitto (1998) who reported that the excessive work load which the society imposes on girls hinder them from accessing reproductive health information. At home girls perform multiple roles which range from food preparation to house cleaning, laundry, taking care of other members of the family and so on. At home, parent’s unwillingness to discuss reproductive health issues such as sex with the adolescents is another major obstacle to reproductive health information access. This finding is not at variance with previous studies by Manda (2006),Akumadu (1998), Baldo (1993), Bammeke and Nnorom (2006) among others who from their studies found that discussion on issues relating to sex between parents and children are generally indirect and superficial. Consequently, reproductive health issues such as protection from HIV/STIs and prevention of pregnancy are not adequately addressed. At school the challenges the guidance counselors face in the provision of the reproductive health information includes non-inclusion of reproductive health in the school timetable, and excess work load. During the interview process, a guidance counselor in Festac Girls Secondary School observed that: “Family life education is not in the timetable and their subjects are so many, except it will be integrated into biology or any other subject, it is only once a week during school assembly that teachers or people from some NGOs or churches visit the school to speak with the students”.
This implies that the approved National Comprehensive Sexuality Education Curriculum has not been fully implemented in public secondary schools in Lagos State. And perhaps none of the schools surveyed is among the selected pilot schools for the sexuality education project in the state. The guidance counselors are also subject teachers. The class work load does not give them sufficient time to effectively engage the students in one to one counseling.
53 4.6.9 Constraints to use of Reproductive Health Information The results of this study showed that major obstacles to use of reproductive health information were inability to get reliable and accurate information and inadequate knowledge of reproductive health. This is as a result of the conspiracy of silence on sexuality issues by the parents, the family, the school, the state and other stakeholders which promote gap in knowledge. A poor state of reproductive health information is a reflective of poor knowledge of reproductive health. The unwillingness of parents to discuss sex and other reproductive health issues with their daughters at home, the absence of school libraries and the inability of teachers to provide adequate reproductive health information at school all together promote gap in knowledge. Wilson (1997) and Maclnis and Jaworski (1991) support the findings of this study by their proposition that the more knowledgeable the individual, the easier they will find acquisition and utilization of information. Bammeke and Nnorom (2006) also lend credence to the finding of this study by reporting that knowledge and usage of contraceptive among adolescents is very low. Fear of embarrassment was another major factor that affected use of reproductive health information. This result is in agreement with the report of Nare, et al (1997) who observed that adolescents’ use of contraception was surrounded with many negative feelings such as embarrassment, fear of stigmatization and fear that their parents may find out. Baldo (1996) asserts that these adolescents are embarrassed about their reproductive health issues because the societies themselves are embarrassed about it. 4.6.10 Relationship between Access to Reproductive Health Information and Attitude towards Reproductive Health Practices The test of significance of relationship between access to reproductive health information and attitude towards reproductive health practices has shown that there is a significant positive relationship between access to reproductive health information and attitude towards reproductive health practices with Pearson moment correlation value (r=0.107, P < 0.05). On this premise, hypothesis 1 which states that there is no significant relationship between access to reproductive health information and attitude towards reproductive health practices was thus rejected. The interpretation of this is that access to reproductive health information exerts great influence on attitude towards reproductive health practices. In other words, if
54 in-school adolescent girls have access to more reproductive health information they will be more favourably disposed (have positive attitude) towards reproductive health practices. This finding is in agreement with Curras (1987) and Opeke (2004) assertions that information has the ability to modify attitudes and behaviors and to empower potentially disadvantaged groups such as youths, women and children. Okwilagwe and Vome (2002) also affirmed that information has the potentials to modify and direct human behavior towards a predetermined direction. The finding of this study is not at variance with Ikwuako (2001) who observed that awareness of positive reproductive health practices influences attitude of young adults towards reproductive health. 4.6.11 Relationship between use of Reproductive Health Information and Attitude towards Reproductive Health Practices The result of the study has revealed that the relationship between the frequency of use of reproductive health information and attitude towards reproductive health practices was negative and statistically not significant. (r= -.009, P> 0.05. On the basis of this result, hypothesis 2 which states that utilization of reproductive health information and attitude towards reproductive health practices are not significantly related was not rejected. The negative correlation between use of reproductive health information and attitude to reproductive health practices is not in line with the study conducted by Okwilagwe (1993) in which use of information gained from reading of books on sex was related to avoidance of unwanted pregnancy. It is also not in agreement with Richter, Valois, Mckeown, Vincent (1993) report of a strong correlation between the failure to use condoms and reckless behavior. The finding of this study is also at variance with Bruckner, Martin and Bearman (2004) who revealed that contraceptive use was strongly correlated with attitude toward contraception. It seems that this result supports the study by Lee and Wu (2004) which indicated that media use in general appears to have little impact on attitudes toward Asian Americans.
4.6.12 Relationship between Access to and use of Reproductive Health Information and Attitude toward Reproductive Health Practices The third hypothesis addresses the relationship between the three variables. The result of the tested hypothesis in Table 4.10 indicates that access to and use of reproductive health information jointly had significant linear relationship with
55 attitudes towards reproductive health practices. In-school adolescent girls’ attitude towards reproductive health practices can be influenced by access to and use of reproductive health information taken together. In other words, Table 4.10 revealed that there exist a significant linear relationship between access to and use of reproductive health information and attitude of in school adolescent girls towards reproductive health practices in co-educational and single sex girls secondary schools in Lagos State. The implication of this is that the combination of the two variables (access to and use of reproductive health information) has significant effect on in-school adolescent girls’ attitudes towards reproductive health practices. This implies that the higher the level of access to and use of reproductive health information by in- school adolescent girls, the more they will develop positive attitude towards reproductive health practices. Thus, the study has shown that adolescent girls’ access to and use of information as well as their attitude to reproductive health practices is a complex and intricate process that involved a number of factors and depended to a large extent on the situation. More so, information use is dependent on the context of use as well as personal attributes. This result is supported by Ludvigsson (2003) who reported that doctor-mediated breast feeding information given before birth or on the maternity ward was associated with giving colostrums and avoidance of prelacteal foods. Musoke (2005, p.6) also lend credence to the finding of this study by affirming that” when they (her respondents) accessed information and used it, some of that information changed their states of knowledge, values beliefs, attitudes and behavior. This led to the various actions that put the knowledge acquired into practice or applied the information gained in various ways, which improved or promoted health”
4.6.13 Access and use of Reproductive Health Information as Predictors of In- school adolescent Girls’ Attitude to Reproductive Health Practices The analysis revealed that the respondents’ level of access to reproductive health information is highly significant factor in predicting their attitude towards reproductive health practices where as their use of reproductive health information is not the significant factor. The finding is consistent with the report of Bammeke and Nnorom (2006) that although more than half of the respondents have heard of the term contraceptive before and have a good idea of its meaning, their knowledge
56 and usage of specific ones is abysmally low. The results of this study are corroborated by Wilson (1997) who explained the fact that sources of information are available and accessible and information is processed (i.e incorporated into user’s framework of knowledge, beliefs or values) is no guarantee the information will be used (i.e lead to changes in the user’s state of knowledge, behaviors, values or beliefs). In her study, Musoke (2005) asserted that some obstacles” intervene to prevent information use, that is, they intervene after information acquisition and processing, but before information use, hence stopping the information or knowledge from being put to use. Thus, the study revealed that adolescent girls’ access to and use of information as well as their attitude to reproductive health practices is a complex and intricate process that involved a number of factors and depended to a large extent on the situation. More so, information use is dependent on the context of use as well as personal attributes. The findings of this study as regards to the significant contribution of access to reproductive health information on attitude towards reproductive health practices and insignificant contribution of use of reproductive health information should not be interpreted to imply that use of reproductive health information has no influence on in-school adolescent girls’ attitude towards reproductive health practices. It could perhaps imply that access to reproductive health information is of more importance in the explanation of in school adolescent girls’ attitude towards reproductive health practices than the other variable (use of reproductive health information). However, since the results have shown that access to reproductive health information is more important than use of reproductive health information, there is then the need for policy makers and implementers to increase access to reproductive health information through the provision of age-appropriate comprehensive sexuality information programmes based on the needs and experiences of in-school adolescent as a way of mitigating their reproductive health problems.
4.6.14 Difference in Access and use of Reproductive health information and Type of school The result of the study has revealed that there is no statistically significant difference in access to and use of reproductive health information among girls in single sex and co-educational schools. This implies that the type of school they
57 attend does not make any significant difference in their access to and use of reproductive health information. This finding is at variance with Borire, Oyekunle, Izekor and Akinlonu (2008) who reported that there was statistically significant relationship between condom use and type of school. Furthermore, since the result of this study indicated that the level of access to and use of reproductive health information is the same in both co-educational and single sex girls’ schools in Lagos State concerted efforts should be made to provide reproductive health information resources and facilities equally in all public secondary schools in the state.
CHAPTER FIVE SUMMARY OF FINDINGS, CONCLUSION AND RECOMMENDATION 5.0 Introduction This chapter is devoted to the presentation of the summary of findings, conclusion and recommendations drawn from the analysis of the research data. 5.1 Summary of Findings 1. The major findings of the study as revealed by the analysis are as follows: Majority of the in-school adolescent girls who by this study, represent the adolescent group in the society, have no access to reproductive health materials due to the non-availability of such information resource in their schools. The few schools that attest to having libraries, have nothing but room spaces that had less than 10 reproductive health materials for the teaming population of students found in the schools. 2. The reproductive health information greatly required by in-school adolescents girls were information on how to maintain healthy friendship with men
58 without sex, how to avoid HIV/AIDS and other sexually transmitted infection, how to control sexual desire, where to go for HIV test, how to identify signs of HIV/AIDS and sexually transmitted infections, how to refuse teenage marriage, health effects of female circumcision and information on different methods of pregnancy prevention. 3. The most easily accessible sources of reproductive health information were in this order: parents, textbooks, television, siblings, radio, friends, school teachers, music and songs. 4. The in-school adolescent girls appear to have a limited access to reproductive health information. The reproductive health information items that were most easily accessible to them were information on how to maintain healthy friendship with men without sex, how to avoid HIV/AIDS and other sexually transmitted infections, how to control sexual desire, where to go for HIV test, how to identify signs of HIV/AIDS and sexually transmitted infections. 5. Most reproductive health information items were used annually. 6. The respondents had positive attitude towards reproductive health practices. 7. The major factors which hinder the respondents from accessing reproductive health information were lack of time to seek relevant information , unwillingness of my parents to discuss reproductive health issues with me as an adolescent , lack of awareness about sources of reproductive health information, reproductive health information is not easy to obtain , poverty and low socio-economic status , unwillingness of my teachers to discuss reproductive health issues with me as adolescent and reproductive health information resources and facilities are not available. 8. The major obstacles to use of reproductive health information were inability to obtain reliable and accurate information, fear of embarrassment in the event of using the information, inadequate knowledge of reproductive health, negative attitudes of health care providers, religious beliefs and retrogressive cultural beliefs. 9. Access to reproductive health information was found to be significantly related to their attitude to reproductive health practices. 10. The frequency of use of reproductive health information was not significantly related to their attitude towards reproductive health practices. 11. The level of access to and use of reproductive health information when
59 taken together would significantly predict in-school adolescent girls’ attitude towards reproductive health practices. 12. With respect to school type the study revealed that no significant difference existed in level of access to and frequency of use of reproductive health information.
5.2 Implications of the study The findings of the study have demonstrated the fact that the attitudes of in- school adolescent girls towards reproductive health practices are related to their level of access to reproductive health information. The direct implication of this revelation is that as their level of access to reproductive health information increases, their attitudes towards reproductive health practices would be more positive. It is, therefore, imperative that the school libraries in these schools should be made functional and equipped with reproductive health information resources in order to improve access to reproductive health materials. The libraries should also be connected to the Internet so that the students could access online reproductive health resources. Furthermore, there should be frequent seminars, symposia and workshops for both the students and their teachers on topical issues on reproductive health. Resource persons with extensive and in-depth knowledge of reproductive health should be invited to do presentations or to facilitate the sessions. The female students should be encouraged to be actively involved in the discussions. The findings from the study indicate that the frequency of use of reproductive health information is low and that most reproductive health information items were used annually. Similarly, more than forty per cent (40%) of the respondents had never used reproductive health information. The failure to use reproductive health information accessible to the adolescents has a lot of implication. The consequence is that the adolescents who engage in risky reproductive health behaviors may experience sexuality-related problems such as HIV/AIDS, unwanted pregnancy, abortion in unsafe conditions which could result in infertility, severe morbidity and death. In view of the indication that parents are the most accessible source of reproductive health information for in-school adolescent girls, parents should rise
60 up to the challenge and ensure that the silence on sexuality issues among adolescents is broken. Bammeke and Nnorom (2006) asserted that the conspiracy of silence on sexuality issues by the family, the school, the state and other stakeholders increases adolescents’ vulnerability to sexuality-related risks. And this according to them has human, social and economic development costs. They advocated the provision of comprehensive sexuality information and education which will empower the adolescents to take informed and responsible decisions that would protect their reproductive health. The in-school adolescent girls interact daily with their parents and they rely on them for reliable and accurate information, it is therefore expedient that the parents should create conducive environment that will enable the girls to ask questions, express their thoughts and ideas and seek clarification on reproductive health issues. Amoran and Fawole (2008) urged parents especially mothers to promote reproductive health practices by giving information and education on reproductive health matters. Some factors were found to inhibit access to and use of reproductive health information. The major constraints were inability to get reliable and accurate information, unwillingness of my parents to discuss reproductive issues with me as an adolescent, fear of embarrassment in the event of using the information, lack of time to seek relevant reproductive health information and inadequate knowledge of reproductive health. Others include lack of awareness about sources of reproductive health information, lack of school library, radio, television and newspapers are not readily available, unwillingness of my teachers to discuss reproductive health issues with me as an adolescents and negative attitude of health care providers. The implication is that since access to and use of reproductive health information jointly predict positive attitude towards reproductive health practices, if these deterrents are not addressed urgently negative attitudes towards reproductive health practices will persist.
5.3 CONCLUSION School libraries are established to cater for the information needs of the in- school adolescents. They are to select, acquire, organize, preserve and disseminate information to their users and this includes reproductive health information. This study has established that access to and use of reproductive health information jointly significantly predict attitude towards reproductive health practices.
61 Precisely, access to reproductive health information and in-school adolescent girls’ attitude towards reproductive health practices in the schools surveyed are significantly correlated. The utilization of reproductive health information is low. This cannot be divorced from their inability to get reliable and accurate information and fear of embarrassment. However, days in which reproductive health discussions are regarded as taboos are gone and parents, teachers, health practitioners, government and non-governmental organizations should rise up to the challenge and provide useful and age appropriate information on reproductive health to the adolescents. 5.4 RECOMMENDATIONS Based on the findings of this study, the following recommendations are suggested to improve access to and use of reproductive health information among in-school adolescents. The state government should make specific annual budgetary allocation for the developing and maintaining of the school libraries in all public secondary schools in the state. These libraries should be stocked with current reproductive health materials in print and non-print formats. The school libraries should be connected to the Internet. Regular workshops, seminars, symposia, lectures and talks aimed at promoting access to and use of reproductive health information should be organized for parents, teachers, health care workers and students. The National Comprehensive Sexuality Education curriculum should be implemented in all public secondary schools and this should reflect in the school timetable. All school libraries should be manned by trained professionals with at least diploma in library and information studies. The school librarian should ensure that reproductive health information is downloaded and repackaged at the level of the students. Multi-media approach should be adopted for the dissemination of reproductive health information in public schools in Lagos State. A blend of interactive strategies geared towards helping adolescent girls to feel comfortable with sexuality-related topics while limiting potential intimidation and embarrassment should be promoted. There is need for more aggressive efforts by all stakeholders-parents,
62 teachers, government and non-governmental agencies to provide reproductive health information to adolescent girls so that an entire generation might not go into extinction because of the consequences of risky sexual behaviours. 5.5 Contribution of the Study to Knowledge If the in-school adolescent girls have access to libraries (school and public) that are fully equipped with a variety of reproductive health materials, they would be favourably disposed towards reproductive health practices. Health talks, symposia, seminars could provide avenue for in-school adolescent girls to have access to reproductive health information that could affect their attitude towards reproductive health practices. In-school adolescent girls are conscious of their reproductive health information needs. The government and non-governmental agencies should integrate all available sources of information to enhance accessibility of reproductive health information needs of this group.
5.6 SUGGESTIONS FOR FURTHER RESEARCH This study investigated in-school adolescent girls’ access to and use of reproductive health information and attitude towards reproductive health practices in Lagos State, Nigeria, future research should include out-of-school adolescent girls. This population may have an even greater need for reproductive health information and may have fewer resources to meet that need. Access to and use of reproductive health information among adolescent boys also could be investigated. The relationship between socio-demographic variables and access to and use of reproductive health information can be researched upon. Furthermore, research in attitudes and beliefs of teachers, parents and policy makers could help lead to insights on how to gain their support for comprehensive sexuality information and education.
63 REFERENCES
Aaker, D.A., Batra, R. and Myers, J. G. 1992. Advertising management. 4 th ed. Englewood Cliffs, NJ: Prentice Hall. Aboyade, B.O. 1987. The provision of information for rural development. Ibadan: Foundation publications. Action Health Incorporated. 1997. Teenage festival of life. Growing Up. 2. ------. 2006. Integration of sexuality education in Lagos State schools. Retrieved Oct.30,2006 from http://www.actionhealthinc.org/ articles/article002.htm. Adedimeji, A. 2005. Perceptions of HIV/AIDS infection and condom use among undergraduates in a Nigerian University. Journalists against AIDS Nigeria. Retrieved May 14,2006 from http://www.nigeria- aids.org/reports.cfm? read= 32. Adegbola, O. and Babatola, O. 1999 Premarital and extramarital sex in Lagos, Nigeria.The continuing HIV/AIDS epidemic in Africa:responses and coping strategies. I.O. Orubuloye, J.C. Caldwell and J.P.M. Ntozi. Eds. Health Transition Centre, National Centre for Epidemiology and Poplation Health, Australian National University, Canberra. Ademuwagun, Z. A. 1985. The Principles of health education. Principles and practice of community health in Africa. G.O. Sofoluwe and F. J. Bennett. Eds. Ibadan : University Press Limited. Adomi, E. E., Obarakpor, E. F. and Akparobore, D. C. 2005. The Use of Information Technology by electronic media workers in Delta State, Nigeria. The Electronic Library. 23.3:295-301. Afullo, J. J. 2000. Global information and Africa: the telecommunication infrastructure for cyberspace. Library Management. 21.4: 205-213.
64 Ajuwon, A. J. 2006. Attitudes, norms and experiences of sexual coercion among young people in Ibadan, Nigeria. Sex without consent: young people in developing countries. S. J. Jejeebhoy, I.Shah and S.Thapa Eds. London: Zed Books. Ajzen, I. 1988. Attitudes, personality and behaviour. Attitude structure and function. A. R. Pratkanis, S. J. Breckler and A. G. Greenwald Eds. Hills-dale, NJ: Erlbaum. Akumadu, T. U. 1998. Beasts of burden: a study of women’s legal status and reproductive health rights in Nigeria. Lagos: Civil Liberties Organisation. Alabi, B.2004. Evolving role of ICT in teaching research. Nigerian Tribune. Apr. 30 :30 Amazigo, U; Silva, N.; Kaufman, J; and Obikeze, D. S. 1997. Sexual activity and contraceptive knowledge and use among in-school adolescents in Nigeria. International Family Planning Perspectives. 23: 28-33. Ampofo, K. 1990. Epidemiology of vesico vaginal fistula in Northern Nigeria. West African Journal of Medicine. 9. 2: 98-102. ------. 1990. Risk factors of vesico vaginal fistula in Maiduguri, Nigeria: a case control study. Tropical Doctor 20.3: 138-139. Anasi, S. N.I. 2004. Audiovisual media capabilities and the dissemination of health information. Library Focus. 22: 50-60. Araoye, M.O. 1998. Knowledge and attitude of secondary school teachers towards reproductive health education in school. The Nigerian Journal of Guidance and Counselling. 6 1,2:67-78. ------and Adegoke, A. 1996. AIDS- related knowledge, attitude and behaviour among selected adolescents in Nigeria Journal of Adolescence. 19:179- 181. ------and Fakeye, O. O. 1998. Sexuality and contraception among Nigerian adolescents and youth. African Journal of Reproductive Health. 2: 142-150. Asuzu, M.C. 1994. Sexual beliefs, attitudes and knowledge of adolescents’ youths in Ibadan concerning AIDS. West African Journal of Medicine, 13.4: 245-247. Averting HIV and AIDS 2006. HIV and AIDS in Nigeria. Retrieved Feb.1, 2006 from http//www.avert.org/ aids- nigeria.htm Ayankogbe,O.O. Omotola, B.D., Inem, V.A., Ahmed, O.A. and Manafa, O.U. 2003. Knowledge. Attitudes, beliefs and behavioural practices for creating awareness about HIV/AIDS in Lagos State, Nigeria. Nigeria Medical Practitioner. 44.1:7-10. Aziken, M.E.; Okonta, P.I. and Ande, A.B.A. 2003. Knowledge and perception of emergency contraception among female Nigerian undergraduates. International Family Planning Perspectives, 29.2: 84-87. Babalola, S.1993. Mobile family planning drama. Promotion and Education – International Journal of Health Promotion and Education. 42-45. Badawi, G.A. 2005. The Librarians challenges in Nigeria’s fight against HIV\AIDS: a case study of Kano state. In the compendium of papers presented at the 43rd National Annual conference and AGM of the Nigerian Library Association held at June 12 cultural center, Abeokuta, 9-15 July 2005 pp. 13- 23. Baldo, M. 1993. Does sex education lead to earlier or increased sexual activity in youth? In Abstract on Report of Ninth International Conference on Aids. Berlin, June 6-11, 1 & 11. Bettman, J.A. 1978. Consumer information acquisition and search strategies. The Effects of information on consumer and market behaviour. A. A. Mitchell. Ed. Chicago: American Marketing Association. Bii, H. K. and Otike, J. 2003. Provision and accessibility of health information to the rural communities in Kenya: A case study of Bomet district. African Journal of Library, Archival and Information Science. 13.2: 155-174 Boerma, T. 2005. Setting the numbers right. Bulletin of World Health Organisation, 83.8 :567-568. Brabin, L. 1995. Reproductive tract infections and abortion among adolescent girls in rural Nigeria. Lancet. 345: 300-304. Buga, G., amoko, D., Ncayiyana, D.J. 1996. Adolescents’ sexual behaviour, knowledge and attitudes to
65 sexuality among school girls in Transkei, South Africa. East African medical Journal 73.2: 95-100. Butkovich, N.J. 1996. User studies : a selective review. Journal of Information Studies.4.2:359-368. Chandrasekhar, C. P. and Ghosh, J. 2001. Information and communication technologies and health in low income countries: the potentials and constraints. Bulletin of the World Health Organisation. 79:9. Chowdhury, S., Goswani, A.,Amar,S.1993 Sexual behaviour and perception of Risk in youth of urban slums of Delhi,India. International Conference on AIDS. 9.2, 951 (abstract no. PO-D37-4399) June, 6-11. Cleveland, M. 2000. Archetypal fears and female circumcision. Vision watch. April-June. Project Alert on Violence against women. 8. Choo, C. W. and Austeer, E. 1993. Enviromental scanning: acquisition and use of information. Annual Review of Information Science and Technology. 28; 279-314. Darkwa, O. and Mazibuko, F. 2005. Creating virtual learning communities in Africa: challenges and prospects. Retrieved June7,2005 from http://www./firstmonday.org/issues/issue5-5/darkwa/. Davis, G. B. 1974. Management information systems: conceptual foundation, structure and development. 2nd ed. London: McGraw-Hill. Dawood, N.; Govender, K. and Chohan, E. 2006. Knowledge, attitudes and sexual practices of adolescents with mild retardation, in relation to HIV/AIDS. African Journal of AIDS Research 5.1:1-10.Retrieved Oct.16,2006 from http:/www.ajol.info.viewarticle.php?jid=46 &:d=25550&layout=abstract. Dervin, B. 1992. From the mind’s eye of the user: The sense-making qualitative and quantitative methodology. In J. Glazier and R. Powell (eds.), Qualitative Research in Information Management pp. (61-84). Englewood: Libraries Unlimited. Effah-Chukwuma, and Osarenren, N. 2001. Beyond boundaries. Lagos: Project Alert on Violence Against Women. Ellis, D. 1989. A behavioural approach to information retrieval design. Journal of Documentation. 45, 3:172- 212. Eriksson-Backa, K.2003. Who uses the web as a health information source? Health Informatics Journal, 9.2: 93- 101. Erulkar, A, Mekbib, T. A., Simie, N, Gulema, T. 2005. Adolescent life in low income and slum areas of Addis Ababa , Ethiopia. Accra: Population Council. Erulkar, A.S., Ettang, L.I. A., Onoka, C. Nyagah, F.K. and Muyonga, A. 2004. Behaviour change evaluation of a culturally consistent reproductive health program for young Kenyans. International Family Planning Perspectives. 30.2. 58 – 67. Evelyn, U. I. and Osafu, O. 1999. Sexual behaviour and perception of AIDS among adolescent girls in Benin City, Nigeria. African Journal of Reproductive Health. 3: 39-44. Fatoki, O. C. 2005. Prospects of GSM technology for academic library services. The Electronic Library. 23. 3:266-273. Fawole, O. I.; Asuzu, M. C., and Odunta, S. O. 1999. Survey of knowledge, attitude and sexual practices relating to HIV infection/AIDS among Nigerian Secondary School Students. African Journal of Reproductive Health 3.2: 15-24. Fazio, R. H. 1986. How do attitudes guide behaviour? Handbook of motivation and cognition. R.M. Sorrentino and E. T. Higgins Eds. New York: Guilford Press. ------, Sanbonmatsu, D. M., Powell, M. C. and Kardes, F. R. 1986. On the automatic activation of attitudes, Journal of Personality and Social Psychology. 50:229-238. Federal Ministry of Health, Nigeria. 1996. National health policy 1995-2005. Lagos: Federal Ministry of Health. ------2001. National HIV/Syphilis sentinel survey among pregnant women attending antenatal clinics in Nigeria, Abuja: Federal Ministry of Health ------. 2001. National reproductive health policy and strategy to achieve quality reproductive and sexual health for all Nigerians. Abuja: Federal Ministry of Health.
66 ------.2003.National HIV/AIDS reproductive health survey. Abuja: Federal Ministry of Health, Nigeria. ------. 2004. Technical report on the 2003 National HIV/Syphilis sentinel survey among pregnant women attending antenatal clinics in Nigeria, Abuja: Federal Ministry of Health. Ferreira, A., and Maool, S. (1994) Training health agents for prevention in urban low socio-economic status women. International Conference on AIDS, 10.1, 328(abstract no. PD01357), August 7-12. Feyisetan, B. and Pebley A. 1989. Premarital sexuality in urban Nigeria. Studies in Family Planning 20.6: 343- 354. Fikree, F.F., Khan, A., Kadir, M. M., Sajan, F. and Rahbar, M. H. 2001. What influences contraceptive use among young women in urban squatter settlements of Karachi, Pakistan? International Family Planning Perspectives 27.3: 130-136 Fishbein, M. and Ajzen, I. 1975. Belief attitude, intention and behaviour: an introduction to theory and research. Menlo park, Calif:Addison-Wesley Publishing, Co., Inc. Folorunsho, O. 2000. AIDS information needs, sources and attitudes of secondary school students in Osun State. MLS project. Department of Library, Archival and Information Studies, University of Ibadan. Gann, R. 1986. The Health information handbook. Hants: Gower. Gericke, E. M. 1998. Serving the unserved in the year 2000. International Federation of Library Associations Journal. 24;20-28. Germain, A. 1987. Reproductive health & dignity: choices by third world women technical background paper prepared for the international conference on better health for women and children: through family planning held in Nairobi, Kenya. October 5-9, 1987. International Women’s Health Coalition, New York. Glover, K. E., Bannerman, A., Pence, B. W., Jones, H., Miller, R., Weiss, E. and Nerquaye-Tetteh, J. 2003. Sexual health experiences of adolescents in three Ghanaian towns. International Family Planning Perspectives. 29.1: 32-40. Godlee, F., Pakenham-Walsh, N., Cohen and Paker 2004. Can we achieve health information for all by 2015.The Lancet. 364.9430: 295-300. Gorgen, R., Yansane, M.L., Marx, M., Millimounou, D. 1998. Sexual behaviour and attitudes among unmarried urban youth’s in Guinea. International Family Planning Perspectives. 24.2: 65-71. Grunseit, A. et al. 1997. Sexual education and people’s sexual behaviour: a review of studies. Journal of Adolescent Research. 12.4: 421-453. Hall, B.L. 1987. Mass communication and adult education.An introduction to the study of adult education. B. Lalage and J.T. Okedara (eds). (pp 224-229). Ibadan: University Press Limited. Hu, D.J. Torel, C. and Kim-Farley, R. 1994. The computerized information system of the expanded programme on immunization. World Health Forum. 15.1: 238-239. Ijatuyi, A.O. 2005. Awareness and use of information as predictor of women’s management of the physical environmental in Ondo State, Nigeria. Ph.D. Thesis. University of Ibadan. Ikamba, L. M. and Ouedraogo, B. 2003. High-risk sexual behaviour: knowledge, attitudes and practice among youths at Kichangani Ward, Tanga, Tanzania. Action Research, e-reports. Retrieved Apr.10, 2006,from http://www2.fhs.usyd.edu.au/arow/arer/018.htm. Ikwuako, C. 2001. The development and effects of information, education and communication (IEC) strategies on young adults’ reproductive health practices in Lagos State. Ph.D. Thesis. Department of Adult Education. University of Lagos. International Clinical Epidemiology Network 2006. Adolescent health. INCLEN Research: International Clinical Epidemiology Network. RetrievedSept.25,2006,from http://www.inclen.org/research/ah.html . International Planned Parenthood Federation. 1994. Understanding adolescents. An International Planned Parenthood Federation Report on young people’s sexual and reproductive health needs, 4, 5 Introna, L. D. 1997. Management, information and power: a narrative of the involved manager. London: Macmillan Press Ltd.
67 Isamah, A. N; Owumi, B. E.; Adewumi, F.; Okunola, R. 1998. The impact of price reform on the health and productivity of rural women in Southern Nigeria. Ibadan: Nigerian Institute of Social & Economic Research (NISER). Iwe, J. I. 2005. Enhancing women’s productivity in the library and information sector in Nigeria. The Electronic Library 23.3: 319-332. Jacobson, J. L. 1993. Women’s health: The price of poverty. The health of women: a global perspective. M. Koblinsky; J. Timyan and J. Gay Eds. Colorado: West view press Inc. Jegede, A.S. and Odumosu O. 2003. Gender and health analysis of sexual behaviour in South-Western, Nigeria. African Journal of Reproductive Health. 7.1: 63-70. Jejeebhoy, S.J. and Bott, S. .2006. Non-consensual sexual experiences of young people in developing countries: an overview. Sex without consent: young people in developing countries. S. J. Jejeebhoy, I. Shah and S. Thapa Eds. Zed Books: London. Jimba, S. W. 2000. Accessibility to information technologies, their value-in-use and user attitudes among scientists using agricultural libraries in Nigeria. Ph.D. Thesis. University of Ibadan. Johnsonson, J.D. and Meischke, H. 1991. Cancer information: women’s source and content preferences. Journal of Health Care Marketing, 11,37-44. Joint United Nations Programme on HIV/AIDS. 1999. Report on a consultation on the socioeconomic impact of HIV/AIDS on household, Chiang Mai, Thailand. Geneva: UNAIDS. Kaaya, S.F, Flisher, A.J. Mowambo, J.K; Schaalma, H., Aaro, L. E. and Klepp, K. 2002. A review of studies of sexual behaviour of school students in sub-saharan Africa. Scandinavian Journal of Public Health 30.2: 148-160. Kibret, M. 2003. Reproductive health knowledge, attitude and practice among high school students in Bahir Dar, Ethiopia. African Journal of Reproductive Health 7.2: 39-45. Kitto, D. 1998. Reproductive health information: Accessibility and utilization by adolescents and youths in Kiboga District, Kampala. Retrieved Sept.25, 2006 from http://www.nutrition.uio.no/ARHNe/new/Thesis- Dissertations/kitto.pdf Kim, Y. M., Kols, A., Nyakauru, R., Marangwanda, C. and Chibatamoto, P. 2001. Promoting sexual responsibility among young people in Zimbabwe. International Family Planning Perspectives. 27.1: 11- 19. Kinsman, J. et al. 2001. Evaluation of a comprehensive school–based AIDS education programme in rural Masaka, Uganda. Health Education Research: Theory and Practice, 16.1: 85-100 Kirkby, D. 2001. Emerging answers: research findings on programs to reduce teen pregnancy, Washington, D.C.; National campaign to prevent teen pregnancy. Kivits, J. (2005). “Health information on the internet: researching information seekers and practices in a mediated health context” Ph.D Thesis. Retrieved Jan.23 2006 from http://www.ise.ac.uk/collections/media@ise/ Krejcie, R. and Morgan, D. W. 1970. Determining sample size for research activities. Educational Psychological Measurement.30: 607-610. Kuhlthau, C. C. 1993. A principle of uncertainty for information seeking. Journal of Documentation. 49,4: 339- 355. Lee, M.K.O. and Pow, J.1996. Information access behaviour and expectation of quality: two factors affecting the satisfaction of users of clinical hospital information systems. Journal of Information Science. 22 (3), 171- 179. Lee, R. M. 1993. Doing research on sensitive topics. London: Sage. Li, Y., Cottrel, R. R., Wagner, D.I., and Ban, M. 2004. Needs and preferences regarding sex education among Chinese college students: a preliminary study. International Family Planning Perspectives 30.3: 128-133. Lotrean, L. M. and Laza, V. 2000. Knowledge, attitudes, beliefs and practices regarding condom use among students from Cluj-Napoca, Romania.Retrieved Oct. 25,2006 from
68 http://gateway.nlm.nih.gov/meetingabstracts/ 102242199.html.. Mabawonku, I. 1998. Health Information provision to semi-urban people in Oyo state, Nigeria: What role for library and information centres? African J. A. Library, Archives and Information Science. 8. 2:127-138. Maclnnis, D. J. and Jaworski, B.J. 1991. Enhancing and measuring consumers’ motivation, opportunity, and ability to process brand information from advertisements. Journal of Marketing, 53, 1-23. Malim, T. and Birch, A. 1998. Introductory psychology London: Macmillan Press Ltd. Makinwa –Adebusoye,P.1992. Sexual behaviour, reproductive knowledge and contraceptive use among urban youth in Nigeria. International Family Planning Perspective. 18.2: 66-70. ------. 1991. Adolescent reproductive behaviour in Nigeria: A study of five cities. NISER monograph series, 3. ------. 1991. Contraception among urban youth in Nigeria. Proceedings of the demographic and Health Surveys World Conference. 2155-2171. Manda, P.A. 2006. HIV\AIDS information flow and access: experiences from Babati district, Tanzania. University of Dar es Salaam Library Journal, 8 .1, 2: 49-59 Mane, P. and McCauley, A. P. Impact of sexually transmitted infections including AIDS on adolescents :a global perspective. Retrieved Oct. 20,2006 from http//www.who.int/reproductive-health/publications/towards- adulthoood/22.pdf Marie Stopes International Worldwide. 2002. Young people, RetrievedOct.20, 2006 from http://www.mariestopes.org.uk/ww/young-people.htm . Mathews, C. et al 2006 Factors associated with teachers’ implementation of HIV\AIDS Education in secondary schools in Cape Town South Africa. AIDS Care. 18. 4: 388-397. Retrieved May 8,2007 from http://www.informaworld.com\Smpp\content_ content= a74764642_db=all. Matogo, B. W. K. 1976. The role of libraries in the environmental transformation of Africa In Library and Information Services as the instruments of transition to the 21st century in Africa: Proceedings of SCESCAL 2, Lusaka, October 4-9, Lusaka ZLA, 1978. 50-53. Maharaj, P. 2006. Reasons for condom use among young people in Kwazulu-Natal: prevention of HIV, pregnancy or both? International Family Planning Perspectives. 32.1: 28-34. Mckenzie, Bruce C. 1997. Medicine and the internet: introduction to online resources and terminology. 2nd ed. Oxford: Oxford University Press. McGuire, W. J. 1981. Behavioural medicine, public health and communication theories. Health Education. 8. Melkote, S.R., Muppidi, S.R. and Goswami, D.(2000). Social and economical factors in an integrated behavioural and societal approach to coomunications in HIV/ AIDS. Journal of Health Communication. 5, supplement. 17-28. Merry, P. 1997. Effective use of health care information. London:Bowker Saur. Meyer-weitz, Anna; Steyn, Mariana and Ghama, Sita. 1999. A situation analysis: existing information, education and communication strategies (IECS) regarding adolescent sexuality in the Piet-Relief District, Mpumalanga. Human Sciences Research Council Department of Health and Welfare, Mitchel,D.J.1994.Toward a definition of information therapy. Proceedings of Annual Symposium on Computer Application for Medical Care.71-75. Mohammadi, M. R., Mohammad, K., Farahani, F.K.A., Alikhani, S., Zare, M., Tehrani, F.R., Ramezankhani, A. And Alaeddini, F. 2006. Reproductive knowledge, attitudes and behaviour among adolescent males in Tehran, Iran. International Family Planning Perspectives 32.1: 35-44. Mukherlee, B. and Chatterjee,M. 1993. HIV risk in India and challenge towards a better future. International Conference on AIDS. 9.2, 677(abstract no PO-(08-2759), June 6-11. Musoke, M. 2005. Access and use of information by primary health care providers in rural Uganda: an interaction- value model. University of Dar es Salam Library Journal. 7.1:1-19 Narayan, Peepa Ed. 2002. Empowerment and poverty reduction: a source book. Washington: The World Bank.
69 Nare, C., Katz, K. and Tolley, E. 1997. Adolescents access to reproductive health and family planning services in Dakar (Senegal). African Journal of Reproductive Health 1.2: 15-25. Natividad, J.N. and Marquez, M. 2004. Sexual risk behaviours. Youth sex and Risk behaviours in the Phillipines. C. Raymundo and G. Cruz. Eds. Research and Development Foundation Inc. UP Population Institute. National Population Commission. 2000. Nigeria demographic and health survey 1999. Abuja: National Population Commission. Neelamegham, A. 1981. Some issues in information transfer: A Third World Perspective. IFLA Journal, 7. 1: 9. Niran, A and Iyoro, A.O. 2004 Analysis of the relationship between information gathering habit, use, attitudes and knowledge of undergraduate students towards HIV\ AIDS. International Journal of Social and Policy Issues, 2.1,2: 177-185. Njongmeta, L. N. and Ehikhamenor, F. 1998. Health information needs and services in Cameroun. African Journal of Library, Archives and Information Science, 8.1 : 13-22. Noble, J. The World's Youth 1996. Washington, DC : Population Reference Bureau, Inc. (1996). Ocansey, F.2006. Gender differences in adolescent students’ knowledge, attitudes and practices on HIV/AIDS in Ghana. Gender and Behaviour, 4.1: 568-579. Odujinrin, O. M. 1991. Sexual activity, contraceptive practice and abortion among adolescents in Lagos, Nigeria. International Journal of Gynaecology and Obstetrics, 34.4: 361-366. ------and Akinkuade, F. O. 1991. Adolescents AIDS knowledge, attitude and beliefs about preventive practices in Nigeria. European Journal of Epidemiology 7.2:127-133. Retrieved Apr. 10,2006,from http://www.ncbi.nlm.nih.gov/entrez/query.fcgizcmd=retrieve&db=pubilled&list_uids=20. Odumosu, O. 2001. Knowledge, beliefs and attitudes to HIV/AIDS in South West Nigeria. NISER Monograph series 11, 16- 17. Odusanya, O.K. and Bankole, O.M. 2006. A survey of information sources used by secondary school students in Ogun State, Nigeria for knowledge and attitudes towards HIV/AIDS. African Journal of Libraries, Archives and Information Science,16.1:53-63 Odutola, A. B. 2003. Developing countries must invest in access to information for health improvements. Journal. of Medical Internet Research 5.1: 5. Ogbuagu, S. C. and Charles, J.O. 1993. Survey of sexual networking in Calabar. Health Transition Review. Supplement to 3: 105-119. Ogunbunmi, K. 2004. How AIDS may impede Nigeria’s growth, by UNDP. The Guardian. Dec. 12:7. Ogwezzy, A. O. 2005. Access to information and its impact on knowledge, attitude and practice of contraception among in-school adolescent girls in Delta state, Nigeria. Ph.D. Thesis. University of Ibadan. Ojeda, G., Williams, T. and Vernon, R. 1990. Discussion, World Health Forum. 11:95. Okojie, S. E. 1976. Induced illegal abortions in Benin city, Nigeria. International Journal of Gynecology and Obstetrics, 14: 517-521. Okoko, E. E. 2001. Environmental and health implications of biofuel consumption on Nasarawa women. International Journal of Research in Science and Education 1.1: 121-126. Okonofua, F. E. 1995. Factors associated with adolescent pregnancy in rural Nigeria, Journal of Youth and adolescence. 24: 419-438. Okwilagwe, O. A. 1995. Bibliotherapeutic influence on Nigerian female university student: self report on sexual attitudes and behaviours. Nigerian Journal of Clinical and Counselling Psychology. 1:2, 173-186. Okwilagwe, O. A. and Vome, (2002) Bibliotherapy and value system formation by undergraduates in Nigerian University., Nigerian Journal of Applied Psychology. 7:1. Oloko, B. A. and Omoboye, A. O. 1993. Sexual networking among some Lagos state Yoruba students. Health Transition Review. Supplement to 3: 151-157,Retrieved Oct.30/2006,from http://209.85.135.104/search? qzcache:06 nnapxfumj.hte.anu.edu.au/pdfs/oloko1.pdf..
70 Olukoya, A. A. and Ferguson, J. 2002. Adolescent sexual and reproductive health and development. Archives of Ibadan Medicine 3.1: 22-27. Olukoya, A.2004. Reducing maternal mortality from unsafe abortion among adolescents in Africa. African Journal of Reproductive health, 8.1: 57-62. Omoegun, M.M. 1998 Awareness of sex- related issues among females in Lagos metropolis: implications for counseling. The Nigerian Journal of Guidance and Counselling. 6 .1,2: 79-88. Omona, Walter 2005. Health Information Systems (HIS). The internet and telemedicine in the delivery of health care in Uganda. University of Dares, Salam Library Journal. 7.1:20-31. Omu, A. E., Oronsaye, A.U., Faal, M. K. B. and Asuquo, E. E .J. 1981. Adolescent induced abortion in Benin city. Journal of Gynecology and Obstetrics. 19: 495-499. Onwuamanam, D. O. 1982. Sexual activity of school going adolescents in Nigeria. Adolescence 17.65: 81-87. Opeke, O. R. 1984. Information consciousness as a factor in organizational decision making. The case of Ogun State Ministry of Education, Ph.D. Thesis, University of Ibadan, p. 124. Oronsaye, A. U.; Ogbeide, O. and Unuigbe, E. 1982. Pregnancy among school girls in Nigeria. International Journal of Gynecology and Obstetrics. 20:409-412. Oshi, D.C; Nakalema, S. and Oshi, L.L 2005. Cultural and social aspects of HIV\AIDS in secondary schools in Nigeria. Journal of Biosocial Science. 37. 2: 175-183 Retrieved May 8,2007 from http://journals.cambridge.org\action\displayAbstract:sessionid=ABO1A7BFFF37F3FC5 Osibogun, A., Odeyemi, K. A. and Okoye, S. O. 2005. Female functional literacy for health (FFLH): Experience from the field. Nigeria Medical Practitioner, 48.4:110-115. Otive-Igbuzor, E. J. 2003. HIV/AIDS in Nigeria: rethinking women’s vulnerabilities beyond the biomedical paradigm. Nigerian Journal of Health and Biomedical Sciences, 2.1: 1-6. Otoide, V. O; Oronsaye, F; and Okonofua, F. E. 2001. Why Nigerian adolescents seek abortion rather than contraception: evidence from focus group discussions International Family Planning Perspectives, 2001, 27.2: 77-81. Planned Parenthood Federation of Nigeria. 1994. Annual report 1993. Lagos: Planned Parenthood of Nigeria. ------. 2003. Annual Report 2003. Lagos: Planned Parenthood of Nigeria. Population Reference Bureau. 1996. World Population Data Sheet. Washington, D.C.: Population Reference Bureau. ------2006. The world’s youth 2006 data sheet. Washington, DC: The Bureau 2006. Ohiri- Aniche, C. and Odukoya, D. 2004. HIV/AIDS and the education sector in Nigeria: review of policy and research documents. Retrieved May 8,2007 from http://www.rocare. org\HIV_AIDS_ education sector_ Nigeria,.pdf Queye, M., Castle, S. and Knoate, M.K. 2001. Timing of first intercourse among Malian adolescents: implications for contraceptive use. International Family Planning Perspectives 27.2: 56-62, 70. Rajam, K. 1990. Computer in health education, World Health Forum, 11.3: 311. Rani, M. Figueroa, M.E. and Ainsle, R. 2003. The Psychosocial context of young adult sexual behaviour in Nicaragua: Looking through the gender lens. International Family Planning Perspectives. 29.4: 174-181. Rommelmann, V. 2005. Cost and results of information systems for health and poverty indicators in the United Republic of Tanzania. Bulletin of World Health Organization 83.8: 569-577. Roscoe, B. and Kruger, T. L. 1990. AIDS: Late adolescents’ knowledge and its influence on sexual behaviour. Adolescence, 25.97: 39-48. Saunders, W.L. 1980 information, the unscarce resource. Presidential address delivered at the Joint Conference of the Library Association. ASLIB and the Institute of Information Scientists.Sheffield. September,1980. Shah, I. 1991. Knowledge and perceptions about AIDS among married women in Bangkok. Social Science and Medicine, 33.1, 1287-1293.
71 Shuey,D.A Babioshangire, B.B and Omiat, S. and Bagarukayo, H. 1999. Increased sexual abstinence among school adolescents as a result of school health education in Soroti districts, Uganda. Health Education Research, 14 .3: 411-419. Silayan-GO, A. 1990. Entertainment for health. World Health Forum. 1.11: 297-301. Silva, K. T. and Schensul, S. 2006. Differences in female attitudes towards premarital sex in a sample of Sri Lanka youth. Retrieved Oct. 20, 2006 from http//www.who.int/reproductive-health/publication/towards- adulthood/12.pdf Smyke, P. 1991. Women and health. London: Zed Books Ltd. Snunith, S.1998. Scholarly communication: a study of Isreali academic researchers. Journal of librarianship and information science.30.2:113-121. Stover, J. and Bravo, M. 1991. The impact of AIDS on knowledge and attitudes about condoms as a contraceptive method in Urban Mexico International Family Planning Perspectives 17.2: 61-64. Sunmola, A.M.; Dipeolu, M; Babalola, S.and Adebayo, O. D. 2003. Reproductive knowledge, sexual behaviour and contraceptive use among adolescents in Niger state of Nigeria. African Journal of Reproductive Health. 7.1: 37-48. Syke, J.R 2005. College of students’ perception of their sex education: a qualitative study. A thesis submitted to the faculty of Miami University in partial fulfillment of the requirements for the degree of Master of Social Work, Miami University Oxford. Tiamiyu, M. A. 1990. Factors underlying the use of information sources in government institutions in Nigeria. Ph.D. Thesis. University of Western Ontario. ------. 1993. The realities of developing modern information resources management systems in government organizations in developing countries with particular reference to Nigeria. Journal of Information Science. 19; 189-198. Tinker, A.; Daly, P.; Green, C.; Saxenian, H.; Lakshminarayanan, R.; and Gill, K. 1994. Women’s health and nutrition: making a difference World Bank Discussion Papers. Washington: The World Bank. Tinkham, Catherine W. and Voorhies, Eleanor F.1977. Community Healthy Nursing Evolution and Process, 2nd ed. New York: Appleton-century Croffs Tones, K. and Tilford, S. 1994. Health education: effectiveness, efficiency and equity. London: Chapman and Hall. Trigo, M.J.A.; Correia, A.M.R. and Wilson T. 1996. National information policy: the Portuguese legal framework(1980-1992). Journal of Information Science. 22 (3), 219-227. Uhegbu, A.N. 2001. The Information user: issues and themes. Enugu : John Jacobs Classic Publishers. United Nations. 2000. The world’s women 2000: Trends and Statistics. New York: United Nations. United Nations.1989. Conventions on the rights of the child. Retrieved November 23, 2007 from http://www.ohchr.org/english/law/pdf/crc.pdf United Nations Development Program. 2004. Human development report: Nigeria. Lagos: UNDP. United Nations Development Program. 1993. Young women: silence, susceptibility and the HIV epidemic. New York: United Nations Development Program UNICEF. 2001. Children’s and women’s rights in Nigeria: a wake up call, situation assessment and analysis ------. 2006. HIV/AIDS and children: prevention among young people. Retrieved Oct. 20,2006,from http://www.unicef.org/aids/index-preventionyoung. html. ------. 1997. Impact of HIV and sexual health education on the sexual behaviour of young people: A review update. UNAIDS/97, 4. Geneva: UNAIDS. UNAIDS. 1997. Women and AIDS: UNAIDS point of view (UNAIDS Best Practice Collection: Point of view). Geneva: UNAIDS. Uwalaka, E. and Matsuo, H. 2002. Impact of knowledge, attitude and beliefs about AIDS on sexual behavioural
72 change among college students in Nigeria: The case of the University of Nigeria, Nsukka. West Africa Review. Retrieved Apr.10,2006 from http://www.westafricareview.cdom/vol.3.2/uwalaka-matsuo.html. Villarruel, A. M., Jemmolt, L. S., Howard, M., Taylor, L, and Bush, E. 1998. Practice what we preach? HIV knowledge, beliefs and behaviours of adolescents and adolescent peer educators. Journal of the Association of Nurses in AIDS care, 9.5: 61-72. Weiss, E; Whelan, D; Rao Gupta, G. 1996. Vulnerability and opportunity: Adolescents and HIV/AIDS in the developing world. Washington D. C: International Center for Research on Women. Wimmer, R. D. and Diminick, J. R. 1987. Mass media research: An introduction. California: Wadsworth Company. Wilson, T. D. 1999. Models in information behaviour research. Journal of Documentation, 55, 3: 249-270 Witwer, M. 1997 In sub-Saharan Africa, levels of knowledge and use of contraceptives are involved to media exposure. International Family Planning Perspectives 23.4: 183, 184. World Health Organisation.1986. The First International Conference on Health Promotion. Held in Ohawa 7-12 November, 1986. Canadian Journal of Public Health. 77: 426-427. ------.1997. Young people and sexually transmitted diseases. Fact sheet. #186. Geneva: World Health Organization. ------2002. Adolescent friendly health services: an agenda for change. Retrieved Oct.20,2006,from http://www.who.int/child-adolescent-health/new-publications/ADH/WHO-FCH-CAH- 02-14.pdf. ------2005. “Countries need better information to receive development aid”. Bulletin of World Health Organisation, 83(8), pp. 565-566. Zimbardo, P.G., Ebbesen, E. B. and Maslath, C. 1977. Influencing attitudes and changing behaviour. Menlo Park, Calif: Addison-Wesley Publishing Co. Inc.
73