Classroom Teacher Documentation of Interventions
IDENTIFYING INFORMATION
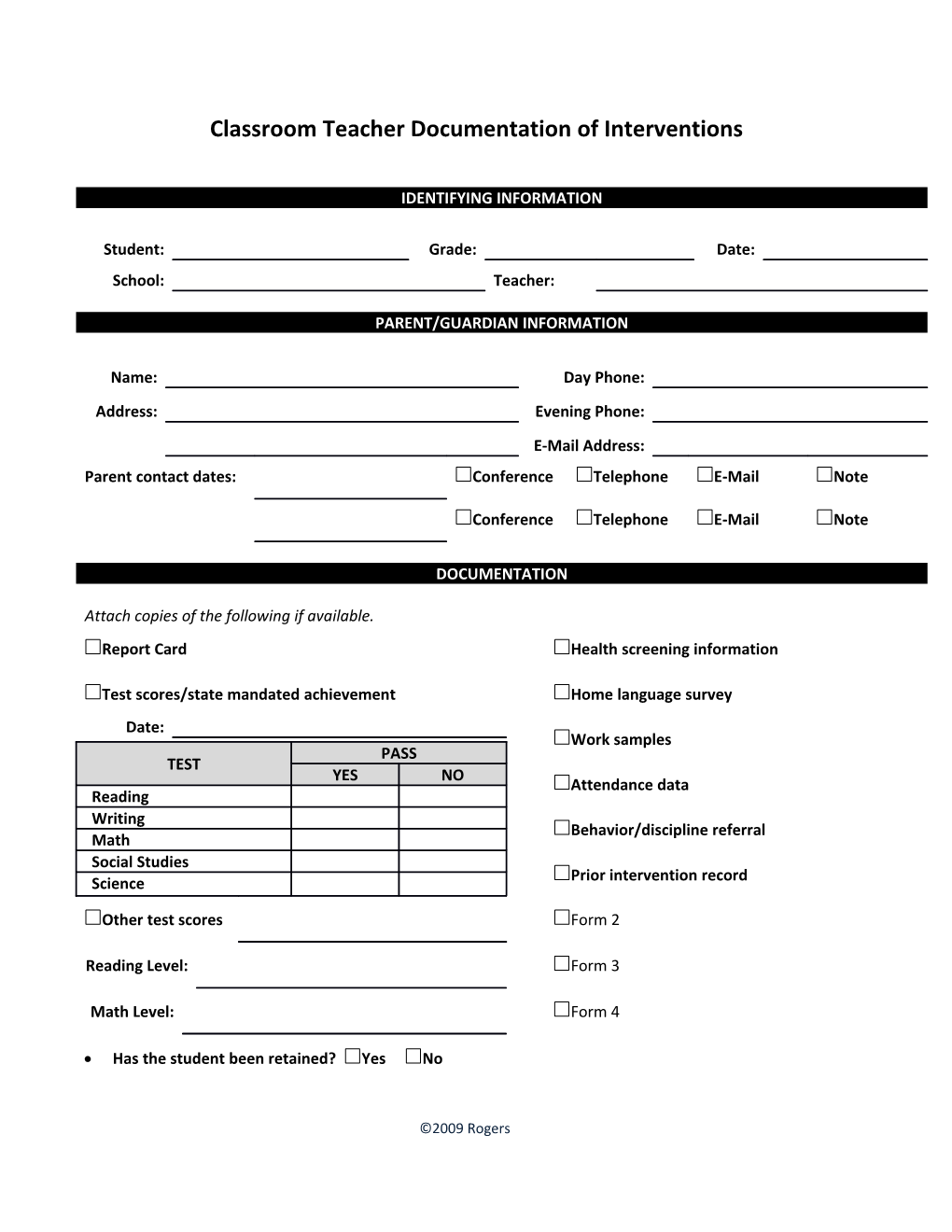
Student: Grade: Date: School: Teacher:
PARENT/GUARDIAN INFORMATION
Name: Day Phone: Address: Evening Phone: E-Mail Address: Parent contact dates: Conference Telephone E-Mail Note
Conference Telephone E-Mail Note
DOCUMENTATION
Attach copies of the following if available. Report Card Health screening information
Test scores/state mandated achievement Home language survey Date: Work samples PASS TEST YES NO Attendance data Reading Writing Behavior/discipline referral Math Social Studies Science Prior intervention record
Other test scores Form 2
Reading Level: Form 3
Math Level: Form 4
Has the student been retained? Yes No
©2009 Rogers Has the student been referred for special education assessment? Yes No
In how many prior schools has the student been educated? TIER I SUPPORT SERVICES
Academic support – regular classroom Campus interventions Re-teaching Mentoring
In-class tutorials Computer assisted instruction
Parent conference Remedial reading program ______
Differentiated instruction Remedial math program ______Other: ______Mandatory tutoring
Other: ______Title I services
Other: ______Other: ______
STATEMENT OF CONCERN
Concerns primarily related to: Academic Behavior Both
Primary reason for referral:
Describe the student’s strengths:
©2009 Rogers