EMPLOYER’S FIRST REPORT OF INJURY OR DISEASE Department of Workforce Development Worker’s Compensation Division An employer subject to the provisions of ch. 102, Wis. Stats., shall within one day after the death of 201 E. Washington Ave., Rm. C100 an employee due to a compensable injury, report the death to the Department of Workforce PO Box 7901 Development (DWD) and to the employer's insurance carrier, if insured. In cases of permanent Madison, WI 53707-7901 disability or where temporary disability results beyond the 3-day waiting period, an insured employer Imaging Server Fax: (608) 260-2503 shall also notify its insurance carrier of a compensable injury or illness within 7 days after the injury or Telephone: (608) 266-1340 beginning of a disability from occupational disease related to the employee’s compensable injury. Fax: (608) 267-0394 Insurance carriers and self-insured employers must report all compensable claims to DWD on this http://www.dwd.state.wi.us/WC form, the EDI system, or the Internet within 14 days of the date of injury. e-mail: DWDDWC@dwd,state,wi.us
The provision of your social security number is voluntary. Failure to provide it may result in information processing delay. Personal information you provide may be used for secondary purposes Privacy Law, (Please read the instructions on reverse for completing s. 15.04(1)(m). this form.)
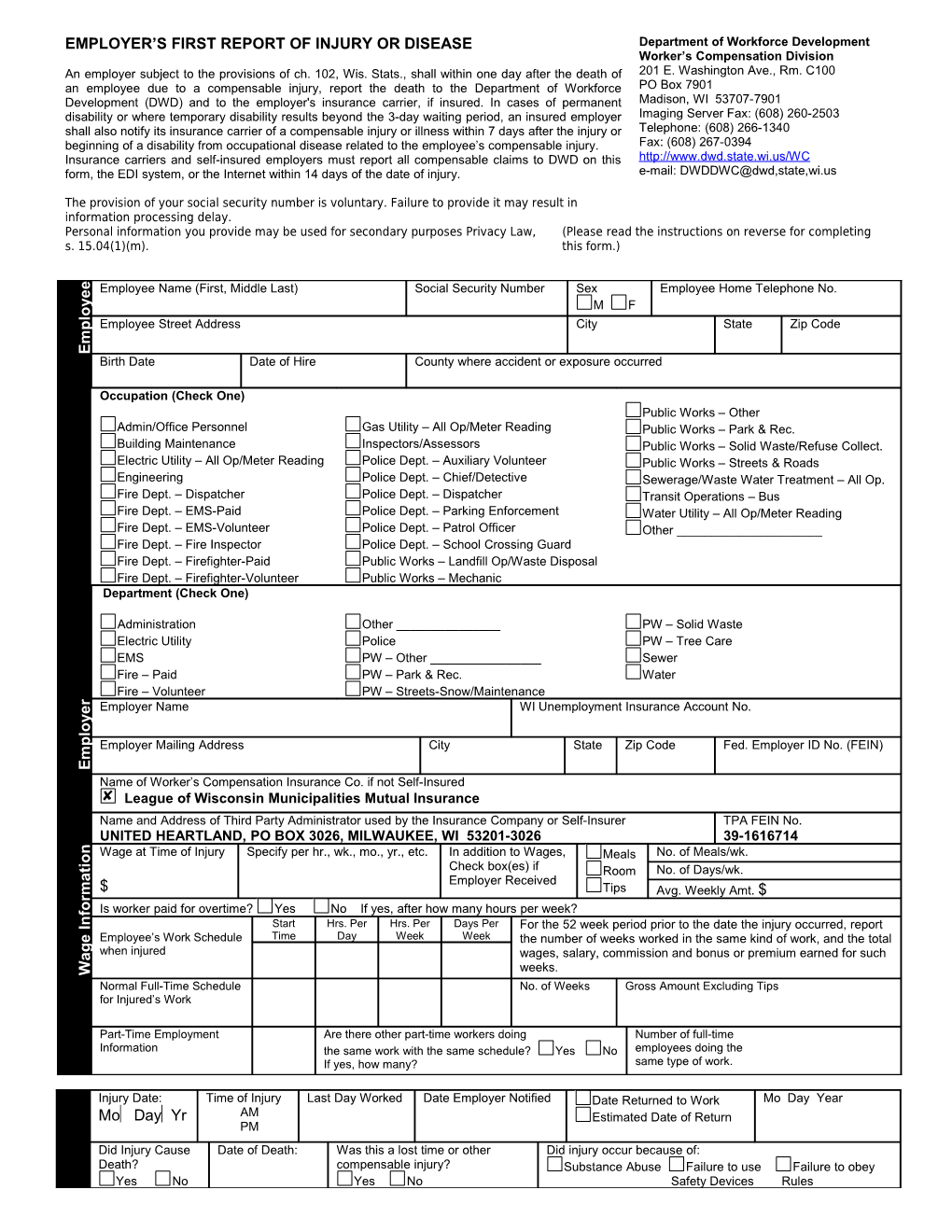
e Employee Name (First, Middle Last) Social Security Number Sex Employee Home Telephone No. e
y M F o l
p Employee Street Address City State Zip Code m E Birth Date Date of Hire County where accident or exposure occurred
Occupation (Check One) Public Works – Other Admin/Office Personnel Gas Utility – All Op/Meter Reading Public Works – Park & Rec. Building Maintenance Inspectors/Assessors Public Works – Solid Waste/Refuse Collect. Electric Utility – All Op/Meter Reading Police Dept. – Auxiliary Volunteer Public Works – Streets & Roads Engineering Police Dept. – Chief/Detective Sewerage/Waste Water Treatment – All Op. Fire Dept. – Dispatcher Police Dept. – Dispatcher Transit Operations – Bus Fire Dept. – EMS-Paid Police Dept. – Parking Enforcement Water Utility – All Op/Meter Reading Fire Dept. – EMS-Volunteer Police Dept. – Patrol Officer Other ______Fire Dept. – Fire Inspector Police Dept. – School Crossing Guard Fire Dept. – Firefighter-Paid Public Works – Landfill Op/Waste Disposal Fire Dept. – Firefighter-Volunteer Public Works – Mechanic Department (Check One)
Administration Other ______PW – Solid Waste Electric Utility Police PW – Tree Care EMS PW – Other ______Sewer Fire – Paid PW – Park & Rec. Water Fire – Volunteer PW – Streets-Snow/Maintenance r Employer Name WI Unemployment Insurance Account No. e y o l
p Employer Mailing Address City State Zip Code Fed. Employer ID No. (FEIN) m E Name of Worker’s Compensation Insurance Co. if not Self-Insured League of Wisconsin Municipalities Mutual Insurance Name and Address of Third Party Administrator used by the Insurance Company or Self-Insurer TPA FEIN No. UNITED HEARTLAND, PO BOX 3026, MILWAUKEE, WI 53201-3026 39-1616714
n Wage at Time of Injury Specify per hr., wk., mo., yr., etc. In addition to Wages, Meals No. of Meals/wk. o i t Check box(es) if Room No. of Days/wk. a Employer Received $ Tips m Avg. Weekly Amt. $ r
o Is worker paid for overtime? Yes No If yes, after how many hours per week? f
n Start Hrs. Per Hrs. Per Days Per I For the 52 week period prior to the date the injury occurred, report Time Day Week Week e Employee’s Work Schedule the number of weeks worked in the same kind of work, and the total g when injured wages, salary, commission and bonus or premium earned for such a weeks. W Normal Full-Time Schedule No. of Weeks Gross Amount Excluding Tips for Injured’s Work
Part-Time Employment Are there other part-time workers doing Number of full-time Information the same work with the same schedule? Yes No employees doing the If yes, how many? same type of work.
Injury Date: Time of Injury Last Day Worked Date Employer Notified Date Returned to Work Mo Day Year Mo DayYr AM Estimated Date of Return PM Did Injury Cause Date of Death: Was this a lost time or other Did injury occur because of: Death? compensable injury? Substance Abuse Failure to use Failure to obey Yes No Yes No Safety Devices Rules they may be reached, if additional information is needed. This form was designed to include This isneeded.wasformto information include informationdesigned if may additional reached, be they number at telephone which the and report the preparing nameperson this Provide theof the injury. caused haveetc.) may that vehicle, (i.e., ladder,tools saw, or objects the of andany burn,use etc.) concussion, fracture,injury strain, nature (i.e., the of the specific the injured, body injury,including part of of the description Section: Information Injury time atperformed of injury.jobthe being worked the for hours Section: Information Wage claim. if administrator,this for is used one party claim third the identify injury. expenses this employer for Also the responsiblefor worker’s insured compensation self- Numbercarrier for the or insurance Federal (FEIN) andEmployer Identification name Provide the injury. Section: Employer was injured.she he jobwhichwas the on Hire”employeehired isthe foror the “Date date of of employment, the dates multiple Employee Section: provided. completed. of be sections this form must the claims, administer following each of orderaccurately to In ofinjury.days work within14the date Development of Workforceemployer aresubmit to formthe Department thisclaims insured required administeringan to for carrier insurance Wis.an Stats., and s. insure102.28, under duty from to the exempt employer An Workforce Development workainjury any resulting For in worktime. not lost does involve it injurymedical anythough reporteven requiring treatment, immediately to also used be orforminsurance request this employer’scarrier administrator the claim’sthat third-party may The time. resulting in compensation lost whichor for disability temporary injury permanent related causes work-of ora insurance partyclaim the carrier administrator (7) afterdate third seven days within compensation worker’sthe employer’sform it this submitto onand sections relevant all complete must The employer ANDINSURANCE CARRIERINSTRUCTIONS EMPLOYER WKC-12 3/2002)(R.WKC-12 Injury Information Report Prepared ByReport affected) it bodyhow ofwas and affected orthe the illness?part injury(State was What cause to illness? injury(Describe occurred)this or happened how injury What involved. Description- Injury Log: OSHA from Case Number the Hospital: Address and Practitioner and Treating Name of an employeeemergency roomtreated in Was The First Report of Injury will be returned to the sender if the mandatory information is not isnot mandatory informationif sender the ofreturned to ReportInjury bethe will The First Provide all requested information to identify the injured worker’s employer at the timeworker’s injured of employerat the the to identify all information Provide requested Describe activities of employee when injury or illness occurred and what tools, machinery, objects, chemicals, etc. were chemicals, what objects, etc. were illnesstools, injuryand machinery, employee Describe activities of when oroccurred Provide all requested information to identify the injured employee. If an has If employee employee. the identifyinjured information Provide requested to all within 24 hours of the fatality of hours within 24 SEND REPORT IMMEDIATELY DO NOT WAIT FORMEDICALSEND REPORTIMMEDIATELYDONOTWAIT Provide information regarding the date and time of injury. Provide a detailedof ainjury. time and regarding Provide the information date Provide Provide the information requested regarding the the employee’swage requested injured and information regarding Provide the fatality Work Phone Number Phone Work ? ? MANDATORY INFORMATION , the employer must also submit this form directly to the Departmentof directlyto the submit form this ,the also must employer Yes No Was employee hospitalized overnight as an in-patient?as Was employee overnightan hospitalized . Position Date Signed Yes No required by OSHA on form 301. If this section is completed and retained, the employer will not have to complete the OSHA 301 form.