The BPE Probe
The BPE process:
•Mouth divided into sextants (no 8’s) represented by a single box chart for each sextant
•The probe is introduced into the gingival sulcus with a light probing pressure (25-30g)
•The probe is “walked” around the tooth starting buccally
•Only the highest score for each sextant is recorded
•0>1>2>3>4>*
An example of a completed BPE chart
3 2 X
3 2 *
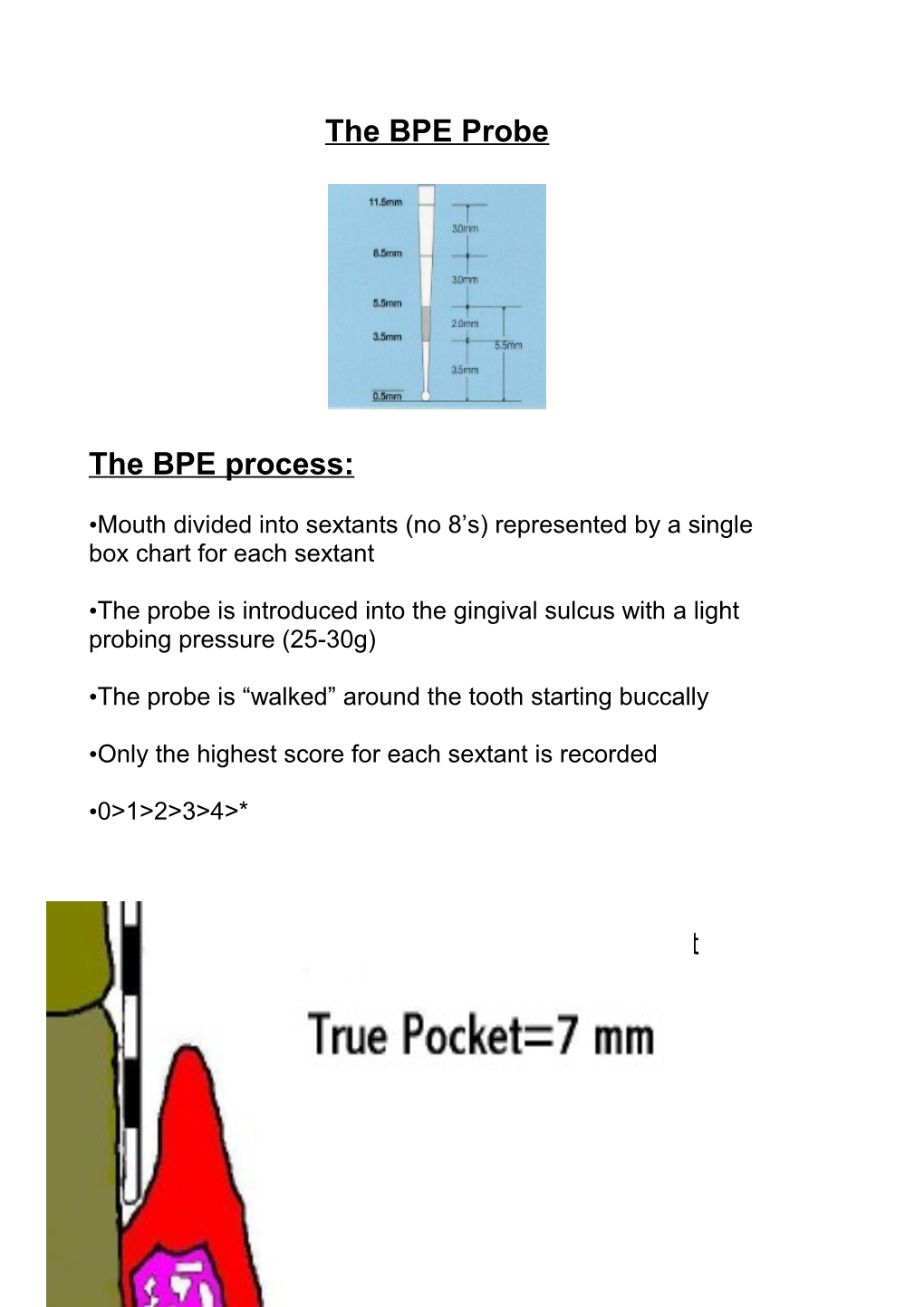
1 A true pocket has destruction of the periodontium
No destruction of periodontium in a false pocket
Code 0: Healthy gingival tissues with no bleeding on gentle probing.
2 Code 1: The coloured band on the probe remains completely visible in the deepest pocket within the sextant. There are no defective margins or calculus. There is some bleeding (within 30s) after gentle probing. Code 2: The coloured part of the probe remains visible in the deepest pocket in the sextant supra or sub-gingival calculus detected or defective margin(s) of crowns or restorations.
Code 3: Coloured part of the probe remains visible in the deepest part of the sextant.
Code 4: Coloured part of the probe disappears completely into the deepest pocket in the sextant.
Code *: Loss of attachment (recession and probing depth > 7mm OR Presence of a furcation lesion .
Management of BPE codes
3 Code 0: No treatment.
Code 1: OHI
Code 2: OHI Removal of retentive factors Screen after 1 year
Code 3: Plaque and bleeding scores pre/post Rx OHI Removal of retentive factors In code 3 sextants: probing depths for that sextant post Rx Re-record bleeding/plaque/probing depths for that sextant in year. BPE screen the remaining sextants
Code 4 or *: Plaque/bleeding charts pre Rx Full double periodontal pocket chart (recording gingival recession/shrinkage & pocket chart) OHI & removal of retentive factors Root surface debridement (RSD) Furcation treatment Re-examine, new charts Consider specialist referral
4 SUMMARY •A screening system that identifies those needing more thorough periodontal examination
•Internationally recognised
•Relatively quick and easy to carry out
•Inexpensive equipment
•Encourages examination of the periodontium in practice
•Summarises the perio status in a readily communicable form
•Gives an indication of treatment requirements
•Requires a special probe
•Lacks detail
•Not a tool to monitor disease
•Lacks information about disease activity
•Does not distinguish between true and false pockets
•Lacks information on furcation involvement
5 •Cannot be used on young individuals
6