DRUGS AND DEPRESSION: THE INCREASE IN CONSUMPTION OF DRUGS AS A SYMPTOM OF A DECREASE IN PSYCHOLOGICAL WELL- BEING
ISABELLE BERGERET, PABLO NICAISE, PHILIPPE CORTEN, VANESSA DE BACKER, AND ISIDORE PELC Laboratory of Medical Psychology, Alcohology and Drug Addiction of the 'Université Libre de Bruxelles', Belgium
1. State of the art At all times and in every society, human beings have used drugs. Each society has its own moral and legal rules giving a social meaning to the use of drugs. The function of drugs can be placed at a religious medicinal or cultural level…
The use of psychoactive substances creates levels of modified consciousness such as other practices, for instance: sex, sport, relaxation, meditation, dance, gambling, a.s… Sharing an activity that modifies consciousness reinforces the social link by a common experience in a common context. In some societies, traditionally welcoming someone could start by sharing a substance with this person; tea, coffee, peace pipe, a glass of “sake”, a betel leave… Thus, the use of drugs cannot be assimilated to sickness.
In our western modern societies, the image of chemically assisted well-being has become a model. Almost all our physical or emotional sensations can be artificially controlled or provoked with chemistry; physical appearance, physical performances, sexual desire, pain or tiredness, anxiety… So the mere fact of using drugs in order to feel better, to improve one’s performances or stop the pain has become a common attitude.
Does this mean that the use of psychoactive drugs in our modern societies has increased? Or has the expression of such habits become common? The results of the international literature on the subject diverge.
If we consider legal drugs, the regular use of tobacco seems to constantly decrease since the 70’s; from 59% to 33% of the general population; and this as well in the United States as in Northern Europe (National Drug Monitor 2002). The use of alcohol seems also to be decreasing since 1975: from 8.9 litres to 8.1 litres per person per year. (The Netherlands - National Drug Monitor). Statistics concerning drugs are not always consistent because of the illegal aspect of these substances, and/or their recent outbreak and/or their greater visibility. West European countries report either stable or falling level of heroin abuse. The number of opiate drug users in the countries of European Union is estimated to 0.4% of the population (15 years older and above) (United Nations Office for Drug Control and Crime Prevention –2000). Nevertheless, a lot of studies put forward an increase of substance consumption in some target groups of population, such as the increase of tobacco use by women, or cannabis use by youth people. The difficulty of these studies is that they emphasise
1 the problematic of specific population groups and, most of the time, it is impossible to distinguish visibility and reality of the problem. In fact, today, it is not possible to positively state that the consumption of legal or illegal drugs is increasing.
However, even if we would consider this increase as a fact, could this phenomenon be considered as a symptom of an increase of depression? It is true that a survey realised in Belgium (ISP-Louis Pasteur 1997) shows that 33% of the Belgians do express a significant state of psychological ill-being according to GHQ 12 (General Health Questionnaire-12 items) (Goldberg D 1970). According to another survey, 17% of the working people in Belgium could be considered by specialists as showing significant depressive symptoms (Ligue Belge de la Dépression & Ministère de l’Emploi et du Travail 1998). But these are transversal studies, and depressiveness or mental suffering are not depression. Depression is a specific disease, with specific symptoms and criteria. Following psychiatric criteria, recently published studies (Murphy & al. 2000 a & b), show evidences that from a strict epidemiological point of view, neither the incidence, nor prevalence of depression is in significant augmentation since 1952! The US National Epidemiological Catchment Area Study (ECA) find also that the prevalence of bipolar disorders are similar than two decade ago, but they were significant increase in lifetimes health service utilization (Judd l & Akiskal H, 2003). Once more the question to be asked is the distinction between this phenomenon and its social expression.
Considering these considerations over the supposed or real increase of drug consumption and depression, we have done the following choices:
1. We decided to take into account the common consumers on the one hand, and the addicted consumers on the other hand (see DSM-IV criteria (American Psychiatric Association 1994). In the DSM-IV, substance use disorders refers to maladaptative behaviour associated with more or less regular use of the substance. Common users are recreational or social users without maladaptative behaviour and without impairment in social functioning due to substance. 2. We chose not to use a depression scale that would only measure the suffering of the persons, and we did not chose a scale of happiness which refers to the fullness of the persons, and which is very sensitive to the immediate existing situation and to the cultural references to happiness. We decided to work with a “Quality of Life” scale, which takes into account positive and negative affects, cognitions, and which is very stable in time (Campbell & al 1976, Andrews et al 1991). 3. In this study, we take only in account illicit drugs versus control group without use of illicit drugs.
The studies ‘Quality of Life as a whole’ are focused on the subjective experience of a person (Mercier C. 1994) and the strategies to maintain this quality of life (Corten & al 1994). This subjective approach is a predictive indicator of the evolution of mental health (Barrufol & al 1995). Within the existing range of surveys on Quality of Life, the survey on aspirations and expectations has been introduced by Campbell
2 (Campbell 1976, Campbell & al. 1976, Campbell 1981). He has formulated the Quality of Life hypothesis on the basis of a double referential (Campbell & al., 1976): on the one hand on the basis of a comparison between the situation of the person and the situation of others, and, on the other hand, on the basis of a comparison between the actual situation of the person and his aspirations and/or expectations. He suggests that greater is the gap lower is the Quality of Life. Corten & al (1997a) have discussed the validity of Campbell’s and Michalos hypothesis (Michalos 1985 & 1986). Bergeret & al (1999) have demonstrated that two attitudes are possible for people who are satisfied with their quality of life. The first one is to elaborate realistic aspirations and expectations. Robbaye (1957) has demonstrated that these persons tend to be more performing. The second attitude is only encountered by aged people, and consists in hoping to maintain the same actual level of quality of life in the future.
In 1977, H. Nowlis stated that: " Drug addiction is the meeting point of a substance, a context and a personality ". This assertion has the advantage of stressing the fact that the substance alone is not the only element to be taken into account in the development of the problem: only the consumption of specific substances, in a specific context, by a specific person in a specific state of health, a specific genetic background, a specific life and past could be considered as a symptom of a larger phenomenon. This was our starting point.
2. Material and methods The constitution of samples has been made thanks to two linking parameters: the parameter of the consumed substance (no illicit drug, cannabis, amphetamines and opiates) and the parameter of the mode of consumption (common use and dependence, as defined by the DSM-IV classification). Inclusion criteria were assessed by a well trained psychologist.
Considering products and mode of consumption, seven groups would constitute a complete sample (opiate common users, opiate addicted users, amphetamine common users, amphetamine addicted users, cannabis common users, cannabis addicted users, control group). However, it is extremely rare to encounter only opiates consumers or persons addicted to cannabis.
Therefore, we created 4 groups of 40 people each: The opiate group includes dependent users of opiates (heroin or opiate substitution treatment). The DSM-IV defines dependence as a maladaptative pattern of substance use, leading to clinically significant impairment or distress (like tolerance, withdrawal,), occurring at any time in the same 12-month period. The persons of this group have been selected in a treatment centre with a " low level of exigency" ; meaning there was not necessarily under treatment at the time of the survey; The amphetamine group includes common users of amphetamines or ecstasy; The cannabis group includes common users of cannabis (no drug dependence nor drug abuse according to DSM-IV criteria);
3 The control group includes people from the general population who do not use illegal drugs.
Two exclusion criteria were applied in this research: 1) an age inferior to 25 years. For several authors, this age represents the oldest limit of adolescence. The period is marked by great changes and psychological reorganisations. Such changes can result in a psychological feeling of “ill-being” that could interfere with the results of the survey. 2) hospitalised patients in order to avoid acute co morbidity disorders. Each person of the group has answered on her own a questionnaire, the Quavisub (Subjective Quality of Life Self Assessment Questionnaire) (Corten & Mercier 1997b), which is a set of tools from which we extracted four parts.
We added to the scales described below a series of anamnestic data such as age, sex, type of studies accomplished, licit or illicit consumed substances during the last month. The four scales we kept are:
The "Satisfaction with Life Domains Scale" (SLDS) of Baker & Intagliata (1982), modified by Corten & Mercier (1989, 1994a). In this scale, the person has to evaluate his satisfaction in different fields of life (such as health, family, hobbies, work,) through pictograms representing smiling or non-smiling faces. Caron & al validated the modified SLDS. In 1997, on a Canadian population, and by Corten & Mercier in 1997b on a Belgian population. Principal Component Analysis have shown that Quality of Life was based on four dimensions: material life, affective life, social life and self-esteem (or self image). The reliability of the sub-scales has been validated by an alpha of Chronbach. Material life includes the following fields: the financial situation, the type of lodging, the neighbourhood and its facilities, and the principal activity. The affective life includes the love life the family relationships, the friends and roommates. The social life includes the free time, outer activities, principal activities, and the freedom which one has. At last, self-esteem includes physical appearance, health, self-confidence and judgement of others. The "Interdependencies Scale" of Corten & al. (1994). This scale explores the balance between the material help that one thinks he can get from others and the one he thinks he can give to others if they need it (i.e.: “on which could you count on to be lodged in case of emergency or to move an heavy object?…”). We added two items to this scale about help in the relationships that we will further deal with separately in order to maintain reliability and validity of the original scale. The "Social Anxiety Scale” of Richardson & Tasto (1976), modified and validated by Corten & al. (1997 and 2002). This scale explores different social situations that can lead to anxiety. It principally measures the impact of the social pressure on individual attitudes. The "Life Scale" or “Life ladder”of Cantril (1965), modified and validated by Corten & al. on a Belgian population (1997b and 2002). The persons have to place on a ladder from best imaginable to the worst imaginable different moments of their lives: actual life, last year’s life, the best in the past, how they imagine next year, the best thinkable situation in the future. Furthermore, they
4 have to place on this scale their estimation of the actual situation of others. Three gaps are taken into account: the actual situation versus the situation next year - called expectation -, the actual situation of the person versus the best thinkable in the future – called aspiration– and the actual situation of the person versus the actual situation of others — that is considered as self-esteem.
For reasons of shortness, authors did not maintain the followings tools of the Quavisub in this study: Importance of Life Domains scale Performance scale Objective Quality of Life questionnaire
The survey compares the four groups about their feeling of well-being and the networks of social support. The well-being is studied through the "SLDS" and "Life Scale" scales. The social links are studied by mean of the "Social Anxiety Scale" and "Interdependencies Scale". In the first part we present descriptive statistics. Then we study the psychological and social well-being in five fields of investigation: the quality of Life in general, the self-esteem, the affective and material life, and the aspirations and expectations. Then, One Way Analysis of Variance – ANOVA - on multiple comparison procedures (Bonferonni test) has been applied to compare the different dimensions of the four samples. The one way analysis of variance on multiple comparison procedure was used because each variable will be tested separately on multiple samples. Finally, clusters analyses has been performed on the four groups in order to come out with specific profiles, for example concerning the aspirations / expectations, the relations, the satisfaction… It should be possible then, to show the links between these profiles and the group to which they belong.
All results are analysed with SPPS9 software for Windows.
3. Results 3.1. Descriptive statistics
The Opiate group has a mean of 29.45 years old with standard deviation of 4.8 years. It is composed of 75% male and 25% female. The Amphetamine and derived group has a mean of 28.48 years old with standard deviation of 2.25 years. It is composed of 35% male and 65% female. The Cannabis group has a mean of 28.1 years old with standard deviation of 2.8 years. It is composed of 55% male and 45% female. The Control group has a mean of 32.5 years old with standard deviation of 5.2 years. It is composed of 35% male and 65% female.
Univariate analysis of variance conducted with ‘groups’ as independent variable and (1) SLDS, (2) Interdependencies Scale, and (3) Life Scale as dependent variables revealed neither significant main effects nor interactions involving level of education of participant, age or gender. Consequently, all subsequent analysis collapsed across this factor.
5 Table 1: Substances used last month (%)
Opiate (N=40) Cannabis (N=40) Amphetamines and Controls (N=40) derived (N=40) o k o k o k o k y h y h y h y h t t t t e e e e a a a a % n n n n n n n n e e e e d d d d o o o o w w w w m m m m tobacco 7.5 90.0 2.5 0 25.0 52.5 22.5 0 2.5 97.5 0 0 55 45 0 0 alcohol 17.5 42.5 32.5 7.5 17.5 25 40.0 17.5 10.0 27.5 45.0 17.5 15 12.5 40.0 32.5 heroin 22.5 40.0 20.0 17.5 100.0 0 0 0 100.0 0 0 0 100.0 0 0 0 methadone 62.5 30.0 7.5 0 100.0 0 0 0 100.0 0 0 0 100.0 0 0 0 cocaine 72.5 10.0 12.5 5 100.0 0 0 0 45.0 0 10 45.0 100.0 0 0 0 cannabis 67.5 22.5 5.0 5.0 0 52.5 42.5 5.0 65.0 35.0 0 0 100.0 0 0 0 amphetamine. 100.0 0 0 0 100.0 0 0 0 20.0 7.5 40.0 32.5 100.0 0 0 0 ecstasy 92.5 7.5 0 0 87.5 0 0 12.5 5.0 0 37.5 57.5 100.0 0 0 0 antidepressor. 85.0 15.0 0 0 97.5 2.5 0 0 100.0 0 0 0 100.0 0 0 0 benzodiazepines. 67.5 20.0 12.5 100.0 0 0 0 97.5 0 0 2.5 87.5 0 12.5 0
6 The group of addicted to opiates is characterised by a high frequency of simultaneous consumption of other substances (65%) whether they are licit (35%) or not (42.5%) (the use of legal substances and/or illicit substances could be cumulative). More than a fourth combine this consumption with cocaine, a third uses cannabis and only 7,5% use daily ecstasy. A third regularly takes anxiolytics and 15% antidepressive drugs. It is also the group where we find the most consumers of alcohol on a daily basis and, together with the group of amphetamine users, the most regular tobacco smokers. It is important to point out that 22,5% of the persons who did not use heroine this last month, were under substitution treatment of methadone.
Half of the persons of the group of cannabis users do use cannabis daily. 12,5% of them use exceptionally ecstasy (once a month). Their use of alcohol and tobacco is close to the one of the control group.
Most of amphetamine and ecstasy users are not daily users what is in accordance with the inclusion criteria of this group, which is, by definition, a recreative group. Almost half of the group uses cocaine from time to time, and a third daily uses cannabis. We point out that nearly all the persons of this group are daily smokers of tobacco.
Then, by definition the control group uses no illicit drug. Some of them use anxiolytics, but none of them daily. Their alcohol consumption is close to the one of the Belgian population (see Health Survey Louis Pasteur) but the tobacco consumption is higher (45% versus 30% in the Health Survey on the Belgian population). There are fewer smokers in the control group than in the opiate and amphetamine user groups and they drink alcohol less frequently.
3.2. Investigation about the Quality of Life
The Quality of Life measures in a balanced way, on one hand the ill-being of the persons, but also the subjective dimension of the well-being, and on the other hand, the judgement that these persons have on these dimensions. In this chapter we will first globally approach and then specifically focus on self- esteem, material situation, socio-relational situation, en at last aspirations / expectations. Here, we will only take into account the significant results at the threshold of p= 0.05.
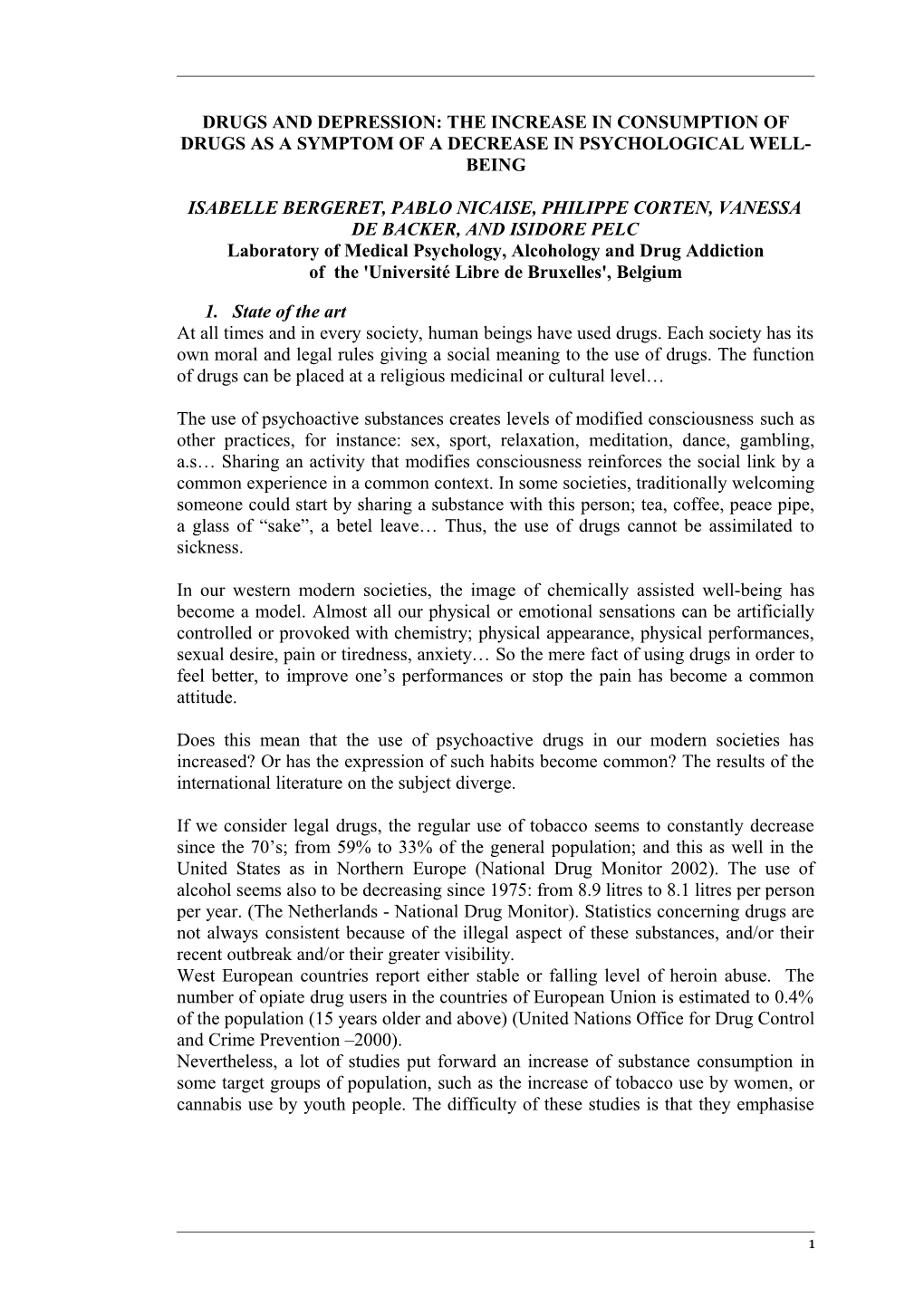
a. Quality of Life in general The SLDS measures four distinct dimensions: self-esteem, affective life, social life and material life. Figure 1 stresses two elements: on the one hand that the consumers of cannabis or amphetamines and its derivates have a similar profile to the controls and judge their quality of life as good or fairly good. (>= 4). On the other hand, the persons addicted to opiates have a quality of life that they judge rather bad (except self-esteem). Their profile is also significantly different of than the three other groups in the Bonferonni test.
7 Quality of Life
7
g 6 n i e b - l l e 5 W
4
f e e e
m f f f o
i i i
e
L L L
y e
t
t l l i l
e s a a
i i a v
E i r e c t u
f e i f
o l c t Q
L
3 e e S a
l f
a S f M g b A o n l i
G Opiate e b -
l 2 Cannabis l I Amphetamines Controls 1
Figure 1 : Quality of Life
b. Self-esteem Self-esteem can be analysed through the SLDS dimensions on the one hand, and the Cantril’s Life Scale. The SLDS : Self-esteem is the only dimension to be experienced as satisfactory by the four groups. For the group of addicted to opiates it is the best score even if, the mean of the group in the Bonferonni test is significantly lower than the three other groups and characterised by a great spread of the results. This dimension includes satisfaction with one’s physical image, health, self-confidence and judgement of others. If we apply the Bonferonni test to each of the variables included in the self- esteem subscale, the group addicted to opiates will again show less satisfaction with each of the items except for self-confidence where there is no significant difference between the four groups.
The Life Scale: The Life Scale measures the gap between the vision one has of it’s own actual life and the actual life of others in general. In this case, the group of amphetamine users and its derivates (ecstasy) distinguishes itself from the other groups in the Bonferonni test by estimating their actual situation much more enviable than the actual situation of others.
c. Material Life Here again, the group dependant to opiates diverges significantly to the three other groups by showing less satisfaction, globally and with specific items included in
8 this dimension. Furthermore, the persons of this group are particularly dissatisfied with their lodging, their neighbourhood and it’s facilities.
d. The social and relational situation The social and relational situation can be approached (1) by the SLDS that measures two dimensions: the satisfaction with the affective life and the satisfaction with the social life, (2) by the scale of interdependencies (3) and by the scale of social anxiety. The SLDS: The dimensions themselves as well as the items they include give significantly less satisfaction to the group dependent to opiates, which seems to get less satisfaction from its affective and social life. Concerning the items, we also notice that in this survey the Bonferonni test does not show differences between the control group and the group dependant to opiates about their love life. Both groups seem significantly dissatisfied compared to the group of cannabis users and the group of amphetamine users. Furthermore, concerning the outer activities, the group using amphetamines and its derivate shows more satisfaction than the control group. The scale of interdependencies: here again, the dimensions as well as the items taken separately, the group dependent to opiates shows less people to rely on (an average of 50% has no one or almost no one to count on for help), and have less people counting on them (30% see no one or almost no one). On the other hand 95% of the control group, 87.5% of the amphetamine users and its derivates and 82.5% of the cannabis users can count on several people to help them in a series of material problems. To confide one’s personal problems to, the three groups show less people than the control group able to count on several persons to help them, but 95% are sure that several persons can count on them. . About the different services they could ask for, the cannabis users imagine more different services than the group dependant to opiates. The control group, the group of amphetamines users and the group dependent to opiates show no significant differences on this point.
If we look closer on whom they can count on, we first see friends, and family; once more the group dependent to opiates have little or no friends. (Bonferonni test significant at p= 0.05 versus the others groups). Concerning the help to the family, no significant difference between the groups appears. On the other hand, concerning the help received, the cannabis users believe to receive more help than the amphetamine users. The group dependent to opiates receive less help than the three other groups. The neighbours seem less concerned in this survey, particularly in the group of amphetamine users and the group dependent to opiates. At last, the roommates have a marginal role. Regrettably, we do not have enough data on cohabiting people. The scale of social anxiety: Here, we found no significant difference between the four groups. This means that globally the social anxiety is similar in each group. The control group though tends to be more sensitive to remarks and criticism than the group dependant to opiates, and the cannabis users are less at ease than the control group when they feel they are not liked.
e. Aspirations-Expectations
9 The group dependent to opiates perceive their actual situation, the situation next year and the best they can expect less positive than the three other groups. On the other hand, this group has the largest gap between his expectations (next year – actual life) and its aspirations (better life in the future – actual life)(Bonferonni). As mentioned in the introduction, these gaps are related with the quality of life. There is no significant difference between the three other groups.
3.3. Cluster analysis
Cluster analysis allow to take all subjects or variable, no matter the group they are included in, and to put forward clusters over the sample groups. The method is based on the Euclidian distance (distance between each group and distance between each subject inside one specific group). Cluster analysis are computed on the SLDS, interdependencies scale, and life scale.
The “Satisfaction with Life Domains Scale –SLDS” shows 3 clusters. The first cluster is characterised by a good level of satisfaction in all life domains. This cluster is composed with 72.5% of amphetamines and derived users, 72.5% of cannabis users, 65% control and 17.5% opiate dependent. The second cluster is characterised by a low level of satisfaction in all life domains. It is composed with 35% of opiate dependent and 5% amphetamine and derived users. The third cluster is characterised by a rather good level of satisfaction in material conditions of life (food, accommodation), and a low level of satisfaction in social relationship (family and love relations, other's judgement) and leisure activities. This cluster is compound with 47.5% of opiate dependent, 35% control, 27.5% of cannabis users and 22,5% of amphetamine users.
The “Interdependencies Scale” also shows 3 clusters. The first cluster is characterised by subjects involved in extended social relationship (they may rely on others and others may rely on them towards different situations of life). Moreover, these subjects know about professionals to help them. This cluster is composed with 67.5% of cannabis users, 60% of amphetamine and derived users, 47.5% control and 27.5% opiate dependent. The second cluster is also involved in extended social relationship (they may rely on others and others may rely on them towards different situations of life). But these subjects would not ask professionals to help them. It is composed with 47.5% control, 35% of amphetamine and derived users, 32.5% of cannabis users, and 25% opiate dependent. The third cluster is characterised by subjects with low social relationship. It is composed with 47.5% of opiate dependent, 5% control, and 5% of amphetamine and derived users.
At last, “Life Scale” shows 4 clusters. The first cluster is characterised by a good actual life, good situation in the past, and better expectations for close and remote future. They have a good opinion about other's situation, but their own actual situation is higher. This cluster is composed with 87.5% of control, 75% of cannabis users, 72.5% of amphetamine and derived users, and 10% of opiate dependent.
10 The second cluster has a similar profile, except that these subjects have a bad opinion about last year situation. This group is composed with 35% of opiate dependent, 15% of amphetamine and derived users, 12.5% of cannabis users and 12.5% of control. The third cluster is characterised by a lower opinion on actual situation than on last year situation. Others situation is also estimated better than theirs. They have great expectations for close and remote future. This cluster is composed with 35% of opiate dependent, 12.5% of cannabis users, and 12.5% of amphetamine and derived users. At last, the fourth cluster has a similar profile, but actual situation is even worse than in the third cluster, while last year situation was better than in the third cluster. Thus, there is a quite big distance between their best in the past situation and their actual life. Their aspirations and expectations are very high. This cluster is composed with 20% of the opiate dependent.
4. Discussion
Our hypothesis was that the consumption of drugs alone could not account for a social ill-being, and that we should take into account a group of other elements among which we could mention, for example: consumption contexts, specific personality of the consumers, their respective background and genetic inheritance, health and various co-occurrences.
On the one hand, the groups of common amphetamine and cannabis users have statistically a similar behaviour than the control group. These three groups show a good socialisation: numerous affective and social relationships, and a similar answer to social pressure. We do not notice an erosion of the social link in these groups, in spite of drug use for two of them. Moreover, these three groups consider their subjective Quality of Life as good or fairly good for each dimension used: self-esteem, affective life, social relations, and material life. We notice no phenomenon of ill-being within the members of these groups. At last, the relative aspirations / expectations of these three groups are also similar. The cannabis and amphetamine users seem to have a good socialisation level and a subjective Quality of Life situated on the well-being side. It also seems that their drug consumption does not represent a problem for them, nor a fortiori a symptom of a larger social phenomenon.
On the other hand, the group dependant to opiates significantly diverges from the three other groups, with the weakest results : their subjective Quality of Life refers more to "ill-being" –except for what concerns self-esteem– , their interdependencies and social relationships are weak, their aspirations / expectations are low with a very negative perception of their actual situation. Besides, the opiates dependent group is not homogenous. We notice among the group : 17,5% with a good subjective Quality of Life, 27,5% with high interdependencies, 30% with a positive perception of their actual situation and relatively similar aspirations / expectations than the control group. Thus, ill-being and erosion of the social link are not even ineluctable among opiate dependent individuals. It would be interesting in a further survey, to closely outline the characteristics of this group keeping good parameters of social functioning.
11 Numerous objections could be expressed concerning this preliminary study. The choice of the substances taken in to account for the group of consumers and the addicted group is not insignificant : the fact that we could not find for each type of use consumers of each substance, the fact that the size of the sample groups remained limited, the role of alcohol, a.s. Nevertheless, our survey allows us to show that the consumption of drugs cannot in anyway be considered as the sole indicator of a phenomenon of ill-being, or a factor of erosion of the social link. If we stick to the elements taken into account in our selection criteria, the difference between a common use on the one hand, and abuse or dependence on the other hand seems statistically significant.
It could then be fruitful, in another study, to constitute groups of users according to these diagnoses, focusing on the modes of consumption instead of the substance used. Our clinical experience suggests, for example, that groups of addicted alcoholics could show similarities with a group addicted to opiates. Also, the context of consumption could be significant in these cases. We could, for example, take into account, the social differences between the domestic alcohol consumers (at home), and the alcohol consumers outside their home (bars…). Finally, according to our selection criteria, it could be interesting to consider more closely the states of modified consciousness that people aim at and take into account their psychological and social status, namely in relation to boredom, self-esteem and social links.
12 Bibliography
AMERICAN PSYCHIATRIC ASSOCIATION (1994) Diagnostic and Statistical Manual of Mental Disorders Fourth Edition. Washington DC, Publ. A.P.A.,
ANDREWS F. M., & ROBINSON J. P. (1991). « Measures of Subjective Well- Being ». In J. P. ROBINSON,P. R. SHAVER, & L. S. WRIGHTSMAN (Eds.), Measures of Personality & Social Psychological Attitudes. Volume 1 of Measures of Social Psychology Attitudes. San Diego Ca, Academic Press, 61-115.
BAKER F., & INTAGLIATA J. (1982). « Quality of Life in the Evaluation of Community Support Systems. » Evaluation & Program Planning, vol 5, n°1, 69 :78.
BARRUFOL E, GISLE L, CORTEN P. (1995) « Life Satisfaction as mediator between distresssing events and neurotic impairment in a général population. » Acta psychiatrisa Scandinavica vol 92 , 56 :62
BERGERET I, CORTEN PH, SYLIN M, MERCIER C. (1999) Quality of life, expectations and aspirations. Oral presentation in the « Congress: Genome and environment » International Federation of Psychiatric Epidemiology. Taiwan - 6-9 mars
CAMPBELL A. (1976) Subjective Measures of Well-Being. American Psychologist vol 31, 117 :124.
CAMPBELL A., CONVERSE PE., RODGERS WL. (1976) The Quality of American Life. Perceptions, Evaluations and Satisfactions. CAMPBELL A, CONVERSE PE, RODGERS WL. (Eds) New-York, Russel Sage Foundation.
CAMPBELL A, (1981) The Sense of Well-Being in America. Recent Patterns and Trends . CAMPBELL A (Eds) . New-York, NY, McGraw Hill,:253.
CANTRIL, H. (1965). The Pattern of Human Concerns. In CANTRIL (Eds) New Brunswick, New Jersey, Rutgers University Press.
CARON J, MERCIER C, TEMPIER R. (1997) « Une validation québecquoise du Satisfaction with Life Domains. » Santé Mentale au Quebec vol 22, n°2, 195 :217
CORTEN PH, MERCIER C, PELC I. (1994a) « Subjective Quality of Life. Clinical Model for Assessment of Rehabilitation Treatment in Psychiatry. » Social Psychiatry & Psychiatric Epidemiology vol 29, 178 :183.
CORTEN PH, BERGERET I, HACHEY R, MERCIER C. (1997a) « Expectation, aspirations and Quality of Life » in CORTEN Ph & MERCIER C. (Eds) International Report NATO Collaborative Research Grant n° 910084 ‘Pattern of Quality of Life among People with Disabilities’ Brussels
CORTEN PH, MERCIER C. (1997b) « Subjective Quality of Life Assesssment. The Quavisub : content, validity, utility. » in CORTEN Ph & MERCIER C. (Eds)
13 International Report NATO Collaborative Research Grant n° 910084 ‘Pattern of Quality of Life among People with Disabilities’ Brussels
CORTEN PH, BERGERET I, FROM L, MERCIER C, PELC I (2002) « Are Psychiatric Patients Good Probands for Subjective Assessment of the Quality of life? » (In process)
FACY F. (1995) « Abords épidémiologiques de la toxicomanies: morbidité et évaluation des soins, » La revue du praticien, vol 45, 1345 :1350
GOLDBERG, D. L., COOPER, B., EASTWOOD, M. R., ET AL (1970) "A Standardised Psychiatric Interview Suitable for Use in Community Surveys". British Journal and Social Medicine., 24, 18-23.
INSTITUT SCIENTIFIQUE DE SANTÉ PUBLIQUE LOUIS PASTEUR (1997) Enquête Santé de la Population Belge. Brussels
JUDD L.L. & AKISKAL H.S. (2003) « The prevalence and disability of bipolar spectrum disorders in the US population : Re-analysis of the ECA database taking into account subthreshold cases » Jouranal of Affective Disorders, vol73, n° 1-2 , 123 :131
KAPLAN H.J. (1985) « Testing a general theory of drug abuse and other deviant adaptation », Journal of Drug Issues, vol 15 : 477 :492
KAPLAN H.J., MARTIN S.S., JOHNSON R.J., ROBBINS C.A. (1986) « Escalation of marijuana use : Application of a général theory of deviant behavior », Journal of Health and Social Beahavior, vol 27 : 44 :61
LAQUEILLE X., URIBÉ M., OLIÉ J-P. (1995) « Clinical aspects of drug addiction », La revue du praticien, vol 45 : 1359 :1363
LIGUE BELGE DE LA DÉPRESSION & MINISTÈRE FÉDÉRAL DE L’EMPLOI ET TRAVAIL (1998) Dépressivité et monde du travail , Brussels, 14 pp
MERCIER C, CORTEN PH. (1989). « Qualitry of Life iand Social Rehabilitation: Canadian and belgian surveys with Severely Mentally Ill. » In: A.P.A eds. Syllabus of 41st Institute on Hospital and Community Psychiatry. Washington D.C. American Psychiatric Association, 62 :63
MERCIER C. (1994) « La Méthodologie de l’évaluation de la qualité de vie subjective. » In TERRA J-L (Eds) Qualité de Vie Subjective et Santé Mentale.. Paris Ellipses, 92 :110
MICHALOS AC. (1985) « Multiple Discrepancies Theory. » Social Indicators Research. Vol 16, 347 :413.
MICHALOS A. (1986) « An Application of Multiple Dicrepencies Theory to Senior. » Social Indicators Research, vol 18, 349 :374.
14 MURPHY J.M., LAIRD N.M., MONSON R.R., SOBOL A.M., LEIGHTON A.H. (2000a) « Incidence of depression in the Stirling County Stundy : Historical and comparative perspectives ». Psychosociological Medecine, vol 303, n°3, 505 :514
MURPHY J.M., LAIRD N.M., MONSON R.R., SOBOL A.M., LEIGHTON A.H. (2000b) « A 40 years perspective on the prevalence of depression : The Stirling County Study. » Archives of général Psychiatry. Vol 57, n°3, 209 :215
NATIONAL DRUG MONITOR (2001)
NATIONAL DRUG MONITOR (2001)
NATIONAL DRUG MONITOR (2001)
NOWLIS H. (1977) « The epidemiology of drug abuse : current issues. Interpretations and policy implications. » NIDA research monography, vol 10 , 244 :247
Richardson, F. C., & Tasto, D. L. (1976). « Development and Factors Analysis of a Social Anxiety Inventory. » Behavior Therapy, vol 7, 453 :462.
Robaye F, (1957). Niveaux d'aspiration et d'expectation. In ROBAYE F. (Eds) Paris Presses Universitaires de France (PUF)
Schifano F. Potential human neurotoxicity of MDMA : subjective self-reports, evidence from an Italian drug addiction centre and clinical case studies, Neuropsychobiology ; 2000 ; 42 :25-33
Solal J-F., Schneider, M-C. (1996) « Drug addiction and social exclusion. » La revue du praticien, vol 46, 1854 :1860
United Nations Office for Drug Control and Crime Prevention (2000) World Srug Report.
Velea D., Hautefeuille M., Vazeille G. Lantran-Davoux C. Nouvelles drogues synthétiques empathogènes, L’encéphale, 1999 ; XXV :508-514
15 ISABELLE BERGERET, PABLO NICAISE Laboratoire de Psychologie Médicale, d’alcoologie et de toxicomanie ULB, 4 place Van Gehuchten, 1020 Bruxelles Belgique, [email protected], 322.4772701
Isabelle Bergeret, a psychologist, and Pablo Nicaise, a sociologist and a political scientist, both work at the Research Laboratory of Medical Psychology, Alcohology and Drug Addiction of the Université Libre de Bruxelles, Belgium, in research on drug addiction. Isabelle Bergeret was also involved in the “Drug Cell” of the Belgian Ministry of Public Health. Their research interests are : treatment of drug addiction, care and patient’s needs, policy and addiction.
PHILIPPE CORTEN, Laboratoire de Psychologie Médicale, d’alcoologie et de toxicomanie ULB, 4 place Van Gehuchten, 1020 Bruxelles Belgique, [email protected], 322.4772701
Philippe Corten is a neuropsychiatrist, associated professor at the Laboratory of Medical Psychology, Alcohology and Drug Addiction and Professor at the Health Public School of the Univesité Libre de Bruxelles. He is specialized in Stress and Quality of Life researchs. Previously, he was also visiting professor at the McGill University Montreal and the State University of Portland Oregon, and until recently psychiatric advisor at the Ministry of Social Welfare, Public Health and Environment of Belgium.
VANESSA DE BACKER, Laboratoire de Psychologie Médicale, d’alcoologie et de toxicomanie ULB, 4 place Van Gehuchten, 1020 Bruxelles Belgique, 322.4772701
Vanessa De Backer is a psychologist at Brugmann Hospital, Brussels, Belgium. She does clinical work with drug addicts.
ISIDORE PELC Laboratoire de Psychologie Médicale, d’alcoologie et de toxicomanie ULB, 4 place Van Gehuchten, 1020 Bruxelles Belgique, [email protected], 322.4772701
Isidore Pelc is a neuropsychiatrist, (MD, PhD), head of the Department of Psychiatry and Medical Psychology at the Teaching Brugmann Hospital, Director of the Laboratory of Medical Psychology, Alcohology and Drug Addiction of The Université Libre de Bruxelles, Belgium.
KEYWORDS: Drug addiction, Cannabis, Opiate, Amphetamine, Quality of Life
16