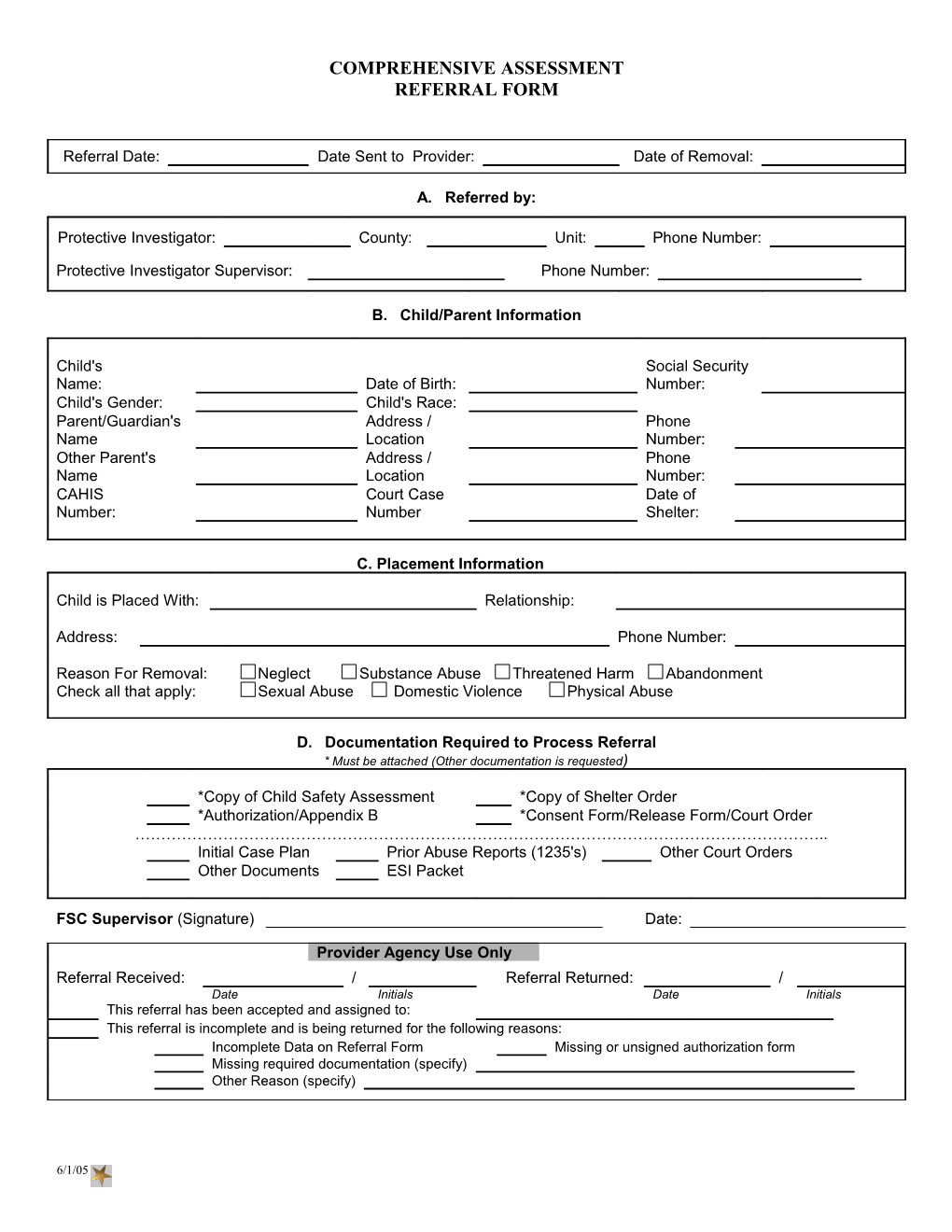
COMPREHENSIVE ASSESSMENT REFERRAL FORM
Referral Date: Date Sent to Provider: Date of Removal:
A. Referred by:
Protective Investigator: County: Unit: Phone Number:
Protective Investigator Supervisor: Phone Number:
B. Child/Parent Information
Child's Social Security Name: Date of Birth: Number: Child's Gender: Child's Race: Parent/Guardian's Address / Phone Name Location Number: Other Parent's Address / Phone Name Location Number: CAHIS Court Case Date of Number: Number Shelter:
C. Placement Information
Child is Placed With: Relationship:
Address: Phone Number:
Reason For Removal: Neglect Substance Abuse Threatened Harm Abandonment Check all that apply: Sexual Abuse Domestic Violence Physical Abuse
D. Documentation Required to Process Referral * Must be attached (Other documentation is requested)
*Copy of Child Safety Assessment *Copy of Shelter Order *Authorization/Appendix B *Consent Form/Release Form/Court Order …………………………………………………………………………………………………………………….. Initial Case Plan Prior Abuse Reports (1235's) Other Court Orders Other Documents ESI Packet
FSC Supervisor (Signature) Date:
Provider Agency Use Only Referral Received: / Referral Returned: / Date Initials Date Initials This referral has been accepted and assigned to: This referral is incomplete and is being returned for the following reasons: Incomplete Data on Referral Form Missing or unsigned authorization form Missing required documentation (specify) Other Reason (specify)
6/1/05 APPENDIX B
AUTHORIZATION FOR COMPREHENSIVE BEHAVIORAL HEALTH ASSESSMENT
This is to certify that
Child's Name Date
Medicaid Number
has been screened and determined to be in need of a Comprehensive Behavioral Health Assessment (H00031 HA) as Outlined in the Medicaid Community Mental Health Services Coverage and Limitations Handbook. The comprehensive behavioral health assessment will be provide by
(provider)
District SAMH Representative Date
AND
District Family Safety Program Office Representative Date
OR
Juvenile Justice Representative Date
AUTHORIZATION FOR COMPREHENSIVE BEHAVIORAL HEALTH ASSESSMENT FOR CHILD IN SHELTER
This is to certify that
Child's Name Date of Referral
Medicaid Number Shelter Name
Shelter Address
Has been screened and determined to be in need of a Comprehensive Behavioral Health Assessment (H0031 HA) as outlined in Medicaid Community Mental Health Coverage and Limitations handbook. The behavioral health comprehensive assessment will be provided by
(provider)
District Family Safety Representative Date
To be placed in recipients (child's medical record
6/1/05