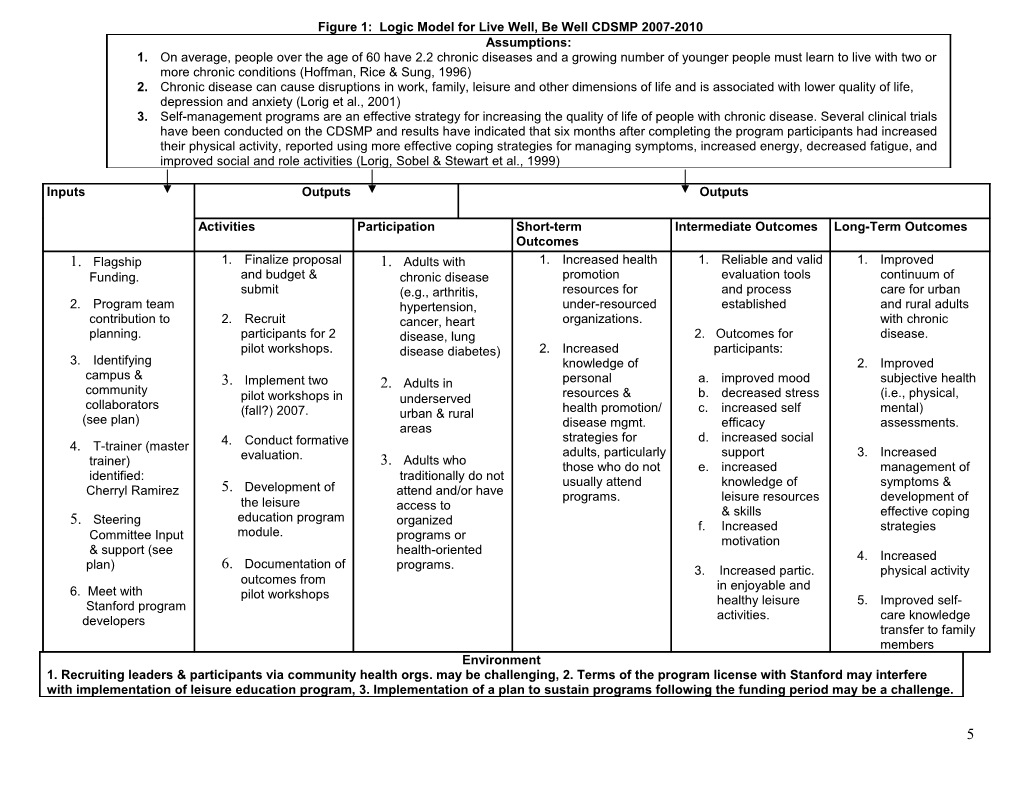
Figure 1: Logic Model for Live Well, Be Well CDSMP 2007-2010 Assumptions: 1. On average, people over the age of 60 have 2.2 chronic diseases and a growing number of younger people must learn to live with two or more chronic conditions (Hoffman, Rice & Sung, 1996) 2. Chronic disease can cause disruptions in work, family, leisure and other dimensions of life and is associated with lower quality of life, depression and anxiety (Lorig et al., 2001) 3. Self-management programs are an effective strategy for increasing the quality of life of people with chronic disease. Several clinical trials have been conducted on the CDSMP and results have indicated that six months after completing the program participants had increased their physical activity, reported using more effective coping strategies for managing symptoms, increased energy, decreased fatigue, and improved social and role activities (Lorig, Sobel & Stewart et al., 1999)
Inputs Outputs Outputs
Activities Participation Short-term Intermediate Outcomes Long-Term Outcomes Outcomes 1. Flagship 1. Finalize proposal 1. Adults with 1. Increased health 1. Reliable and valid 1. Improved Funding. and budget & chronic disease promotion evaluation tools continuum of submit (e.g., arthritis, resources for and process care for urban 2. Program team hypertension, under-resourced established and rural adults contribution to 2. Recruit cancer, heart organizations. with chronic planning. participants for 2 disease, lung 2. Outcomes for disease. pilot workshops. disease diabetes) 2. Increased participants: 3. Identifying knowledge of 2. Improved campus & 3. Implement two Adults in personal a. improved mood subjective health community 2. pilot workshops in underserved resources & b. decreased stress (i.e., physical, collaborators (fall?) 2007. health promotion/ c. increased self mental) (see plan) urban & rural areas disease mgmt. efficacy assessments. 4. Conduct formative strategies for d. increased social 4. T-trainer (master adults, particularly support 3. Increased evaluation. Adults who trainer) 3. those who do not e. increased management of identified: traditionally do not usually attend knowledge of symptoms & Cherryl Ramirez 5. Development of attend and/or have the leisure programs. leisure resources development of access to & skills effective coping 5. Steering education program organized module. f. Increased strategies Committee Input programs or motivation & support (see health-oriented 4. Increased Documentation of plan) 6. programs. 3. Increased partic. physical activity outcomes from in enjoyable and 6. Meet with pilot workshops Stanford program healthy leisure 5. Improved self- developers activities. care knowledge transfer to family members Environment 1. Recruiting leaders & participants via community health orgs. may be challenging, 2. Terms of the program license with Stanford may interfere with implementation of leisure education program, 3. Implementation of a plan to sustain programs following the funding period may be a challenge.
5