1 Adult Residential Licensing – Resident Assessment-Support Plan (RASP) For compliance with 55 Pa.Code §§ 2600.225-227
Instructions for Use
The Preadmission Screening process provides only a “sketch” of a resident’s needs, enough to make a decision about admission but not enough to develop a plan of care. Timely and accurate assessment of a resident’s needs is essential to ensure that the admitting home is aware of all of a resident’s medical, personal care, behavioral health, and psychosocial needs. The regulations allow 15 days for the assessment process to allow sufficient time for homes to become acquainted with the resident’s overall status and develop an accurate assessment.
Once the assessment is completed, the assessment results are used to create a support plan, which is simply the home’s plan to meet the needs identified through the assessment. The regulations allow 30 days for the completion of the support plan to ensure that there is sufficient time to create a high-quality and effective plan.
The assessment and support plan are inseparably linked; one will never be created without the other. As such, they are both contained on this single document, the Resident Assessment- Support Plan, or RASP. The left side of the document is the assessment; the right side of the document is the support plan. The RASP has been designed to easily match the resident’s needs with the plan to meet those needs; simply move the assessed need on the left to the plan to meet the need on the right.
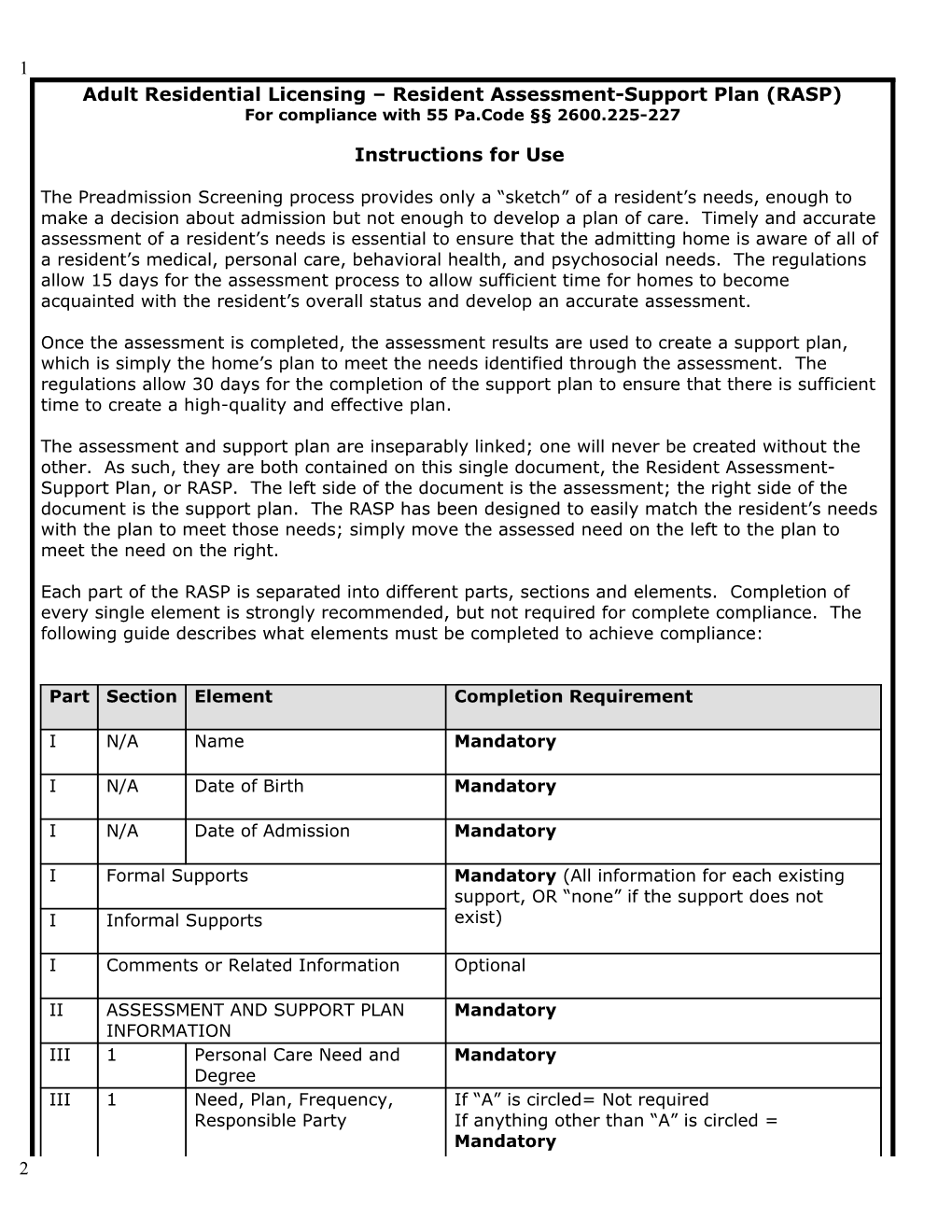
Each part of the RASP is separated into different parts, sections and elements. Completion of every single element is strongly recommended, but not required for complete compliance. The following guide describes what elements must be completed to achieve compliance:
Part Section Element Completion Requirement
I N/A Name Mandatory
I N/A Date of Birth Mandatory
I N/A Date of Admission Mandatory
I Formal Supports Mandatory (All information for each existing support, OR “none” if the support does not I Informal Supports exist)
I Comments or Related Information Optional
II ASSESSMENT AND SUPPORT PLAN Mandatory INFORMATION III 1 Personal Care Need and Mandatory Degree III 1 Need, Plan, Frequency, If “A” is circled= Not required Responsible Party If anything other than “A” is circled = Mandatory 2 1
3 4 Adult Residential Licensing – Resident Assessment and Support Plan For compliance with 55 Pa.Code §§ 2600.225-227
PART I: RESIDENT INFORMATION
Name: Formal Supports Informal Supports (Family, Friends, etc.) Support Name Telephone Number Name Relationship Telephone Number
Primary Physician Designated Person
Date of Birth: Dentist
Case Manager
Date of Admission: Other (specify):
Other (specify):
Comments or related information:
PART II: ASSESSMENT AND SUPPORT PLAN INFORMATION
Date of Reason for Reason for Support Date Assessment Finalized: Admission: Assessment: Plan: Finalization Timeframes: Initial Initial Initial – Within 15 days of admission Date of Last Annual – Within 380 days (1 year plus 15-day grace period) after most recent assessment Assessment: Annual Annual Significant Change – Within 5 calendar days of significant change Department Request – Within 24 hours of request Significant Change* Significant Change* Date Support Plan Finalized: Department Request Department Request Date of Last Finalization Timeframes: Support Plan: Initial – Within 30 days of admission Annual – Within 30 days of completion of the annual assessment Significant Change – Within 5 calendar days of new assessment Department Request – Within 24 hours of new assessment *If the assessment and support plan were completed due to a significant change, please include a description of the change:
2
5 DPW – ARL – RASP Page 1 of 11 6 PART III: ASSESSMENT AND SUPPORT PLAN INFORMATION
The left side of the document is the assessment. The assessment is used to determine what the resident’s needs are. The right side of the document is the support plan. Each resident’s support plan is based on the results of the assessment. The support plan is used to record how the resident’s needs will be met. Complete the assessment portion first, and then use the results to create a support plan. Attach additional pages as necessary. Section 1: Personal Care Needs, Supervision, Mobility, and Medications
Assessment: Support Plan - Personal Care Needs Personal Care Needs Description of Service Need - Specify exactly what service or services are needed to meet the need. Example: Resident cannot lift eating utensils to mouth due to complications from Parkinson’s Disease. Degree Codes A = Independent Plan to Meet Service Need - Specify what will be done to make sure the service need is met. B = Prompting/Cueing Example: Staff will feed the resident during mealtimes. C = Some Physical Assistance D = Total Physical Assistance Frequency - Specify how often the plan will be enacted using one of the choices. Example: Other: At all mealtimes. E = Not Applicable Responsible Party - Specify who will perform the plan using one of the choices. Example: DCS Responsible Party Codes: DCS = Direct-Care Staff on Duty F = Family Member CM = Case Manager N/A = Not Applicable (Degree Code A Only) O = Other (Specify):
3 Personal Care Need and Degree Description of Service Need Plan to Meet Service Need Frequency Responsible Party
Eating Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance with eating, such as feeding the Hourly Other F O: resident or encouraging the resident to eat Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Drinking Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance with fluid intake, such as raising Hourly Other F O: a glass to the resident’s mouth Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Transferring in/out of bed/chair Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assisting the resident to rise from or sit/lie Hourly Other F O: on a bed or chair Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Toileting Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance with hygienic practices Hourly Other F O: surrounding toilet use Degree (Circle One): Daily CM (Specify): A B C D E Weekly
7 DPW – ARL – RASP Page 2 of 11 8 Personal Care Need and Degree Description of Service Need Plan to Meet Service Need Frequency Responsible Party
Bladder management Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance with urinary incontinence-related Hourly Other F O: problems Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Bowel management Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance with fecal incontinence-related Hourly Other F O: problems Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Ambulating Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance moving from one place to Hourly Other F O: another Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Personal hygiene Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance with overall personal hygiene, Hourly Other F O: such as hair and nail care Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Managing health care Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance with overall healthcare Hourly Other F O: coordination, such as tracking different doctors’ appointments and medications Daily CM (Specify): Degree (Circle One): Weekly A B C D E
Securing health care Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance with locating a health care Hourly Other F O: provider for a specific need Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Turning and positioning in bed/chair Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance with moving a resident while in a Hourly Other F O: bed or chair Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Doing laundry Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Self-explanatory Hourly Other F O: Degree (Circle One): A B C D E Daily CM (Specify): Weekly
Shopping Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Self-explanatory Hourly Other F O: Degree (Circle One): A B C D E Daily CM (Specify): Weekly
9 DPW – ARL – RASP Page 3 of 11 10 Personal Care Need and Degree Description of Service Need Plan to Meet Service Need Frequency Responsible Party
Securing and using transportation Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance with locating a transportation Hourly Other F O: source and with use of the source Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Managing finances Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Self-explanatory Hourly Other F O: Degree (Circle One): A B C D E Daily CM (Specify): Weekly
Using the telephone Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance locating or dialing telephone Hourly Other F O: numbers Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Making and keeping appointments Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance with scheduling appointments, Hourly Other F O: tracking appointments, and arranging for transportation to appointments Daily CM (Specify): Degree (Circle One): Weekly A B C D E
Caring for personal possessions Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Self-explanatory Hourly Other F O: Degree (Circle One): A B C D E Daily CM (Specify): Weekly
Writing correspondence Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance with writing personal and Hourly Other F O: business-related letters and emails Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Engaging in social and leisure activities Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance with identifying and participating Hourly Other F O: in available activities Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Using a prosthetic device Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Assistance attaching, removing, or cleaning Hourly Other F O: a prosthetic device Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Obtaining clean, seasonal clothing Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Self-explanatory Hourly Other F O: Degree (Circle One): A B C D E Daily CM (Specify): Weekly
4 11 DPW – ARL – RASP Page 4 of 11 12 Assessment – Supervision Support Plan – Supervision None Description of Supervision Needs Plan to Meet Supervision Needs Responsible Resident requires no supervision either in the home or when in the Party community DCS Minimal F Resident requires no supervision in the home or when in familiar CM surroundings, but needs attendance in unfamiliar places N/A O: Moderate Resident requires some supervision in the home and needs attendance when outside the home, and/or tends to wander
Extensive Resident requires regular supervision in the home and cannot leave home unattended; unaware of unsafe areas Total Resident requires 24-hour direct supervision Assessment – Mobility Support Plan – Mobility Description of Mobility Needs Plan to Meet Mobility Needs Responsible Independent (Mobile) Party Resident has no mobility needs and can evacuate independently in an emergency DCS F Minimal (Mobile) CM Resident requires limited physical or oral assistance to evacuate in an N/A emergency O:
Moderate (Immobile) Resident requires moderate physical or oral assistance to evacuate in an emergency
Total (Immobile) Resident requires total physical or oral assistance to evacuate in an emergency from one or more staff persons
Assessment – Medications Support Plan – Medications Resident can self-administer without assistance Description of Medication Needs Plan to Meet Medication Needs Responsible Party OR DCS Resident can self-administer with (check all that apply)… F …assistance in remembering schedule CM …assistance in offering medications at prescribed times N/A …assistance in opening container or locked storage area O:
OR
Resident cannot self-administer medications
13 DPW – ARL – RASP Page 5 of 11 14 Section 2: Medical, Dental, Dietary, and Sensory Needs
Assessment: Support Plan – Medical Needs Medical Needs Plan to Meet Medical Need - Specify what will be done to make sure the need is met. Example: Staff will measure resident’s blood pressure. Medical Diagnoses – Physical Using the Documentation of Medical Frequency - Specify how often the plan will be enacted using one of the choices. Example: Daily Evaluation Form from the most recent medical evaluation, list all of the resident’s Responsible Party - Specify who will perform the plan using one of the choices. Example: DCS physical diagnoses. Example: Hypertension Responsible Party Codes: DCS = Direct-Care Staff on Duty F = Family Member CM = Case Manager N/A = Not Applicable (Degree Code A Only) O = Other (Specify):
5 Medical Diagnoses – Physical Plan to Meet Medical Need Frequency Responsible Party
N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly
N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly
N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly
N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly
N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly
N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly
15 DPW – ARL – RASP Page 6 of 11 16 Medical Diagnoses – Physical Plan to Meet Medical Need Frequency Responsible Party
N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly
N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly
6
7 Assessment: Support Plan – Dental, Dietary, and Support Needs Dental Plan to Meet Need Specify what will be done to make sure the resident’s dental, dietary, and sensory needs are addressed. Diagnoses or Needs Examples: Resident will see dentist, resident will have special diet, resident will see ophthalmologist List all of the resident’s dental, dietary, and sensory needs Frequency - Specify how often the plan will be enacted using one of the choices. Example: Monthly Examples: Impacted tooth Responsible Party - Specify who will perform the plan using one of the choices. Example: CM Mechanical soft foods Cataracts Responsible Party Codes: DCS = Direct-Care Staff on Duty F = Family Member CM = Case Manager N/A = Not Applicable (Degree Code A Only) O = Other (Specify): Dental Need Plan to Meet Dental Need Frequency Responsible Party
N/A Monthly DCS N/A Hourly Other F O: Daily CM (Specify): Weekly
N/A Monthly DCS N/A Hourly Other F O: Daily CM (Specify): Weekly
Dietary Need Plan to Meet Dietary Need Frequency Responsible Party
N/A Monthly DCS N/A Hourly Other F O: Daily CM (Specify): Weekly
N/A Monthly DCS N/A Hourly Other F O: Daily CM (Specify): Weekly
Sensory Need Plan to Meet Sensory Need Frequency Responsible Party
17 DPW – ARL – RASP Page 7 of 11 18 Assessment: Support Plan – Dental, Dietary, and Support Needs Dental Plan to Meet Need Specify what will be done to make sure the resident’s dental, dietary, and sensory needs are addressed. Diagnoses or Needs Examples: Resident will see dentist, resident will have special diet, resident will see ophthalmologist List all of the resident’s dental, dietary, and sensory needs Frequency - Specify how often the plan will be enacted using one of the choices. Example: Monthly Examples: Impacted tooth Responsible Party - Specify who will perform the plan using one of the choices. Example: CM Mechanical soft foods Cataracts Responsible Party Codes: DCS = Direct-Care Staff on Duty F = Family Member CM = Case Manager N/A = Not Applicable (Degree Code A Only) O = Other (Specify): Dental Need Plan to Meet Dental Need Frequency Responsible Party
Vision N/A Monthly DCS N/A Hourly Other F O: Daily CM (Specify): Weekly
Hearing N/A Monthly DCS N/A Hourly Other F O: Daily CM (Specify): Weekly
Communication N/A Monthly DCS N/A Hourly Other F O: Daily CM (Specify): Weekly
Olfactory (smell) N/A Monthly DCS N/A Hourly Other F O: Daily CM (Specify): Weekly
Tactile (touch) N/A Monthly DCS N/A Hourly Other F O: Daily CM (Specify): Weekly 8
Section 3: Mental Health, Behavioral Health, and Cognitive Functioning Needs
Assessment: Support Plan – Mental Health Needs Mental Health Needs Plan to Meet Mental Health Need - Specify what will be done to make sure the need is met. Example: Resident will see therapist Medical Diagnoses – Psychological Frequency - Specify how often the plan will be enacted using one of the choices. Example: Weekly Using the Documentation of Medical Evaluation Form from the most recent Responsible Party - Specify who will perform the plan using one of the choices. Example: CM medical evaluation, list all of the resident’s diagnoses. Responsible Party Codes: Example: Schizophrenia DCS = Direct-Care Staff on Duty F = Family Member CM = Case Manager N/A = Not Applicable (Degree Code A Only) O = Other (Specify):
19 DPW – ARL – RASP Page 8 of 11 20 Section 3: Mental Health, Behavioral Health, and Cognitive Functioning Needs
Medical Diagnoses – Psychological Plan to Meet Psychological Need Frequency Responsible Party
N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly
21 DPW – ARL – RASP Page 9 of 11 22 9
Assessment: Support Plan - Behavioral or Cognitive Care Needs Behavioral or Cognitive Need Description of Service Need - Specify exactly what service or services are needed to meet the need. Example: Resident is upset by loud noises due to PTSD. Degree Codes A = No problem Plan to Meet Service Need - Specify what will be done to make sure the service need is met. B = Minimal Problem Example: Staff will sit with resident when loud noises occur. C = Moderate Problem D = Severe Problem Frequency - Specify how often the plan will be enacted using one of the choices. Example: Other: As needed E = Not Applicable Responsible Party - Specify who will perform the plan using one of the choices. Example: DCS Responsible Party Codes: DCS = Direct-Care Staff on Duty F = Family Member CM = Case Manager N/A = Not Applicable (Degree Code A Only) O = Other (Specify):
10 Behavioral or Cognitive Description of Service Need Plan to Meet Service Need Frequency Responsible Party Need and Degree
Orientation to time, place, and person Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Resident does not know when, where, or Hourly Other F O: who he is Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Irritability Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Resident is easily upset Hourly Other F O: Degree (Circle One): A B C D E Daily CM (Specify): Weekly
Judgment Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Resident’s decisions are harmful to self or Hourly Other F O: others Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Agitation Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Resident is easily upset or unsettled Hourly Other F O: Degree (Circle One): A B C D E Daily CM (Specify): Weekly
Aggression Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Resident is violent, verbally or physically Hourly Other F O: Degree (Circle One): A B C D E Daily CM (Specify): Weekly
Hallucinations Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Resident hears or sees things that are not Hourly Other F O: there Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Communication of needs Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Resident cannot express needs or desires Hourly Other F O: Degree (Circle One): A B C D E Daily CM (Specify): Weekly
23 DPW – ARL – RASP Page 10 of 11 24 Behavioral or Cognitive Description of Service Need Plan to Meet Service Need Frequency Responsible Party Need and Degree
Understanding instructions Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Resident cannot understand instructions or Hourly Other F O: directions Degree (Circle One): Daily CM (Specify): A B C D E Weekly
Short-Term memory Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Resident is unable to retain small amounts Hourly Other F O: of information in mind in an active, readily- available state for a limited period time Daily CM (Specify): Degree (Circle One): Weekly A B C D E
Long-Term memory Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A Resident is unable to store information in Hourly Other F O: mind for a long period of time to be recalled at a later date Daily CM (Specify): Degree (Circle One): Weekly A B C D E
Ability to use and avoid poisonous Not Applicable (Code A Only) Not Applicable (Code A Only) N/A Monthly DCS N/A materials Hourly Other F O: Resident is unable to safely use and avoid poisonous materials Daily CM (Specify): Degree (Circle One): Weekly A B C D E
11 Section 4: Social and Recreational Needs Assessment: Support Plan - Social and Recreational Needs Social and Recreational Needs Plan to Meet Service Need - Specify what will be done to make sure the residents’ social/recreational needs are addressed. Example: Resident will be offered mystery novels to read. List all of the resident’s social and recreational needs in each section. Frequency - Specify how often the plan will be enacted using one of the choices. Example: Other: As needed
Responsible Party - Specify who will perform the plan using one of the choices. Example: DCS Responsible Party Codes: DCS = Direct-Care Staff on Duty F = Family Member CM = Case Manager N/A = Not Applicable (Degree Code A Only) O = Other (Specify): Social and Recreational Need Plan to Meet Social and Recreational Need Frequency Responsible Party
The resident’s hobbies/interests include: N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly The resident enjoys the following solitary N/A Monthly DCS N/A activities: Hourly Other F O: Daily (Specify): CM Weekly The resident enjoys the following group N/A Monthly DCS N/A activities: Hourly Other F O: Daily (Specify): CM Weekly
25 DPW – ARL – RASP Page 11 of 11 26 The resident’s religious affiliation, if any, is: N/A Monthly DCS N/A Hourly Other F O: Daily (Specify): CM Weekly The resident does not participate in solitary or N/A Monthly DCS N/A group activities because: Hourly Other F O: Daily (Specify): CM Weekly 12
PART III: SUMMARY AND DETERMINATION
Summary of Resident’s Overall Wellness (include significant changes identified through the assessment process, comments for improving quality of care, or other relevant information not capture above):
Determination – By signing below, I certify that… I am the home’s administrator, a staff person authorized to complete these documents, or a human services agency representative The information on this assessment is accurate and was developed based on records and/or interviews The above-named resident’s needs may be met in this personal care home by following the support plan Assessor’s Printed Name: Assessor’s Title / Agency:
Assessor’s Signature: Date Signed:
PART IV: PARTICIPATION By signing below, the signature verifies that s/he participated in the assessment and/or support plan process
Name Relationship to Resident Signature Date Copy of Document Copy Provided? Signed Requested? Yes Yes No Self OR No N/A Unable to participate Refused to sign Declined to participate Unable to sign Yes Yes No OR (check one) No N/A Refused to sign Unable to sign
27 DPW – ARL – RASP Page 12 of 11 28 Yes Yes OR (check one) No Refused to sign Unable to sign No N/A Yes Yes No OR (check one) No N/A Refused to sign Unable to sign 13
29 DPW – ARL – RASP Page 13 of 11 30