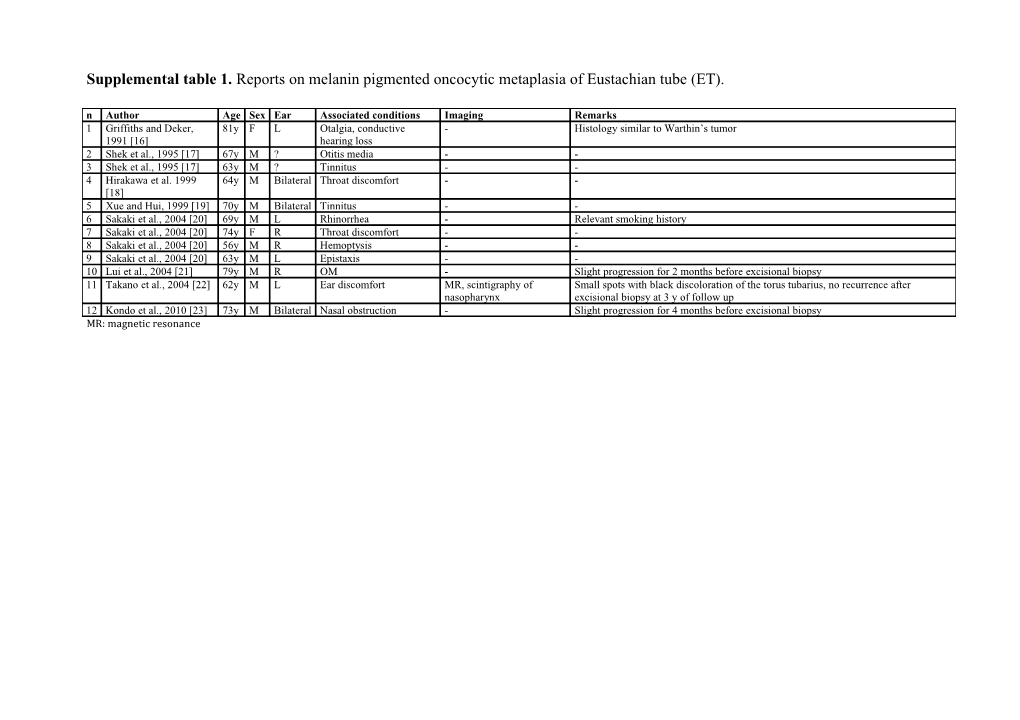
Supplemental table 1. Reports on melanin pigmented oncocytic metaplasia of Eustachian tube (ET). n Author Age Sex Ear Associated conditions Imaging Remarks 1 Griffiths and Deker, 81y F L Otalgia, conductive - Histology similar to Warthin’s tumor 1991 [16] hearing loss 2 Shek et al., 1995 [17] 67y M ? Otitis media - - 3 Shek et al., 1995 [17] 63y M ? Tinnitus - - 4 Hirakawa et al. 1999 64y M Bilateral Throat discomfort - - [18] 5 Xue and Hui, 1999 [19] 70y M Bilateral Tinnitus - - 6 Sakaki et al., 2004 [20] 69y M L Rhinorrhea - Relevant smoking history 7 Sakaki et al., 2004 [20] 74y F R Throat discomfort - - 8 Sakaki et al., 2004 [20] 56y M R Hemoptysis - - 9 Sakaki et al., 2004 [20] 63y M L Epistaxis - - 10 Lui et al., 2004 [21] 79y M R OM - Slight progression for 2 months before excisional biopsy 11 Takano et al., 2004 [22] 62y M L Ear discomfort MR, scintigraphy of Small spots with black discoloration of the torus tubarius, no recurrence after nasopharynx excisional biopsy at 3 y of follow up 12 Kondo et al., 2010 [23] 73y M Bilateral Nasal obstruction - Slight progression for 4 months before excisional biopsy MR: magnetic resonance Supplemental table 2. Reports on Eustachian tube (ET) teratomas and dermoids (or “hairy polyps”).
Author Age° Sex Ear Presentation Imaging Origin Micro Remarks First surgery Definitive surgery Recurrence (Follow up) 1 Henke, 1924 8m F R Discharging ear No Anterior wall, near mesoderm, Tympanic membrane and Removal attempt from the Radical tympanomastoidectomy ? (?) [24] nasopharyngeal ectoderm ossicles not recognizable external ear ostium, widened ET 2 Navratil, 8y F L Discharging ear X-Ray Anterior mesoderm, Antero-inferior tympanic - Antromastoidectomy Atticoantrotomy, middle ear and no (3y), small 1965 [25] hypotympanum, ectoderm membrane perforation, - Adenotomy and ear polyp pharyngeal combined approach, residual widened ET ossicles intact removal skin free flap to cover the lower tympanic half tube perforation 3 Pirodda, 22y F L Discharging ear X-ray ET inferior and mesoderm. Large perforation of - Tympanomastoidectomy Re-exploration, careful No (2m) 1965 [26] infero-lateral walls, ectoderm inferior and part of - Revision enlargement of the tympanic widened ET with superior quadrants of the tympanomastoidectomy ostium of the tubal bony canal normal tympanic membrane and piecemeal removal of the nasopharyngeal mass ostium 4 Eichel et 28m F L Discharging ear X-ray ET walls mesoderm, Small tympanic membrane - Adenoidectomy and left Re-exploration and one piece No (4m) Hallberg, ectoderm, perforation, erosion of the myringotomy mass removal 1966 [27] entoderm long process of the incus, - Anterior drum polyp stapes and facial nerve removal intact but covered with - Complete cortical granulation tissue, mastoidectomy and mastoid associated congenital cleft cavity obliteration of the posterior left ear lobule 5 Münker, 7y F L Middle ear X-ray ET,widened ET mesoderm, Incudostapedial joint -Adenoidectomy and left Middle ear revision and through No (1y) 1972 [28] effusion ectoderm erosion ventilation tube insertion nasopharynx one piece mass - Left mastoidectomy removal 6 Karduck et 6y F L Discharging ear X-ray ET isthmus mesoderm, Subtotal perforation of the Adenotonsillectomy Transmeatal one piece mass ? (?) Schulz, 1973 ectoderm tympanic membrane removal [29]
7 Desnos et 10d, M L Discharging ear, No ET and iuxta-tubal mesoderm, Central perforation of the Early transoral removal Tympanoplasty through ? (?) Martin, 1974 14* life threating nasopharynx ectoderm tympanic membrane, endoaural approach [30] upper airway ossicles dislocation, obstruction stenosis of the nasopharyngeal ostium, autosomic dominant genetic deafness 8 Arcand et 10m F L Discharging ear CT, MR, from protympanum mesoderm, Anterior petrous bone and - Polyp removal Modified radical mastoidectomy No (2y), Abela, 1985 and CA to cartilagineous ET ectoderm ET cartilages destroyed, - Exploration of mastoid and through retro- and pro-tympanic residual ET [31] few posterolateral compression middle ear through retro- combined approach with dysfunction weeks and bony erosion of carotid tympanic approach, biopsy condylar subluxation artery 9 Nicklaus et 6m M R Discharging ear, CT nasopharyngeal mesoderm, no - Adenoidectomy and bilateral Transoral removal No (?) al., 1991 upper airway orifice, widened ET ectoderm ventilation tube insertion [32] obstruction - Needle aspiration (to exclude blood or cerebrospinal fluid) 10 Vrabec et 14m F L Discharging ear CT, MR antero-inferior mesoderm, Extensive granulation - Bilateral ventilation tube Excision of the tumor through No (?) Schwaber, hypotympanum, ectoderm tissue surrounding the insertion the middle ear 1992 [33] widened osseous ET ossicles - Exploratory tympanotomy and biopsy 1 Boedts et al., 18m F L Chronic otitis X-ray, along ET, mesoderm, Malleus and incus partly Large mastoidectomy with Revision type III tympanoplasty No (10y) 1 1992 [34] media CT downwards just on ectoderm destroyed partial removal with careful dissection along ET top of tonsillar lodge
12 Forrest et al., 8m F L Discharging ear CT lateral aspect of the mesoderm, Ossicles displaced, Modified radical Transoral removal No (4m) 1993 [35] carotid artery with a ectoderm, associated with antral mastoidectomy, partial pedicle attached to entoderm cholesteatoma removal causing slipping the upper pole of the through ET and life threating left tonsil, widened tracheal obstruction ET 13 Kolias et al., 12m F L Middle ear CT, MR hypotympanum and mesoderm, Parapharyngeal extension - Bilateral ventilation tube Retro-tympanic tympanoytomy ? (?) 1995 [36] effusion ET, widened osseous ectoderm (under the digastric insertion approach and modified neck ET muscle) and flattening of - Exploratory tympanotomy dissection carotid canal through retro-tympanic approach 14 Kolias et al., 17m ? L Recurrent otitis CT, MR ET, widened ET mesoderm, Parapharyngeal extension, - Tympanoplasty with partial Retro-tympanic tympanotomy ? (?) 1995 [36] media ectoderm incudostapedial joint mass removal approach with simultaneous erosion, in contact with fiberoptic nasopharyngoscopy carotid artery open exploration of the neck and of the parapharyngeal space 15 Morisseau- Birth F R Life threating MR ET nasopharyngeal mesoderm, Thickened middle ear Early partial removal “au ras” Endoaural tympanotomy and No (21m of Durand et upper airway ostium ectoderm mucosa, Rosenmüller fossa from ET nasopharyngeal complete removal at 13m age) al., 1996 obstruction at dysmorphism ostium [37] birth, recurrent otitis media 16 Ruah et al., 4m F R Discharging ear CT medial aspect of ET mesoderm, Tympanic membrane - Miringotomy Exploratory tympanotomy and ? (?) 1999 [38] opening, widened ET ectoderm perforation - Biopsy mass removal through endoaural approach 17 Sichel et al., 30m F L Discharging ear CT, MR ET, widened ectoderm Incudostapedial - Negative middle ear biopsy Modified radical mastoidectomy No (6m) 1999 [39] protympanum discontinuity with infratemporal fossa exposure 18 Gourin et 21m M L Middle ear CT along ET, widened mesoderm, Erosion of the - Left ventilation tube Anterior canaloplasty and open No (3y) Sofferman, effusion protympanum ectoderm, hypotympanum and of the insertion tympanomastoidectomy, 1999 [40] entoderm lower portion of the incus - Right miringotomy piecemeal removal
19 Wasinwong 7d F L Middle ear CT Posterolateral wall of mesoderm, No No Combined transnasal and No (1y) et al. 2003 effusion nasopharyngeal ectoderm, transoral approach [41] ostium, protrusion in entoderm the pharynx 20 Roh, 2004 7m F L Sleep apnea, CT Medial wall of mesoderm, No No Transoral endoscopic removal CR (15m) [42] bloody vomiting nasopharyngeal ectoderm ostium 21 Baek et al. 2y F L Discharging ear CT, MR ET mesoderm, ? ? ? ?(?) 2005 [43] ectoderm 22 Walker, 6m F L Middle ear CT, MR Lower third of mesoderm, Left pre-auricolar sinus, No Transnasal and transoral No (5m) 2008 [44] effusion anterior and postero- ectoderm, bifid tip uvuka, approach inferior walls, entoderm ankyloglossia widened ET 23 Agrawal et 1m M L Life threating CT, MR ET mesoderm, Intubation required No Endoscopic ligature and snare ?(?) al., 2009 upper airway ectoderm excision [45] obstruction 24 Chen et al., 10m F L Discharging ear CT, MR ET, widened ET mesoderm, Middle ear effusion, upper - Biopsy Transoral endoscopic resection, ?(?), small 2010 [46] ectoderm, airway obstruction with soft palate split residual entoderm obstructive sleep apnoea tympanic perforation 25 Wang et al., 14y M L Discharging ear CT, MR ET mesoderm, Discharging ear since - Unknown middle ear Transnasal and transoral ?(?) 2011 [47] ectoderm 1year of age, pedicle surgery approach with cutoff of the adhering to the inner side - Unknown middle ear torus to enlarge the of the internal surgery nasopharyngeal orifice carotid artery - Radical mastoidectomy 26 Sim et al., 6m F R Discharging ear CT, MR ET, widened ET ectoderm Total tympanic membrane - Biopsy Revision mastoidectomy ?(?) 2011 [48] perforation, bony erosion, - Mastoidectomy extending to middle and external ear ° age at definitive diagnosis * recurrence after 9 years CT: computed tomography MR: magnetic resonance CA: carotid arteriography Supplemental table 3. Reports on Eustachian tube (ET) chondromas n Author Age Sex Ear Presentation Imaging Pathology Remarks Treatment Recurrence (Follow up) 1 Drennowa, 32y F R Throat fullness No Chondroma - Transoral removal ?(?) 1930 [49] 2 Yates, 1935 14y F ? ? No Myxochondroma After recurrent Transoral removal ?(?) [50] adenotomies 3 Kishore, 50y M R Throat and ear fullness, nasal X-ray Chondroma as a globular fleshy reddish mass - Transoral removal ?(?) 1967 [51] obstruction, tinnitus since 2 1cm diameter attached by a thin stalk to the months posterior orifice of ET 4 Rao, 1970 18y M ? Throath, and ear fullness, X-ray Chondroma 3x2 inches, oval shaped, - Transpalatal removal ?(?) [52] nasal obstruction, voice lobulated change since 1 year 5 Ikeda et al., 66y F L Middle ear effusion, throat X-ray, Chondroma extended superiorly to the skull No intracranial Transcervical removal No (2y) 1987 [53] fullness CT, MR, base, inferiorly to 5 cm below the extension, tumor CA orbitomeatal line, anteriorly to medial and capsule firmly attached lateral pterygoid processes, posteriorly to the to the base of the skull cervical spine 6 Sichel et al., 47y F L Vertigo, sensorineural CT, CA Chondroma extended from the jugular No intracranial Anterior petrosectomy Persistence of a 1994 [54] hearing loss. Progressive foramen to the geniculate ganglion and extension via transcochlear small mass in the facial nerve palsy, vestibular through the carotid canal and ET to the approach with facial left cavernous paresis, middle ear effusion 1 cavernous sinus nerve rerouting sinus (6y) y later 7 Sichel et al., 54y F R Headache, middle ear CT, MR Chondroma extended from the middle cranial Dura adhesion, no - Fine-needle aspiration No (6y) 1994 [54] effusion fossa to the temporomandibular joint and intracranial extension - open biopsy through middle ear preauricular incision - TTD, bicoronal flap and osteotomy of the zygomatic arch CT: computed tomography MR: magnetic resonance CA, carotid arteriogram Supplemental table 4. Reports on Eustachian tube (ET) melanomas. n Author A Sex Ear Presentation Imaging Pathology Remarks Treatment Follow up, ge outcome (cause of death) 1 Handrock et al., 58 F L Discharging ear for X-ray Pedicled melanoma (3x1 cm) Erosion of the Initial paracentesys, bioptic 1y, P (cerebral 1980 [55] y 3y, then sudden originating from the pharyngeal medial wall of the paracentesys, exploratory invasion) deafness and ostium of ET and extending into tympanic box and of tympanotomy, ET biopsy. peripheral facial palsy nasopharynx, middle ear, internal ear. the facial canal No radical or palliative Cervical and mesenterial positive treatment reported nodes. Lung and abdomen metastases. 2 Lai et al., 2001 58 F R Progressive aural MR, selective digital Melanoma (1x1 cm) originating from Empirical Endoscopic excision 15m, CR [56] y fullness, pulsatile subtraction and occupying the pharyngeal ostium impression of a followed by radiotherapy tinnitus, hearing angiography, whole of ET. No regional or distant haemangioma impairment for more body CT scan metastases at diagnosis than 2m 3 Racic et al., 74 F L Bilateral neck US and CT of the Expansive-growing melanoma (2 cm - Chemotherapy ? 2003 [57] y lymphnode swelling neck, CT of the Ø) originating from the pharyngeal for 6 m, middle ear nasopharynx, chest ostium of ET, protruding into the effusion and abdomen CT, nasopharynx and extending into the bone scintihraphy middle ear. Cervical bilateral positive nodes. Lung metastases. 4 Baek et al., 2006 62 F R 18m hearing MR Melanoma originating from ET Biopsy taken from Neoadiuvant radiotherapy, 1y, CR [58] y impairment and 9m extending to nasopharynx and middle external auditory type C infratemporal fossa bloody discharging ear. canal approach ear 5 Tywończuk- 53 F L Progressive aural MR Melanoma (1.6x2x1.8 cm) originating - Radiotherapy 2y, P Szulc et Kibiłda, y fullness, hearing from and occupying the pharyngeal (metastases) 2007 [59] impairment for 2m ostium of ET. 6 Tanaka et al., 41 M R Progressive aural CT, MR, chest CT, US Melanoma (2.8x3.5 cm) originating - Radiotherapy, adjuvant 8m, CR 2008 [60] y fullness, hearing of the abdomen, PET from cartilagineous ET. No chemotherapy impairment for more metastases. than 3m 7 Yang et al., 2009 75 M L Intermittent epistaxis MR Melanoma (1.2x2.0x1.4 cm) Middle ear effusion ? ? [61] y originating from ET and extending to the nasopharynx. No metastases. 8 Yang et al., 2009 35 F L 2y hearing MR Melanoma (1.4x2.5x1.6 cm) - ? ? [61] y impairment, 1m originating from ET and extending to epistaxis the nasopharynx. No metastases. CT: computed tomography MR: magnetic resonance PET: positron emission tomography US: ultrasonography CR: complete remission P: progression of disease Supplemental table 5. Reports on Eustachian tube (ET) carcinomas. Author Age Sex Ear Presentation Imaging Pathology Remarks Treatment Survival/follow up (outcome) 1 Negri, 1888 ? M ? Negri-Jacod syndrome No Irregular tumor mass with Intracranial invasion ? 4 y (?) [11] ulceration in the orifice of the tube and invading Rosenmueller fossa 2 Procter, ? ? ? Persistent tubal No Soft granulation tissue, easily Omolateral lymphnodes ? 7 m (P, 1912 [62] obstruction bleeding, highly malignant enlargement, intracranial intracranial carcinoma invasion invasion through jugular foramen) 3 Patterson, 48y F L Ear fullness No Walnut-size squamous and Clinically benign. No First removal 10y before, ?(?) 1913 [63] polygonal cell carcinoma cervical lymphnodes recurrence removed by a snare originating from ET involvement reported. pharyngeal ostium, no ulceration 4 Jacod, 1921 64y M L Deafness and tinnitus, No Firm tumor (transitional cell No cervical lymphnodes Radium 6 m (P) [64] trigeminal nevralgia, carcinoma/sarcoma?), involvement reported. obstructed left nostril, enlarged ostium paralysis of IV, V, paresis of III 5 Jacod, 1921 32y M L Deafness and tinnitus, No (transitional cell Intracranial and ? 7 m (P) [64] trigeminal pain, carcinoma/sarcoma?) nasopharyngeal invasion. headache, paresis of III No cervical lymphnodes involvement reported. 6 Charleux et 60y M L Ear pain Salpingoscopy Reddish growth of the orifice Deep soreness on breathing, Radium relieved pain, but P ?(P) al., 1935 of ET: prickle cell paralysis of the left [65] epithelioma oculomotor and abducens nerves, diplopia. No cervical lymphnodes involvement reported. 7 Jacod, 1936 40y M L Deafness and otalgia, No Irregular hypertrophy of the No cervical lymphnodes X-ray followed by ?(?) [66] intermittent temporal orifice of ET (transitional cell involvement reported. transmaxillary resection of ET headache carcinoma/reticular cell sarcoma?) 8 Schumaker, 60y M L 6 weeks fullness and No Poorly differentiated Yellowish TM. No cervical 2x1 millicurie radon seed 3 y (CR, coronary 1940 [67] many years deafness, squamous cell carcinoma lymphnodes involvement implanted 7-8mm into the tumor, accident) gradual ET obstruction originating from ET reported. 3 weekly doses of 300 r to the leading to diagnosis 3 pharyngeal ostium neck weeks later 9 Schumaker, 54y F L Deafness for 2 m, No Round, red, cauliflower-like No cervical lymphnodes Radium ? (?) 1940 [67] yellowish drum with growth, pedicled highly involvement reported. fluid levels malignant squamous cell carcinoma, diameter 12 mm 10 Brownell, 33y M R Deafness and tinnitus, No Poorly differentiated Cervical adenopathy, Deep x-ray 14 m (P) 1940 [68] occipital headache, dull squamous cell carcinoma distant metastases (ribs, tympanic membrane originating from the sternum, vertebrae, midportion of ET, diameter 3 cranium, spleen, liver) cm 11 Brownell, 57y M L Intermittent and then No Medullary squamous cell Intracranial invasion Deep x-ray 16 m (P) 1940 [68] constant ear pain, carcinoma (outher third of ET, petrosa, followed by diplopia, infratemporal fossa, red and thick tympanic gasserian ganglion). No membrane with polyp cervical lymphnodes through posterior involvement reported. perforation; later VI palsy, trigeminal hyperestesia: Gradenigo CR: complete remission PR: partial regression of disease P: progression of disease Supplemental table 6. Reports on Eustachian tube (ET) sarcomas. n Author Age Sex Ear Presentation Imaging Pathology Remarks Treatment Survival 1 Jacod, 68y M L Deafness and No Ovoidal firm tumor (small round cell sarcoma) without ulceration One month after first Surgical removal 5 m (P) 1914 tinnitus, ear pain originating from cartilagineous ET surgery a chain of through transmanxillar [74] enlarged lymphondes approach was removed from the neck. 2 Jacod, 53y M L Deafness and No Tumor (small round cell sarcoma) originating from ET pharyngeal Recurrence in the Surgical removal 6 m (P) 1914 tinnitus, ear and ostium, enlarged ostium regional lymphnodes through transmaxillar [74] omolateral head after 2 m approach pain, left nostril obstruction 3 Lin et 44y M R 3 months CT, MR Synovial sarcoma originating from the lower portion of the anterior Normal mucosa over Transnasal endoscopic 5 y (CR) al., 2009 progressive nasal cushion of the ET (7.0x3.5 cm). Predominantly plump and elongated the mass with surgery, transoral [75] obstruction spindle sarcoma cells with overlapped nuclei and 19x10 mitotic prominent blood removal; adjuvant count focally forming herringbone-like fascicular pattern with vessels, soft palate irradiation to 64.8 Gy staghorn-like vasculature. No tumor necrosis. Epithelial Membrane pushed forward and Antigen, CK7 + (markers of epithelial differentiation); CD99, CD56, hypomobile bcl2 +; SYT-SSX2 fusion transcript at PCR. P: progression CT: computed tomography MR: magnetic resonance CR: complete remission Supplemental table 7. Single reports on other primary lesions of Eustachian tube (ET). n Author Age Sex Ear Presentation Imaging Pathology Remarks Treatment Follow up (outcome) 1 Hildyard and 22y F R Hearing loss since 15 years Tympanography (contrast Osteoma (4mm) at the tympanic - Removal through ?(?) Compere, 1959 medium injection in the middle orifice of ET. Central perforation myringotomy [76] ear); postoperative X-ray without drainage 2 Hirokawa et al., 72y F L Otalgia from several months, CT Horn-like cartilaginous lesion of Normal otoscopy Transnasal 1y (CR) 2001 [77] aggravated by nose blowing, the medial cushion of torus endoscopic occasional ear fullness and tubarius, covering chronically excision tinnitus inflamed mucosa 3 Kirsch et al., 55y F L Bloody otorrhea PET Foreign body reaction: Teflon Teflon injection ? ?(?) 2007 [78] granuloma treatment in 1971 for patulous ET 4 Chrysovergis et 56y M R 4 months of hearing loss, No Cylindrical cell papilloma - Transnasal ?(?) al., 2010 [79] otalgia, vertigo and tinnitus presenting as a soft nodular lesion endoscopic at the pharyngeal opening of ET excision CT: computed tomography PET: positron emission tomography