SCYA 2017-2018 Before & After Care Schedule
Parents must complete this form and circle the days your child will be attending the SCYA program. Return on or before the 15 th of every month to the Program or SCYA Office.
Circle: Full time before care Part time before care Full time after care Part time after care
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
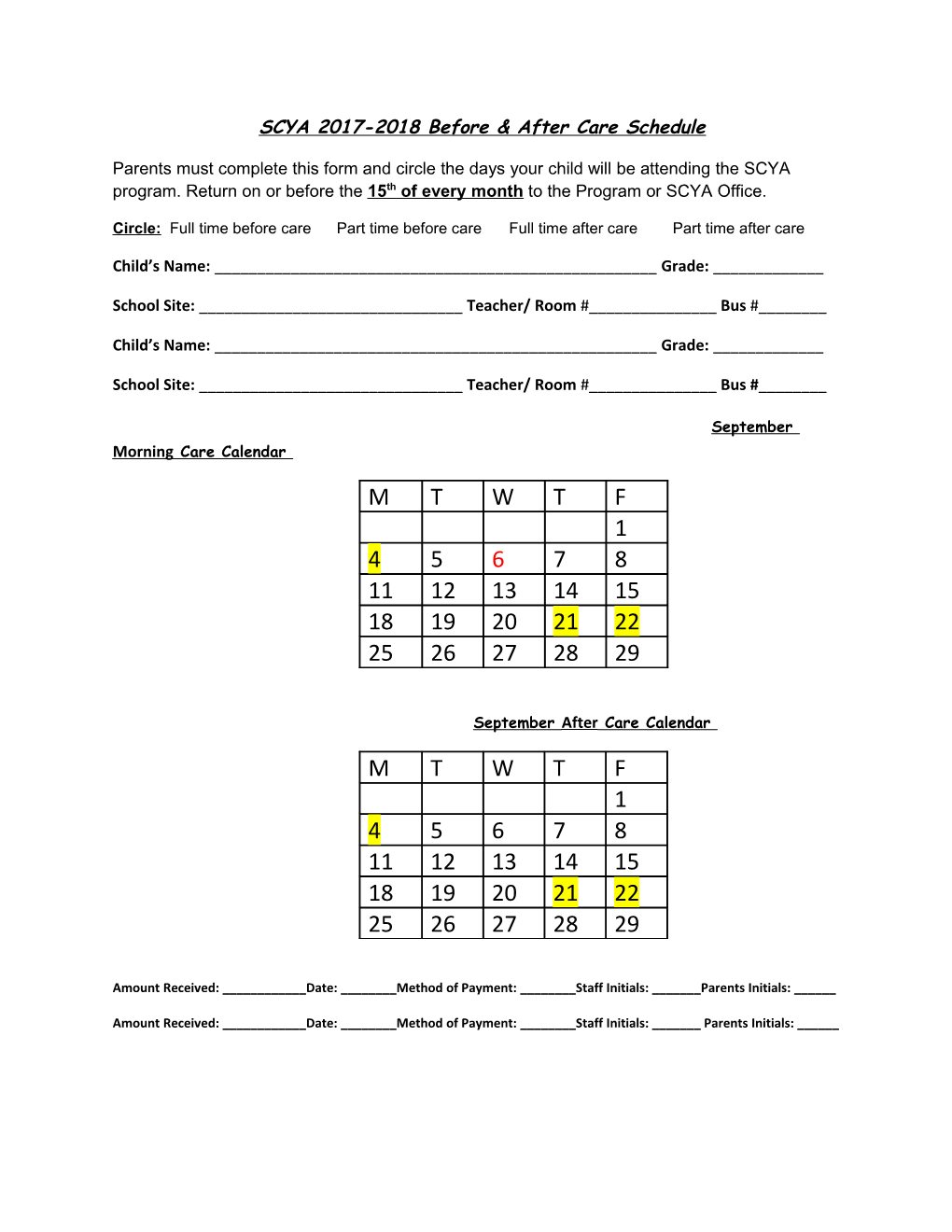
September Morning Care Calendar
M T W T F 1 4 5 6 7 8 11 12 13 14 15 18 19 20 21 22 25 26 27 28 29
September After Care Calendar
M T W T F 1 4 5 6 7 8 11 12 13 14 15 18 19 20 21 22 25 26 27 28 29
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
SCYA 2017-2018 Before & After Care Schedule
Parents must complete this form and circle the days your child will be attending the SCYA program. Return on or before the 15 th of every month to the Program or SCYA Office.
Circle: Full time before care Part time before care Full time after care Part time after care
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
October Morning Care Calendar
M T W T F 2 3 4 5 6 9 10 11 12 13 16 17 18 19 20 23 24 25 26 27 30 31
October After Care Calendar
M T W T F 2 3 4 5 6 9 10 11 12 13 16 17 18 19 20 23 24 25 26 27 30 31
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
SCYA 2017-2018 Before & After Care Schedule
Parents must complete this form and circle the days your child will be attending the SCYA program. Return on or before the 15 th of every month to the Program or SCYA Office.
Circle: Full time before care Part time before care Full time after care Part time after care
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
November Morning Care Calendar
M T W T F 1 2 3 6 7 8 9 10 13 14 15 16 17 20 21 22 23 24 27 28 29 30
November After Care Calendar
M T W T F 1 2 3 6 7 8 9 10 13 14 15 16 17 20 21 22 23 24 27 28 29 30
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
SCYA 2017-2018 Before & After Care Schedule
Parents must complete this form and circle the days your child will be attending the SCYA program. Return on or before the 15 th of every month to the Program or SCYA Office.
Circle: Full time before care Part time before care Full time after care Part time after care
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
December Morning Care Calendar
M T W T F 1 4 5 6 7 8 11 12 13 14 15 18 19 20 21 22 25 26 27 28 29
December After Care Calendar
M T W T F 1 4 5 6 7 8 11 12 13 14 15 18 19 20 21 22 25 26 27 28 29
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
SCYA 2017-2018 Before & After Care Schedule
Parents must complete this form and circle the days your child will be attending the SCYA program. Return on or before the 15 th of every month to the Program or SCYA Office.
Circle: Full time before care Part time before care Full time after care Part time after care
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
January Morning Care Calendar
M T W T F 1 2 3 4 5 8 9 10 11 12 15 16 17 18 19 22 23 24 25 26 29 30 31
January After Care Calendar
M T W T F 1 2 3 4 5 8 9 10 11 12 15 16 17 18 19 22 23 24 25 26 29 30 31
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
SCYA 2017-2018 Before & After Care Schedule
Parents must complete this form and circle the days your child will be attending the SCYA program. Return on or before the 15 th of every month to the Program or SCYA Office.
Circle: Full time before care Part time before care Full time after care Part time after care
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
February Morning Care Calendar
M T W T F 1 2 5 6 7 8 9 12 13 14 15 16 19 20 21 22 23 26 27 28
February After Care Calendar
M T W T F 1 2 5 6 7 8 9 12 13 14 15 16 19 20 21 22 23 26 27 28
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
SCYA 2016-2017 Before & After Care Schedule
Parents must complete this form and circle the days your child will be attending the SCYA program. Return on or before the 15 th of every month to the Program or SCYA Office.
Circle: Full time before care Part time before care Full time after care Part time after care
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
March Morning Care Calendar
M T W T F 1 2 5 6 7 8 9 12 13 14 15 16 19 20 21 22 23 26 27 28 29 30
March After Care Calendar
M T W T F 1 2 5 6 7 8 9 12 13 14 15 16 19 20 21 22 23 26 27 28 29 30
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
SCYA 2016-2017 Before & After Care Schedule
Parents must complete this form and circle the days your child will be attending the SCYA program. Return on or before the 15 th of every month to the Program or SCYA Office.
Circle: Full time before care Part time before care Full time after care Part time after care
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
April Morning Care Calendar
M T W T F 2 3 4 5 6 9 10 11 12 13 16 17 18 19 20 23 24 25 26 27
April After Care Calendar
M T W T F 2 3 4 5 6 9 10 11 12 13 16 17 18 19 20 23 24 25 26 27
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
SCYA 2017-2018 Before & After Care Schedule
Parents must complete this form and circle the days your child will be attending the SCYA program. Return on or before the 15 th of every month to the Program or SCYA Office.
Circle: Full time before care Part time before care Full time after care Part time after care
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
May Morning Care Calendar
M T W T F 1 2 3 4 7 8 9 10 11 14 15 16 17 18 21 22 23 24 25 28 29 30 31
May After Care Calendar
M T W T F 1 2 3 4 7 8 9 10 11 14 15 16 17 18 21 22 23 24 25 28 29 30 31
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
SCYA 2017-2018 Before & After Care Schedule
Parents must complete this form and circle the days your child will be attending the SCYA program. Return on or before the 15 th of every month to the Program or SCYA Office.
Circle: Full time before care Part time before care Full time after care Part time after care
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
Child’s Name: ______Grade: ______
School Site: ______Teacher/ Room #______Bus #______
June Morning Care Calendar
M T W T F 1 4 5 6 7 8 11 12 13 14 15 18 19 20 21 22 25 26 27 28 29
June After Care Calendar
M T W T F 1 4 5 6 7 8 11 12 13 14 15 18 19 20 21 22 25 26 27 28 29
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______
Amount Received: ______Date: ______Method of Payment: ______Staff Initials: ______Parents Initials: ______