Tel: 0114 2900250 Email: [email protected] This form is for both Participants and Volunteers.
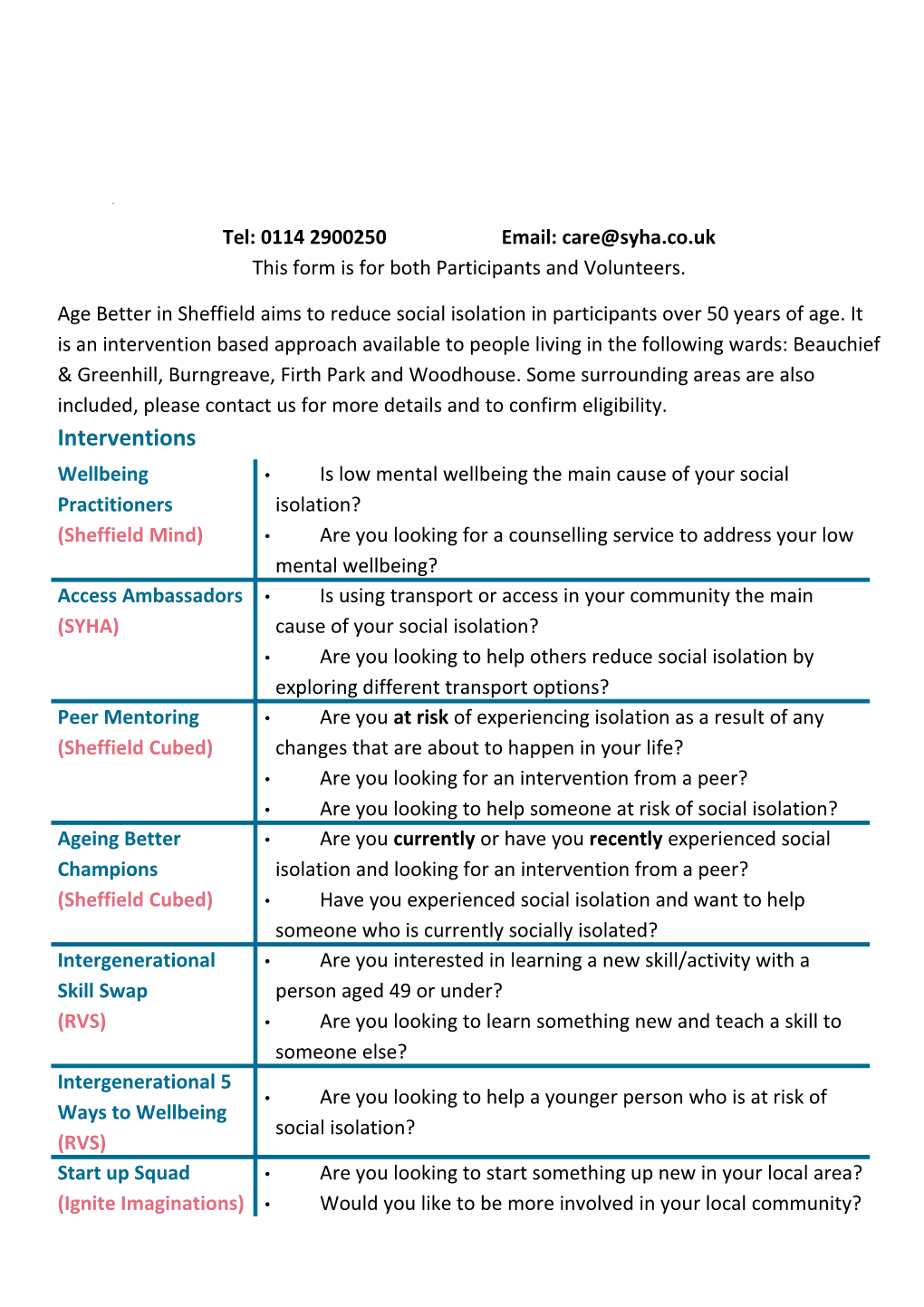
Age Better in Sheffield aims to reduce social isolation in participants over 50 years of age. It is an intervention based approach available to people living in the following wards: Beauchief & Greenhill, Burngreave, Firth Park and Woodhouse. Some surrounding areas are also included, please contact us for more details and to confirm eligibility. Interventions Wellbeing • Is low mental wellbeing the main cause of your social Practitioners isolation? (Sheffield Mind) • Are you looking for a counselling service to address your low mental wellbeing? Access Ambassadors • Is using transport or access in your community the main (SYHA) cause of your social isolation? • Are you looking to help others reduce social isolation by exploring different transport options? Peer Mentoring • Are you at risk of experiencing isolation as a result of any (Sheffield Cubed) changes that are about to happen in your life? • Are you looking for an intervention from a peer? • Are you looking to help someone at risk of social isolation? Ageing Better • Are you currently or have you recently experienced social Champions isolation and looking for an intervention from a peer? (Sheffield Cubed) • Have you experienced social isolation and want to help someone who is currently socially isolated? Intergenerational • Are you interested in learning a new skill/activity with a Skill Swap person aged 49 or under? (RVS) • Are you looking to learn something new and teach a skill to someone else? Intergenerational 5 • Are you looking to help a younger person who is at risk of Ways to Wellbeing social isolation? (RVS) Start up Squad • Are you looking to start something up new in your local area? (Ignite Imaginations) • Would you like to be more involved in your local community? Sharing Information Agreement Form
By completing this form you are agreeing for your details to be passed onto the Delivery Partners commissioned by the Age Better in Sheffield programme.
Taking Part and Use of information Yes No I agree to take part in the Age Better in Sheffield Programme. Taking part in the project may include being interviewed and recorded (audio or video). I understand that my words may be quoted in publications, reports, web pages, and other research outputs. I agree to assign the copyright I hold in any materials related to this project to Age Better in Sheffield. Use of the information I provide beyond this project Age Better in Sheffield aims to collect better evidence of the impact of interventions. I agree for the data I provide to used for research. Including but not limited to Sheffield Hallam University. I understand that other genuine researchers will have access to this data only if they agree to preserve the confidentiality of the information as requested in this form. I understand that other genuine researchers may use my words in publications, reports, web pages, and other research outputs, only if they agree to preserve the confidentiality of the information as requested in this form. Use of your NHS Data I understand that my responses will be linked to other health and social care records held by the Council and the NHS. This data will be linked using your NHS number in accordance with current NHS Information Governance regulations to ensure that your personal data is safeguarded and used appropriately.
Confidentiality Your involvement with Age Better in Sheffield is of a confidential nature and information you share with us will normally be kept within the programme and only given to others with your permission below. However, information may be shared without permission in the following circumstances: If we are required to do so by law Risk of significant harm to you and/or someone else Child/adult protection concerns
Name (Please Print): Signature: Date: Please tick this box to confirm you agree if completing this form electronically
Confidential - If you complete this form SYHA will store and process your data in accordance with the requirements of its Data Protection Policy and in keeping with the Data Protection Act 1988. Registered Address: SYHA, 43-47 Wellington Street, Sheffield, S1 4HF Intervention referred to (Please tick only one) Peer Mentoring Ageing Better Champions Access Ambassadors
Intergenerational 5 Ways to Wellbeing Intergenerational Skill Swap
Wellbeing Practitioners Start Up Squad
Referrer Details Referral Date: Referral Source:
Referrer Name and Company (if Applicable):
Personal Details Title: Forename: Surname:
Date of Birth: Economic Status: Religion: Sex: Is your Gender the same as the gender you were assigned at birth?
NHS Number: Nationality: Living Arrangements: Relationship Status: Caring Responsibilities: Sexual Orientation: Language: If other please state: Literacy: Preferred Communication: Contact Details Address:
Postcode: Telephone Number:
Mobile Number: Email:
This form must be fully completed before submitting
Personal Details (cont.)
Race (Please tick one box) White Asian or Asian British Other Ethnic Group English / Welsh / Scottish / Indian Yemeni Northern Irish/ British Irish Pakistani Other Arab Gypsy/ Irish Traveller Chinese Other ethnic group Roma Other Asian background Mixed / Dual Heritage Other European Black / African / Caribbean White and Black Caribbean or Black British Other white background Caribbean White and Black African Somali White and Asian Not Known Other African background Other mixed background Does not wish to disclose Other Black background
Disability Status:
Do you have an impairment that has or is expected to last more than 12 months? (More than one box can be ticked) Ability to hear – Speech impairment Ability to see - blind profound to mild deafness or partial sighted Mobility or physical Long-standing illness or Learning or impairment –limits or diagnosed health condition developmental restricts physical e.g. cancer, HIV, diabetes, disability e.g. Downs movement, coordination or chronic heart disease, syndrome, autism or manual dexterity rheumatoid arthritis dyslexia Mental ill health e.g. Bi Impaired memory / Other polar disorders, concentration or ability to schizophrenia, depression understand e.g. Stroke, Dementia, Dyslexia, Head- injury If Dementia please tick: Not Known Does not wish to disclose None
Once fully completed please send to [email protected] Alternatively please post to: Core Services, SYHA, 43 – 47 Wellington Street, Sheffield, S1 4HF