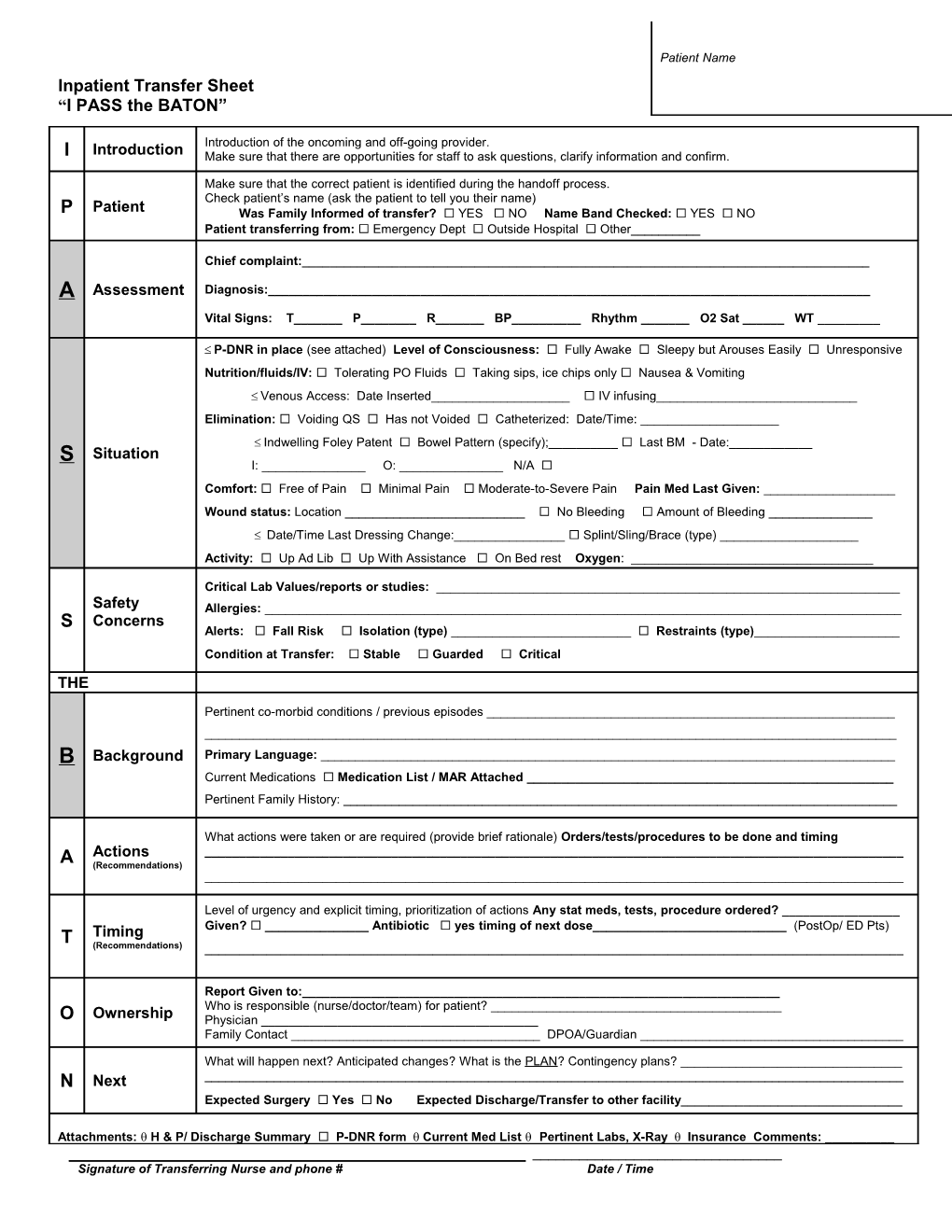
Patient Name Inpatient Transfer Sheet “I PASS the BATON”
Introduction of the oncoming and off-going provider. I Introduction Make sure that there are opportunities for staff to ask questions, clarify information and confirm.
Make sure that the correct patient is identified during the handoff process. Check patient’s name (ask the patient to tell you their name) P Patient Was Family Informed of transfer? YES NO Name Band Checked: YES NO Patient transferring from: Emergency Dept Outside Hospital Other______
Chief complaint:______A Assessment Diagnosis:______Vital Signs: T______P______R______BP______Rhythm ______O2 Sat ______WT ______
P-DNR in place (see attached) Level of Consciousness: Fully Awake Sleepy but Arouses Easily Unresponsive Nutrition/fluids/IV: Tolerating PO Fluids Taking sips, ice chips only Nausea & Vomiting Venous Access: Date Inserted______ IV infusing______Elimination: Voiding QS Has not Voided Catheterized: Date/Time: ______ Indwelling Foley Patent Bowel Pattern (specify);______ Last BM - Date:______S Situation I: ______O: ______N/A Comfort: Free of Pain Minimal Pain Moderate-to-Severe Pain Pain Med Last Given: ______Wound status: Location ______ No Bleeding Amount of Bleeding ______ Date/Time Last Dressing Change:______ Splint/Sling/Brace (type) ______Activity: Up Ad Lib Up With Assistance On Bed rest Oxygen: ______
Critical Lab Values/reports or studies: ______Safety Allergies: ______S Concerns Alerts: Fall Risk Isolation (type) ______ Restraints (type)______Condition at Transfer: Stable Guarded Critical THE
Pertinent co-morbid conditions / previous episodes ______B Background Primary Language: ______Current Medications Medication List / MAR Attached ______Pertinent Family History: ______
What actions were taken or are required (provide brief rationale) Orders/tests/procedures to be done and timing Actions ______A (Recommendations) ______
Level of urgency and explicit timing, prioritization of actions Any stat meds, tests, procedure ordered? ______Given? ______Antibiotic yes timing of next dose______(PostOp/ ED Pts) T Timing (Recommendations) ______
Report Given to:______Who is responsible (nurse/doctor/team) for patient? ______O Ownership Physician ______Family Contact ______DPOA/Guardian ______
What will happen next? Anticipated changes? What is the PLAN? Contingency plans? ______N Next ______Expected Surgery Yes No Expected Discharge/Transfer to other facility______
Attachments: H & P/ Discharge Summary P-DNR form Current Med List Pertinent Labs, X-Ray Insurance Comments: ______Signature of Transferring Nurse and phone # Date / Time