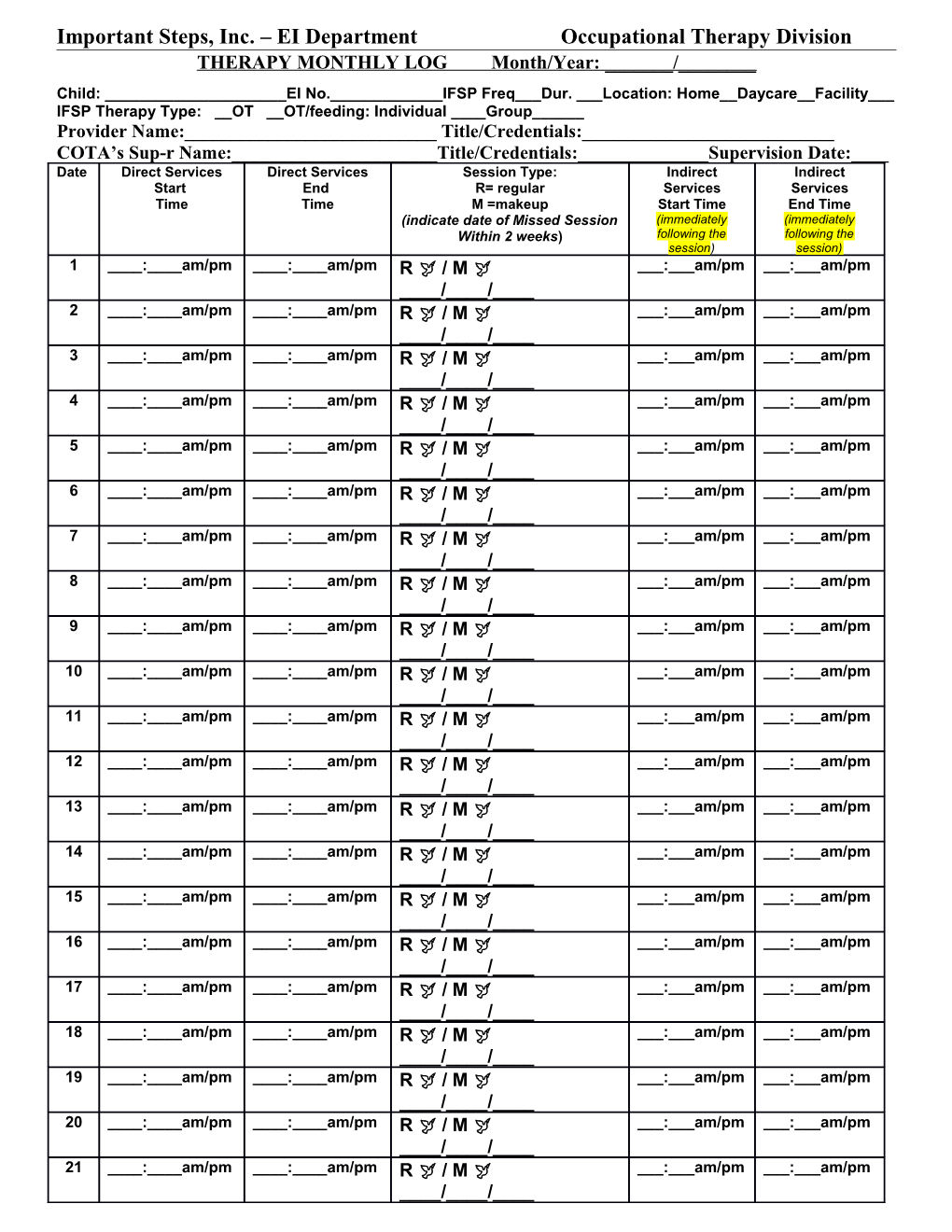
Important Steps, Inc. – EI Department Occupational Therapy Division THERAPY MONTHLY LOG Month/Year: ______/______Child: ______EI No.______IFSP Freq___Dur. ___Location: Home__Daycare__Facility___ IFSP Therapy Type: __OT __OT/feeding: Individual ____Group______Provider Name:______Title/Credentials:______COTA’s Sup-r Name:______Title/Credentials:______Supervision Date:____ Date Direct Services Direct Services Session Type: Indirect Indirect Start End R= regular Services Services Time Time M =makeup Start Time End Time (indicate date of Missed Session (immediately (immediately Within 2 weeks) following the following the session) session) 1 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 2 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 3 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 4 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 5 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 6 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 7 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 8 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 9 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 10 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 11 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 12 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 13 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 14 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 15 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 16 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 17 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 18 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 19 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 20 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 21 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 22 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 23 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 24 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 25 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 26 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 27 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 28 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 29 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 30 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____ 31 ____:____am/pm ____:____am/pm R / M ___:___am/pm ___:___am/pm ____/____/____
Service Provider’s Signature: ______Date:______Total Billable Sessions:______****Session Notes (Originals) Must be Attached and correspond to this Monthly Log-Page 1
Page 2-Instructions for Completing Monthly Log: Complete ALL demographic information at the top of the page, including child’s name and ID #, frequency and duration, type of service, and provider’s name and credentials. Next to the corresponding date of Direct service, enter start and end time of the provided session and record whether it is a regular or make-up session (if it is a make-up session, you must provide the date of the missed session and have a corresponding blank session note for it).
You must now also include any Indirect time spent on the case. For example, enter the time that you spent writing the session note (which must be after the completion of the session and at least 5 minutes in length). This excludes the travel time. Any time that you have spent on the case for that day EXCLUDING your time spent with the child/parent is considered INDIRECT time. Please note: basic sessions are 30-59 minutes; extended sessions are 60 minutes plus.; Sign, date, and indicate the number of billable sessions.
Instructions for Completing CPT/ICD-9 Codes on Session Notes_Attached Use the chart below to indicate the child’s type of delay (ICD-10 codes) (from evaluations) and the type of therapy you have provided (CPT codes).
ICD-9 Code-Use til ICD-10 Code-Effective CPT Code Description Unit Definition Restrictions 09/30/15 October 1, 2015 97110 Therapeutic 15 minutes Session limit 4 units 315.4 F82 Specific developmental Exercises to Developmental disorder of motor function develop strength coordination and endurance, disorder range of motion and flexibility 315.5 Mixed F82 Specific developmental developmental disorder of motor function disorder 315.9 F81.9 Developmental Developmental disorder of scholastic skills, Delay NOS unspecified *or F89 Unspecified disorder of psychological development
781.3 Lack of R27.0 Ataxia Unspecified coordination *or R27.8 Other lack of (Chose only one Coordination ICD-10-as specific *or to child) R27.9 Unspecified lack of coordination
728.3 Other M62.89 Other specified specific muscle disorders of muscle disorders
728.9 Unspecified M62.9 Disorder of muscle, disorder of unspecified muscle, ligament or fascia
728.87 Muscle M62.81 Muscle weakness weakness (generalized)
783.42 Delayed R62.0 Delayed milestone in milestones childhood 97112 Neuromuscular 15 minutes Session limit 4 units See above codes Reeducation of movement, balance, coordination, kinesthetic sense, posture, and/or proprioception for sitting and/or standing See above codes 97124 Massage Therapy 15 minutes Session limit 4 units See above codes including effleurage, pertrissage, tapotement (stroking, compression, percussion) See above codes 97150 Group Therapeutic Encounter I unit per recipient See above codes (2 or more individuals) See above codes 97530 Kinetic therapy- 15 minutes Session limit 4 units See above codes Therapeutic activities, direct (1X1) patient contact by the provider (use of dynamic activities to improve functional performance) See above codes 97533 Sensory Integration 15 min Session limit 4 units See above codes to enhance sensory processing and promote adaptive responses to environmental demands direct (1X1) patient contact by the provider. See above codes 97532 Development of 15 min. Session limit 4 units See above codes cognitive skills to improve attention, memory, problem solving (includes compensatory training), direct (1x1) patient contact by the provider, each 15 minutes See above codes 97755 Assistive 15 minutes With written report Technology assessment See above codes In the event you require more codes please refer to: http://occupational-therapy.advanceweb.com/Article/Everything-You-Wanted-to-Know-About-Coding.aspx http://www.icd10data.com/Convert
Therapy Monthly Log-OT-Page 3