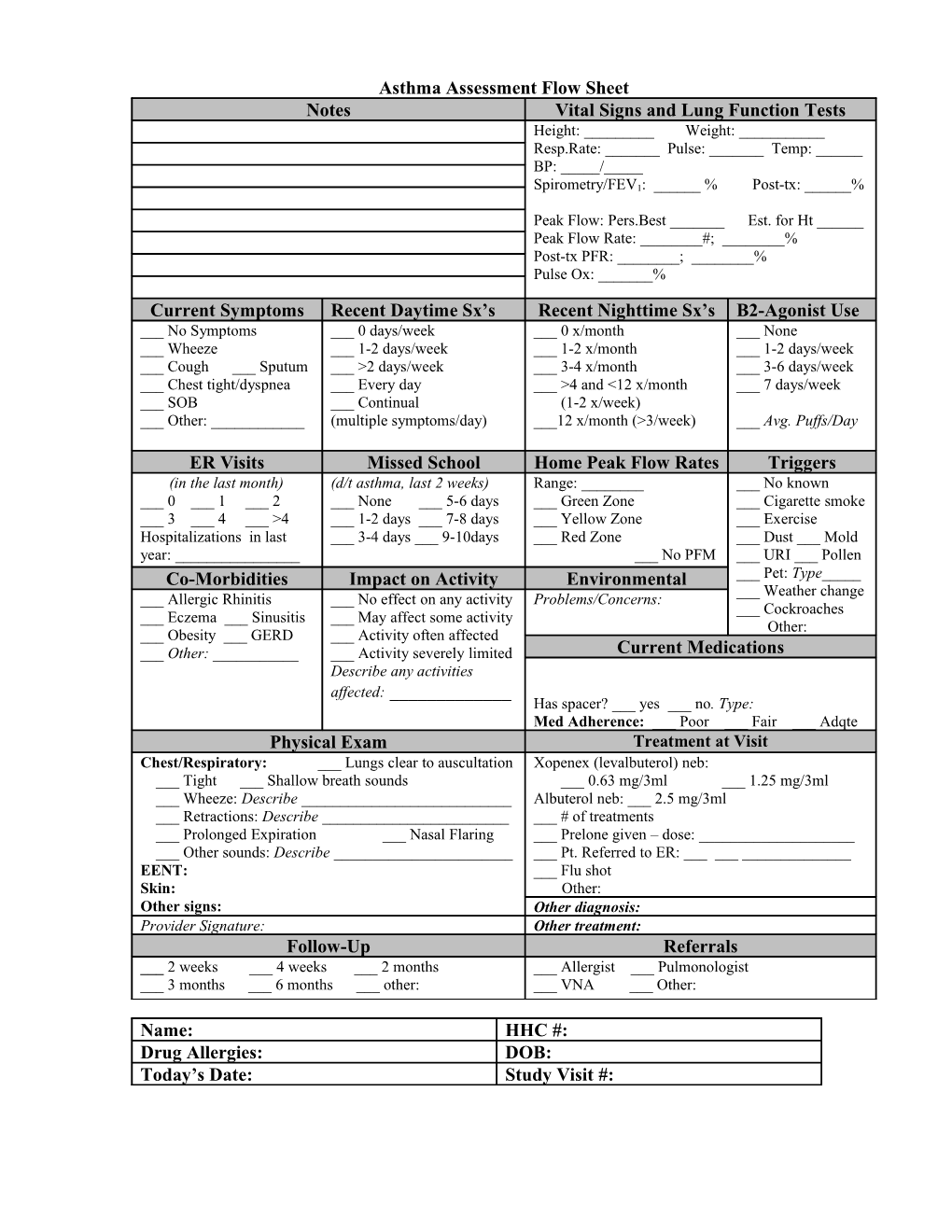
Asthma Assessment Flow Sheet Notes Vital Signs and Lung Function Tests Height: ______Weight: ______Resp.Rate: ______Pulse: ______Temp: ______BP: _____/_____
Spirometry/FEV1: ______% Post-tx: ______%
Peak Flow: Pers.Best ______Est. for Ht ______Peak Flow Rate: ______#; ______% Post-tx PFR: ______; ______% Pulse Ox: ______%
Current Symptoms Recent Daytime Sx’s Recent Nighttime Sx’s B2-Agonist Use ___ No Symptoms ___ 0 days/week ___ 0 x/month ___ None ___ Wheeze ___ 1-2 days/week ___ 1-2 x/month ___ 1-2 days/week ___ Cough ___ Sputum ___ >2 days/week ___ 3-4 x/month ___ 3-6 days/week ___ Chest tight/dyspnea ___ Every day ___ >4 and <12 x/month ___ 7 days/week ___ SOB ___ Continual (1-2 x/week) ___ Other: ______(multiple symptoms/day) ___12 x/month (>3/week) ___ Avg. Puffs/Day
ER Visits Missed School Home Peak Flow Rates Triggers (in the last month) (d/t asthma, last 2 weeks) Range: ______No known ___ 0 ___ 1 ___ 2 ___ None ___ 5-6 days ___ Green Zone ___ Cigarette smoke ___ 3 ___ 4 ___ >4 ___ 1-2 days ___ 7-8 days ___ Yellow Zone ___ Exercise Hospitalizations in last ___ 3-4 days ___ 9-10days ___ Red Zone ___ Dust ___ Mold year: ______No PFM ___ URI ___ Pollen Co-Morbidities Impact on Activity Environmental ___ Pet: Type______Weather change ___ Allergic Rhinitis ___ No effect on any activity Problems/Concerns: ___ Cockroaches ___ Eczema ___ Sinusitis ___ May affect some activity Other: ___ Obesity ___ GERD ___ Activity often affected ___ Other: ______Activity severely limited Current Medications Describe any activities affected: ______Has spacer? ___ yes ___ no. Type: Med Adherence: ___ Poor ___ Fair ___ Adqte Physical Exam Treatment at Visit Chest/Respiratory: ___ Lungs clear to auscultation Xopenex (levalbuterol) neb: ___ Tight ___ Shallow breath sounds ___ 0.63 mg/3ml ___ 1.25 mg/3ml ___ Wheeze: Describe ______Albuterol neb: ___ 2.5 mg/3ml ___ Retractions: Describe ______# of treatments ___ Prolonged Expiration ___ Nasal Flaring ___ Prelone given – dose: ______Other sounds: Describe ______Pt. Referred to ER: ______EENT: ___ Flu shot Skin: Other: Other signs: Other diagnosis: Provider Signature: Other treatment: Follow-Up Referrals ___ 2 weeks ___ 4 weeks ___ 2 months ___ Allergist ___ Pulmonologist ___ 3 months ___ 6 months ___ other: ___ VNA ___ Other:
Name: HHC #: Drug Allergies: DOB: Today’s Date: Study Visit #: