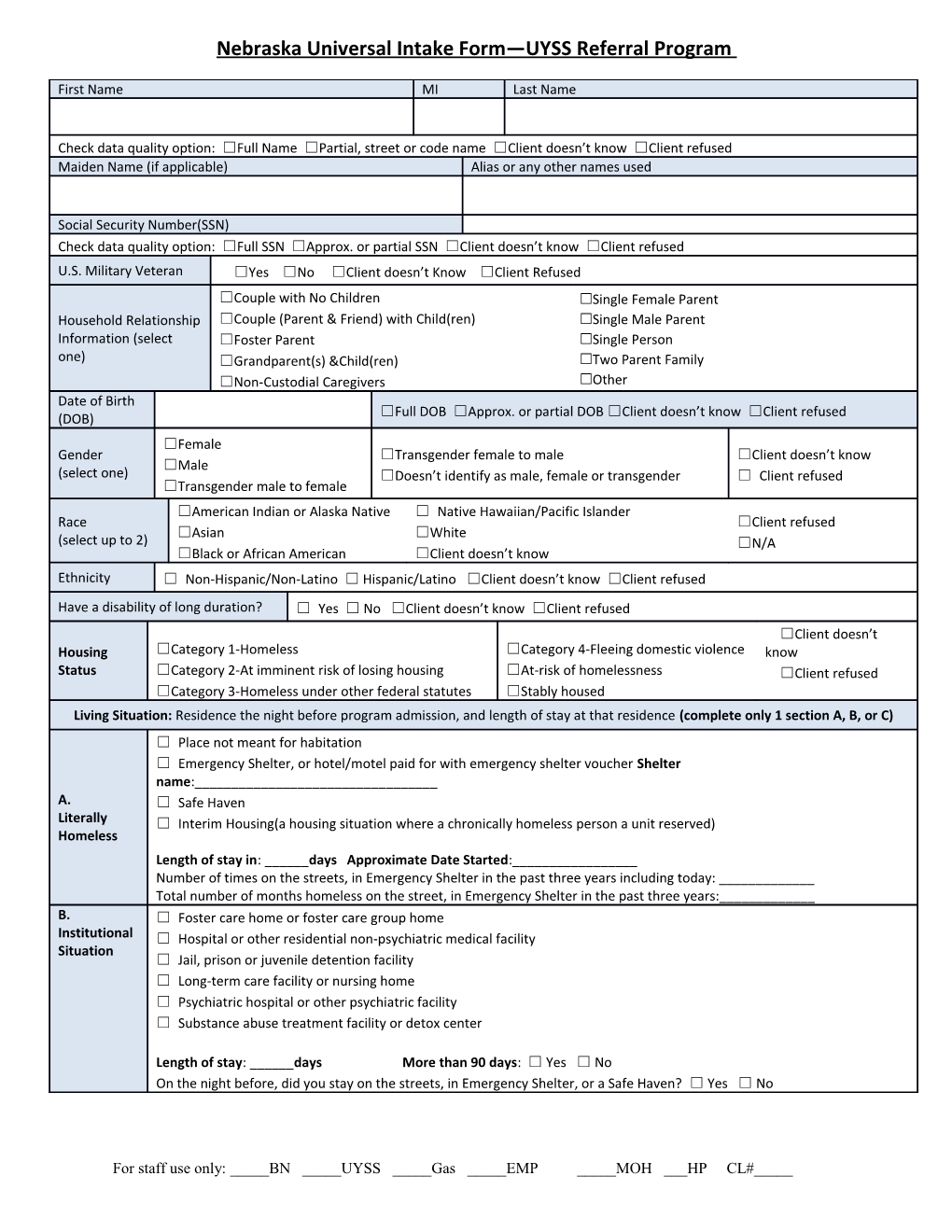
Nebraska Universal Intake Form—UYSS Referral Program
First Name MI Last Name
Check data quality option: ☐Full Name ☐Partial, street or code name ☐Client doesn’t know ☐Client refused Maiden Name (if applicable) Alias or any other names used
Social Security Number(SSN) Check data quality option: ☐Full SSN ☐Approx. or partial SSN ☐Client doesn’t know ☐Client refused U.S. Military Veteran ☐Yes ☐No ☐Client doesn’t Know ☐Client Refused ☐Couple with No Children ☐Single Female Parent Household Relationship ☐Couple (Parent & Friend) with Child(ren) ☐Single Male Parent Information (select ☐Foster Parent ☐Single Person one) ☐Grandparent(s) &Child(ren) ☐Two Parent Family ☐Non-Custodial Caregivers ☐Other Date of Birth ☐Full DOB ☐Approx. or partial DOB ☐Client doesn’t know ☐Client refused (DOB) ☐Female Gender ☐Transgender female to male ☐Client doesn’t know ☐Male (select one) ☐Doesn’t identify as male, female or transgender ☐ Client refused ☐Transgender male to female ☐American Indian or Alaska Native ☐ Native Hawaiian/Pacific Islander Race ☐Client refused ☐Asian ☐White (select up to 2) ☐N/A ☐Black or African American ☐Client doesn’t know Ethnicity ☐ Non-Hispanic/Non-Latino ☐ Hispanic/Latino ☐Client doesn’t know ☐Client refused Have a disability of long duration? ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused ☐Client doesn’t Housing ☐Category 1-Homeless ☐Category 4-Fleeing domestic violence know Status ☐Category 2-At imminent risk of losing housing ☐At-risk of homelessness ☐Client refused ☐Category 3-Homeless under other federal statutes ☐Stably housed Living Situation: Residence the night before program admission, and length of stay at that residence (complete only 1 section A, B, or C) ☐ Place not meant for habitation ☐ Emergency Shelter, or hotel/motel paid for with emergency shelter voucher Shelter name:______A. ☐ Safe Haven Literally ☐ Interim Housing(a housing situation where a chronically homeless person a unit reserved) Homeless Length of stay in: ______days Approximate Date Started:______Number of times on the streets, in Emergency Shelter in the past three years including today: ______Total number of months homeless on the street, in Emergency Shelter in the past three years:______B. ☐ Foster care home or foster care group home Institutional ☐ Hospital or other residential non-psychiatric medical facility Situation ☐ Jail, prison or juvenile detention facility ☐ Long-term care facility or nursing home ☐ Psychiatric hospital or other psychiatric facility ☐ Substance abuse treatment facility or detox center
Length of stay: ______days More than 90 days: ☐ Yes ☐ No On the night before, did you stay on the streets, in Emergency Shelter, or a Safe Haven? ☐ Yes ☐ No
For staff use only: _____BN _____UYSS _____Gas _____EMP _____MOH ___HP CL#_____ Approximate Date Started:______
☐ Hotel or motel paid for without emergency shelter voucher ☐ Owned by client, no ongoing housing subsidy ☐ Owned by client, with ongoing housing subsidy ☐ Permanent housing for formerly homeless persons(such as a CoC project; HUD legacy programs; or HOPWA PH) ☐ C. Rental by client, no ongoing housing subsidy Transitional ☐ Rental by client, with VASH subsidy & ☐ Rental by client, with GPD TIP subsidy Permanent ☐ Rental by client, with other ongoing housing subsidy Housing ☐ Residential project or halfway house with no homeless criteria Situation ☐ Staying or living in a family member's room, apartment or house ☐ Staying or living in a friend's room, apartment or house ☐ Transitional housing for homeless persons (including homeless youth)
Length of stay: ______days More than 7 days: ☐ Yes ☐ No On the night before, did you stay on the streets, in Emergency Shelter, or a Safe Haven? ☐ Yes ☐ No Approximate Date Started:______Length of Time Homeless Status Documented? ☐ Yes ☐ No Zip Code of Last Permanent ☐NE-500 BOS (Anywhere in Nebraska outside of Lincoln/Omaha) Client Location Address ☐NE-502 Lincoln ☐Self (head of household) ☐ Other: Non-relation member Relationship to Head of ☐ Head of Household’s Child ☐ Client doesn’t know Household ☐ Head of Household’s spouse or partner ☐ Client refused ☐ Head of Household’s other relation member As a child, were you ever in Foster Care or are you now? ☐ Yes ☐ No Domestic violence victim/survivor? ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused
☐ Within the past three months ☐ Client doesn’t know If yes for Domestic Violence victim/survivor, when ☐ Three to six months ago ☐ Client refused experience occurred ☐ From six to twelve months ago ☐ More than a year ago
If yes for Domestic Violence Victim/Survivor, are you ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused currently fleeing? ☐ No schooling completed ☐ GED ☐ Nursery school to 4th grade ☐ Post-Secondary School ☐ 5th or 6th grade ☐ Some College ☐ 7th grade or 8th grade ☐ Some Technical School ☐ 9th grade ☐ Graduate Degree Highest level of education attained ☐ 10th grade ☐ Technical School Certification ☐ 11th grade ☐ Client refused ☐ 12th grade, no diploma ☐ Client Doesn’t Know ☐ Some High School ☐ High school diploma Income Information
Income from any source? ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused Total Monthly CASH income: Write in total $ amount and complete the table below Total Monthly Income: $______Receives Income Sources Yes Monthly Amount $ No
AABD (Aid to Aged, Blind & Disabled) ☐ $ ☐ Alimony or Other Spousal Support ☐ $ ☐ Child Support ☐ $ ☐ Contributions from other People ☐ $ ☐ Earned Income (from job) ☐ $ ☐ General Assistance ☐ $ ☐ Pension or retirement income from job ☐ $ ☐ Pension/Retirement ☐ $ ☐ Private Disability Insurance ☐ $ ☐ Retirement Income from Social Security ☐ $ ☐ Self Employment Wages ☐ $ ☐ SSA ☐ $ ☐ SSDI ☐ $ ☐ SSI ☐ $ ☐ Stipend ☐ $ ☐ Unemployment Insurance ☐ $ ☐ VA Non-service connected disability compensation ☐ $ ☐ VA service-connected disability compensation ☐ $ ☐ Worker’s Compensation ☐ $ ☐ Other (specify): ☐ $ ☐
Page 3 of 18 Non-Cash Benefits Information
Non-cash benefits from any source ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused Receives the following Non-cash Benefit Types: Yes Monthly Amount $ (if known) No Supplemental Nutrition Assistance Program (SNAP) ☐ $ ☐ (Food Stamps) Special Supplemental Nutrition for Women, infants, ☐ N/A ☐ children(WIC) TANF Child Care Services ☐ $ ☐ TANF Transportation services ☐ N/A ☐ Other TANF funded services ☐ N/A ☐ Section 8, public housing, or other ongoing rent ☐ $ ☐ assistance Temporary rental assistance ☐ $ ☐ Other (specify): ☐ $ ☐ Health Insurance Information
Covered by Health Insurance ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused Type Covered Covered (Select all that apply) Yes No Medicaid ☐ ☐ Medicare ☐ ☐ State Children’s Health Insurance Program ☐ ☐ Veteran’s Administration (VA) Medical Services ☐ ☐ Employer-Provided Health Insurance ☐ ☐ Health Insurance obtained through COBRA ☐ ☐ Private Pay Health Insurance ☐ ☐ State Health Insurance for Adults ☐ ☐ Indian Health Services Program ☐ ☐ Other ( Specify): ☐ ☐ Client’s Residence/Last Permanent Address Street Address City State Zip code County of Current County of Legal Residence Residence Home Phone Number Cell Phone Work
Child –Please complete for any children in your household (1 child per table) First Name MI Last Name Social Security Number(SSN)
Date of Birth Ethnicity ☐ Non-Hispanic/Non-Latino ☐ Hispanic/Latino ☐Client refused (DOB) Race ☐American Indian or Alaska Native ☐ Native Hawaiian/Pacific Islander ☐Client doesn’t know (select up to ☐Asian ☐White ☐Client Refused 2) ☐Black or African American ☐Female Gender ☐Transgender female to male ☐Client doesn’t know ☐Male (select one) ☐Doesn’t identify as male, female or transgender ☐ Client refused ☐Transgender male to female Have a disability of long duration? ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused ☐Self (head of household) ☐ Other: Non-relation member Relationship ☐ Head of Household’s Child ☐ Client doesn’t know to Head of ☐ Household Head of Household’s spouse or partner ☐ Client refused ☐ Head of Household’s other relation member ☐ Yes ☐ No If yes, enter type Covered by Health Insurance I.E. Medicaid, etc.
Child –Please complete for any children in your household (1 child per table) First Name MI Last Name
Social Security Number(SSN)
Date of Birth Ethnicity ☐ Non-Hispanic/Non-Latino ☐ Hispanic/Latino ☐Client refused (DOB) Race ☐American Indian or Alaska Native ☐ Native Hawaiian/Pacific Islander ☐Client doesn’t know (select up to ☐Asian ☐White ☐Client Refused 2) ☐Black or African American ☐Female Gender ☐Transgender female to male ☐Client doesn’t know ☐Male (select one) ☐Doesn’t identify as male, female or transgender ☐ Client refused ☐Transgender male to female Have a disability of long duration? ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused ☐Self (head of household) ☐ Other: Non-relation member Relationship ☐ Head of Household’s Child ☐ Client doesn’t know to Head of ☐ Household Head of Household’s spouse or partner ☐ Client refused ☐ Head of Household’s other relation member ☐ Yes ☐ No If yes, enter type Covered by Health Insurance I.E. Medicaid, etc. Child –Please complete for any children in your household (1 child per table) First Name MI Last Name
Social Security Number(SSN)
Page 5 of 18 Date of Birth Ethnicity ☐ Non-Hispanic/Non-Latino ☐ Hispanic/Latino ☐Client refused (DOB) Race ☐American Indian or Alaska Native ☐ Native Hawaiian/Pacific Islander ☐Client doesn’t know (select up to ☐Asian ☐White ☐Client Refused 2) ☐Black or African American ☐Female Gender ☐Transgender female to male ☐Client doesn’t know ☐Male (select one) ☐Doesn’t identify as male, female or transgender ☐ Client refused ☐Transgender male to female Have a disability of long duration? ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused ☐Self (head of household) ☐ Other: Non-relation member Relationship ☐ Head of Household’s Child ☐ Client doesn’t know to Head of ☐ Household Head of Household’s spouse or partner ☐ Client refused ☐ Head of Household’s other relation member ☐ Yes ☐ No If yes, enter type Covered by Health Insurance I.E. Medicaid, etc.
Child –Please complete for any children in your household (1 child per table) First Name MI Last Name
Social Security Number(SSN)
Date of Birth Ethnicity ☐ Non-Hispanic/Non-Latino ☐ Hispanic/Latino ☐Client refused (DOB) Race ☐American Indian or Alaska Native ☐ Native Hawaiian/Pacific Islander ☐Client doesn’t know (select up to ☐Asian ☐White ☐Client Refused 2) ☐Black or African American ☐Female Gender ☐Transgender female to male ☐Client doesn’t know ☐Male (select one) ☐Doesn’t identify as male, female or transgender ☐ Client refused ☐Transgender male to female Have a disability of long duration? ☐ Yes ☐ No ☐Client doesn’t know ☐Client refused ☐Self (head of household) ☐ Other: Non-relation member Relationship ☐ Head of Household’s Child ☐ Client doesn’t know to Head of ☐ Household Head of Household’s spouse or partner ☐ Client refused ☐ Head of Household’s other relation member ☐ Yes ☐ No If yes, enter type Covered by Health Insurance I.E. Medicaid, etc. Please Note: UYSS offers financial assistance only twice in one year to the same candidate.
Referral Source: _____Agency ____Self ____Family ____Friend ____Other _____Powerhouse _____FHA _____Rebuilding Together _____Probation _____DHHS Agency/Representative Name:______Grant Amount Requested:______Name of who to make the check payable to: ______Title (landlord, etc.): ______Phone: ______Address: ______Additional Information: ______
Are you affiliated with a church?______Would you like to be?______
**If requesting transportation assistance, you must provide proof of ALL of the following**
_____Driver’s License _____Proof of Insurance _____Registration
To verify gap in services, please explain why the following agencies are unable to provide assistance: ___General Assistance (402-727-2731): (results) ______Salvation Army Church (402-721-0930): (results) ______Low Income Ministry (402-727-6884): (results) ______NENCAP (402-721-0619): (results)______
Please provide one of the following forms of identification: _____Photo ID _____SS Card _____Other
What is the hardship that threatens your housing stability? ______
What do you think would happen to your housing stability if you were not granted funds at this time? ______
I am requesting funds from UYSS as a solution to a hardship and agree that the resources will go directly to the solution and not to me. I agree to allow UYSS to track my progress for one year.
Signature:______Date: ______Printed Name: ______UYSS Representative: ______
Page 7 of 18 Family # or HMIS #:
Number in Household:______
Date: Income Current Projected SNAP $ Income earned from any type of work Child Support ADC Alimony Financial Aid for schooling Social Security - SSDI SSI Other: Other:
Total Net Income
MONTHLY LIVING EXPENSES Expense Current Projected Expense Current Projected SAVINGS FAMILY Emergency Plan Life Insurance** HOUSING Day Care/Baby Sitting Rent/Mortgage Allowance/Spending Money 2nd Mortgage/Mobile Home Space Alimony/Child Support** Property Tax CLOTHING Renters/Homeowners Ins For the Family Home Furnishings Laundry Repairs & Improvements PERSONAL UTILITIES Hair Cut/ Nails Electricity/Gas/Water Toiletries/Cosmetics Trash Tobacco/Alcohol/Drugs FOOD ENTERTAINMENT Groceries/Household Supplies Movie Rentals/Netflix/Hulu Food Bought at Work Dining Out School Lunches Sports/Hobbies TRANSPORTATION Vacations Car Payment #1 BUNDLED SERVICES-List here------> Or list invidiually below Car Payment #2 Phone/Cell Phone Gasoline Cable/Satellite Auto Insurance Internet Maintenance/Tires EDUCATION Registration/Licenses Tuition/School Expense (if not covered by financial aid) Parking/Carpool Music or Other Lessons HEALTH CARE Student Loans Health Insurance** MISC Doctor/Dentist/Eye Care Pet Care Prescriptions Other Debts/Garnishments Other Other:
** T o b e c o u n te d O NLY if th is w a s n o t a lre a d y s u b tra c te d Total Expenses $ fro m yo u r in c o m e . Net Monthly Income $
Income - Expenses
Page 8 of 18 Page 9 of 18 I ______understand information about me and/or my dependents listed below is entered into a database system called ServicePoint. This system helps to better understand homelessness, to improve service delivery and to evaluate the effectiveness of services provided. Participation in data collection is a critical component of our community’s ability to provide the most effective services and housing possible. The information that is collected is protected by limiting access to the database and limiting what information may be shared. Access to the data and sharing of the data is in compliance with the standards set by the federal, state and local regulations governing confidentially of client records. Every person and agency that is authorized to read or enter information into the system has signed an agreement to maintain the security and confidentiality of the information.
By signing this form, I authorize the following: The information collected by this agency will be included in ServicePoint and only partner agencies, which have entered into an HMIS Agency Participation Agreement, may be used to:
Produce a client profile at intake that will be shared with collaborating agencies
Produce aggregate level reports regarding use of services
Track individual program-level outcomes
Identify unfilled service needs and plan for enhancements
Allocate resources among agencies engaged in services
By signing this form, I authorize the following: I authorize the partner agencies and their representatives to share basic information regarding my family members listed below and/or me. I understand that this information is for the purpose of assessing my/our needs for housing, utility assistance, food, counseling and/or other services.
The information may consist of the following PPI (Personal Protected Information):
Name Homeless History Disabling Condition Date of Birth Family Composition Photo (if applicable) Social Security Number Income/Non-cash Housing information Gender Veteran Status Health Insurance Status Ethnicity and Race Domestic Violence Client Location Residence Prior to Project Entry VI-SPDAT
I Understand That:
The partner agencies have signed agreements to treat my information in a professional and confidential manner. I have the right to view the client confidentiality polices used by the HMIS partner agencies
Staff members of the partner agencies who will see my information have signed agreements to maintain confidentiality regarding my information.
Page 10 of 18 The release of my information does not guarantee that I will receive assistance; my refusal to authorize the use of my information does not disqualify me from receiving assistance.
My records are protected by federal, state, and local regulations governing confidentially of client records and cannot be disclosed without my written consent unless otherwise provided for in the regulations.
This authorization will remain in effect until I revoke it in writing, and I may revoke authorization at any time, if I revoke my authorization, all information about me already in the database will remain.
This release if valid for __1____ years from the date of my signature below.
I understand I may withdraw my consent at any time.
Partner Agencies: A list of the partner agencies within the Nebraska Homeless Management Information System may be viewed prior to signing this form.
List all Dependent Children under 18 in the household, if any (first, last and DOB) 1. 2. 3. 4. 5. 6. 7. 8.
Auditors or funders who have legal rights to review the work of this agency, including the U.S. Department of Housing and Urban Development and Nebraska Department of Health and Human Services Homeless Assistance Program may see my complete file in HMIS if services received are funded by their Department/s.
Please initial one of the following levels of consent:
___ I give authorization for me and my dependents listed above, Protected Personal and relevant Information to be entered into the NMIS and shared between Partner Agencies.
Or
___I do not consent to the inclusion of personal information in the NMIS about me and any dependents listed above.
______Consumer’s Signature Date
______Agency Staff Name(print) Agency Staff Signature Date
Page 11 of 18 Page 12 of 18 Nebraska Balance of State Management Information System Collaborative Interagency Data Sharing Agreement Attachment B – Client Release of Information Form or Interagency Sharing
BOS-MIS Release of Information for agency shared data (ROI) Only complete this form if you have in place a CS-MIS shared agency agreement and will share CS-MIS data with other service providers in the community and have the NMIS Release of Information form signed by the client.
1. Client name: ______ServicePoint ID: ______
2. Do you want to include all household members in this ROI? Yes No
If no: Exclude these household members from this ROI: ______
3. Which provider is entering this Release of Information? Uniquely Yours Stability Support, Inc. Select the highest level in the agency; i.e., if the client is served by Lincoln Action Program Housing and Resource Counseling Program, then indicate Lincoln Action Program.
4. Was the release granted by the client? Yes No A “yes” will share the client’s data with other agencies. A “no” will not share any of the client’s data with other agencies. Data will still be entered into CS-MIS for the providing agency.
5. ROI Start Date: _____ /_____/ ______End Date (one year from start): _____ /_____/ ______Month Day Year Month Day Year
6. Please select the form of documentation that authorizes this ROI:
Signed statement from client Verbal consent
(If needed): Witness: ______
Information to be made available to client for this ROI:
Client has the right to be provided a hard copy of the agency Privacy Notification Policy and a listing of other agencies that their data is shared with.
The client should be informed that the data is shared for several reasons in the community including to provide coordinated services that should result in more needs being met, reduce the amount of time and number of times the client is required to provide each provider their particular information and circumstances, and to provide unduplicated counts of persons needing services in the community.
Balance of State Provider Interagency Shared Data Agreement Page 13 of 18 Page 14 of 18 Page 15 of 18 Page 16 of 18 Initial Case Management Notes
Date: ______Client Full Name: ______HMIS#:______CL#:______
UYSS Rep: ______Requested Service(s):______Outcome:______
Referrals:______
Protective Factor Survey Referrals -Counseling, Boys Town Family Support Services, Heartland Family Services, Lutheran Family Services, The Bridge, Nebraska Family Advantage, Community Response, Life Choices, Three Rivers Public Health, Good Neighbor. -Community events, Community Cafes, support groups, Getting Ahead in a Just-Gettin’-By World, Project Everlast, YMCA, Hope Center for Kids, Pathfinder Support Services, UYSS support groups. Food pantries & community meals, Churches to establish faith-based relationship. -Low Income Ministry, Salvation Army, NENCAP, Care Corps, Rebuilding Together, UYSS Life Skills, staffing agencies, Voc Rehab, ResCare, DHHS Economic Assistance, HealthCare Market Place and Medicaid, General Assistance, low-income housing. MOPS, Early Steps to School Success, Parents Interacting With Infants. Follow-up appointment for Case Management/CRN: (Yes / No) Date: ______With: ______Notes:______
Case Management Notes Update: Date: ______UYSS Rep: ______HMIS: ______CL#: ______Need:______NOTES:______
Page 17 of 18 ______Outcome: ______New Referrals:______Action Plan: ______Follow-up appointment for Case Management/CRN: (Yes / No) Date: ______With: ______Notes:______
Case Management Notes Update: Date: ______UYSS Rep: ______HMIS: ______CL#: ______Need:______NOTES:______Outcome: ______New Referrals:______Action Plan: ______Follow-up appointment for Case Management/CRN: (Yes / No) Date: ______With: ______Notes:______
Page 18 of 18