MRN ______
Name ______
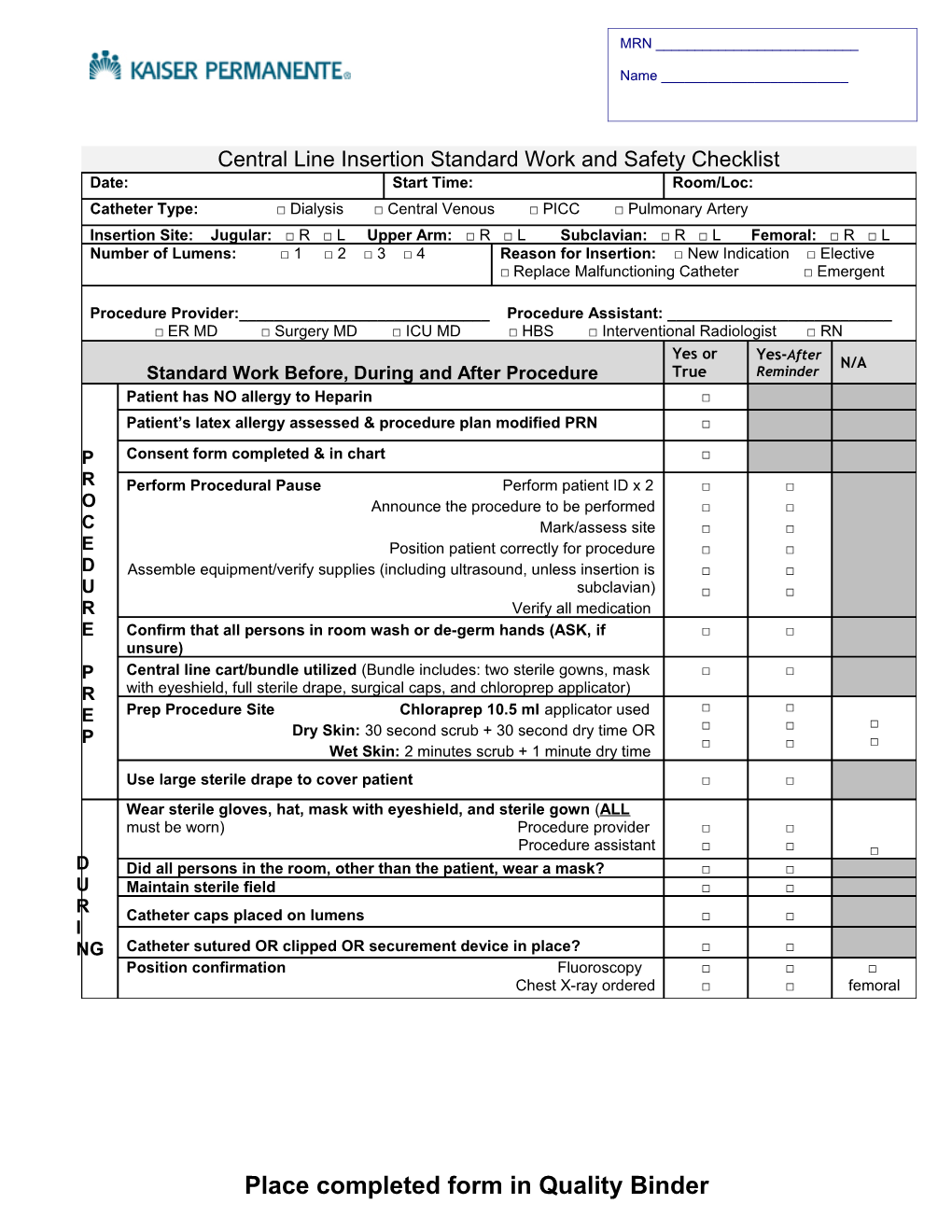
Central Line Insertion Standard Work and Safety Checklist Date: Start Time: Room/Loc: Catheter Type: □ Dialysis □ Central Venous □ PICC □ Pulmonary Artery Insertion Site: Jugular: □ R □ L Upper Arm: □ R □ L Subclavian: □ R □ L Femoral: □ R □ L Number of Lumens: □ 1 □ 2 □ 3 □ 4 Reason for Insertion: □ New Indication □ Elective □ Replace Malfunctioning Catheter □ Emergent
Procedure Provider:______Procedure Assistant: ______□ ER MD □ Surgery MD □ ICU MD □ HBS □ Interventional Radiologist □ RN Yes or Yes-After N/A Standard Work Before, During and After Procedure True Reminder Patient has NO allergy to Heparin □ Patient’s latex allergy assessed & procedure plan modified PRN □ P Consent form completed & in chart □ R Perform Procedural Pause Perform patient ID x 2 □ □ O Announce the procedure to be performed □ □ C Mark/assess site □ □ E Position patient correctly for procedure □ □ D Assemble equipment/verify supplies (including ultrasound, unless insertion is □ □ U subclavian) □ □ R Verify all medication E Confirm that all persons in room wash or de-germ hands (ASK, if □ □ unsure) P Central line cart/bundle utilized (Bundle includes: two sterile gowns, mask □ □ R with eyeshield, full sterile drape, surgical caps, and chloroprep applicator) Prep Procedure Site Chloraprep 10.5 ml applicator used □ □ E □ Dry Skin: 30 second scrub + 30 second dry time OR □ □ P □ □ □ Wet Skin: 2 minutes scrub + 1 minute dry time Use large sterile drape to cover patient □ □ Wear sterile gloves, hat, mask with eyeshield, and sterile gown (ALL must be worn) Procedure provider □ □ Procedure assistant □ □ □ D Did all persons in the room, other than the patient, wear a mask? □ □ U Maintain sterile field □ □ R Catheter caps placed on lumens □ □ I NG Catheter sutured OR clipped OR securement device in place? □ □ Position confirmation Fluoroscopy □ □ □ Chest X-ray ordered □ □ femoral
Place completed form in Quality Binder