An Evaluation of Community-Based Surveillance in the Northern Region of Ghana (Final 27-Oct-2000)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
2021-2024 Budget Preparation Guidelines
2021-2024 Budget Preparation Guidelines AUGUST, 2020 2021-2024 Budget Preparation Guidelines Table of Contents Acronyms and Abbreviations ...................................................................................... ii SECTION ONE: INTRODUCTION .................................................................................. 1 Medium-Term Development Policies ........................................................................... 1 The Economic Outlook of the Country (2021 Fiscal Framework) ................................. 2 SECTION TWO: INSTRUCTIONS FOR PREPARING THE 2021-2024 BUDGET ......... 5 Programme Based Budgeting (PBB) ........................................................................... 5 MDAs 2021 Budget Hearings ....................................................................................... 7 Revenue Management ................................................................................................. 7 Budgeting for Compensation of Employees ................................................................. 8 Budgeting for Goods and Services .............................................................................. 9 Budgeting for Capital Expenditure (CAPEX) ................................................................ 9 Other Budget Preparation Issues ............................................................................... 12 SECTION THREE: SPECIFIC INSTRUCTIONS FOR REGIONAL COORDINATING COUNCILS (RCCs) AND MMDAs............................................................................... -

North East Gonja District Assembly
Table of Contents PART A: STRATEGIC OVERVIEW ................................................................................ 3 1. ESTABLISHMENT OF THE DISTRICT .................................................................... 3 2. VISION ..................................................................................................................... 3 3. MISSION .................................................................................................................. 3 4. GOALS ..................................................................................................................... 3 5. CORE FUNCTIONS ................................................................................................. 3 6. DISTRICT ECONOMY .............................................................................................. 4 7. KEY ACHIEVEMENTS IN 2020 ............................................................................... 6 8. REVENUE AND EXPENDITURE PERFORMANCE ................................................ 7 9. NMTDF POLICY OBJECTIVES IN LINE WITH SDGs AND TARGETS AND COST 9 10. POLICY OUTCOME INDICATORS AND TARGETS .......................................... 10 PART B: BUDGET PROGRAMME/SUB-PROGRAMME SUMMARY ......................... 11 PROGRAMME 1: MANAGEMENT AND ADMINISTRATION ................................... 11 PROGRAMME 2: INFRASTRUCTURE DELIVERY AND MANAGEMENT .............. 24 PROGRAMME 3: SOCIAL SERVICES DELIVERY .................................................. 30 PROGRAMME 4: ECONOMIC DEVELOPMENT -

A Consociational Analysis of the Experiences of Ghana in West Africa (1992-2016) Halidu Musah
Democratic Governance and Conflict Resistance in Conflict-prone Societies : A Consociational Analysis of the Experiences of Ghana in West Africa (1992-2016) Halidu Musah To cite this version: Halidu Musah. Democratic Governance and Conflict Resistance in Conflict-prone Societies : A Conso- ciational Analysis of the Experiences of Ghana in West Africa (1992-2016). Political science. Université de Bordeaux, 2018. English. NNT : 2018BORD0411. tel-03092255 HAL Id: tel-03092255 https://tel.archives-ouvertes.fr/tel-03092255 Submitted on 2 Jan 2021 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. UNIVERSITÉ DE BORDEAUX THÈSE PRÉSENTÉE POUR OBTENIR LE GRADE DE DOCTEUR EN SCIENCE POLITIQUE DE L’UNIVERSITÉ DE BORDEAUX École Doctorale SP2 : Sociétés, Politique, Santé Publique SCIENCES PO BORDEAUX Laboratoire d’accueil : Les Afriques dans le monde (LAM) Par: Halidu MUSAH TITRE DEMOCRATIC GOVERNANCE AND CONFLICT RESISTANCE IN CONFLICT-PRONE SOCIETIES: A CONSOCIATIONAL ANALYSIS OF THE EXPERIENCES OF GHANA IN WEST AFRICA (1992-2016) (Gouvernance démocratique et résistance aux conflits dans les sociétés enclines aux conflits: Une analyse consociationnelle des expériences du Ghana en Afrique de l'Ouest (1992-2016)). Sous la direction de M. Dominique DARBON Présentée et soutenue publiquement Le 13 décembre 2018 Composition du jury : M. -

The Composite Budget of the East Gonja District Assembly for the 2015
REPUBLIC OF GHANA THE COMPOSITE BUDGET OF THE EAST GONJA DISTRICT ASSEMBLY FOR THE 2015 FISCAL YEAR 1 For Copies of this MMDA’s Composite Budget, please contact the address below: The Coordinating Director, East Gonja District Assembly Northern Region This 2015 Composite Budget is also available on the internet at: www.mofep.gov.gh or www.ghanadistricts.com 2 TABLE OF CONTENTS SECTION I: ASSEMBLY’S COMPOSITE BUDGET STATEMENT BACKGROUND Establishment of the District Assembly.............................................................................................................7 The Structure of theAssembly..........................................................................................................................7 Vision of the District........................................................................................................................................7 Mission Statement............................................................................................................................................8 The Values ……………………………………………………………………………………………………………………………………………………8 Objectives ……………………………………………………………………………………………………………………………………………………8 Location...........................................................................................................................................................9 Climate.............................................................................................................................................................9 Vegetation .....................................................................................................................................................10 -
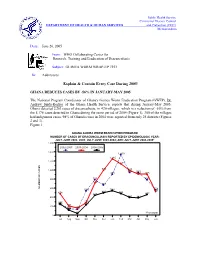
Explain & Contain Every Case During 2005!
Public Health Service Centers for Disease Control DEPARTMENT OF HEALTH & HUMAN SERVICES and Prevention (CDC) Memorandum Date: June 20, 2005 From: WHO Collaborating Center for Research, Training and Eradication of Dracunculiasis Subject: GUINEA WORM WRAP-UP #153 To: Addressees Explain & Contain Every Case During 2005! GHANA REDUCES CASES BY -56% IN JANUARY-MAY 2005 The National Program Coordinator of Ghana's Guinea Worm Eradication Program (GWEP), Dr. Andrew_Seidu-Korkor of the Ghana Health Service, reports that during January-May 2005, Ghana detected 2,263 cases of dracunculiasis, in 420 villages, which is a reduction of -56% from the 5,176 cases detected in Ghana during the same period of 2004 (Figure 1). 300 of the villages had indigenous cases. 98% of Ghana's cases in 2004 were reported from only 25 districts (Figures 2 and 3). Figure 1 GHANA GUINEA WORM ERADICATION PROGRAM NUMBER OF CASES OF DRACUNCULIASIS REPORTED BY EPIDEMIOLOGIC YEAR: JULY-JUNE 2002- 2003; JULY-JUNE 2003-2004; AND JULY-JUNE 2004-2005* 1,600 2002-2003 2003-2004 2004-2005 1,400 1,339 1,245 1,200 1,133 996 990 1,000 944 940 903 907 905 800 785 785 712 665 NUMBER OF CASES 600 558 539 544 520 474 496 482 439 457 400 393 387 257 278 234 230 203 200 142 158 115 131 38 *Provisional 0 Jul Aug Sept Oct Nov Dec Jan Feb Mar Apr May Jun Two districts, Nkwanta (Volta Region) and Tolon-Kumbungu (Northern Region), that together reported 35% of Ghana's cases in 2004, have recorded reductions of -90% (from 1,006 to 97 cases) and -11% (from 452 to 404 cases), respectively, in cases during Jan. -

Traditional Practices, Knowledge and Perceptions of Fire Use in a West African Savanna 2 Parkland 3 4 Esther Ekua Amoako1, 2*, James Gambiza1
bioRxiv preprint doi: https://doi.org/10.1101/2020.09.24.311209; this version posted September 24, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. 1 Title: Traditional practices, knowledge and perceptions of fire use in a West African savanna 2 parkland 3 4 Esther Ekua Amoako1, 2*, James Gambiza1 5 1Department of Environmental Science, Rhodes University, P.O. Box 94, Grahamstown, South Africa 6 2Department of Ecotourism and Environmental Management, University for Development Studies, 7 P.O. Box 1882 Tamale, Ghana 8 *Corresponding author: E-mail address: [email protected] (Esther Ekua Amoako) 9 Abstract 10 Understanding people’s fire practices, knowledge and perceptions of the use of fire and fire regimes 11 can inform fire management plans that could contribute to sustainable savanna conservation and 12 management. We investigated the frequency of fire use, control and perceptions of fire regime for 13 selected livelihood and socio-cultural activities in six districts in the Guinea savanna of Ghana. The 14 majority of respondents (83%) across the study districts indicated that they used fire once a year for at 15 least one of the following activities: land preparation, weed/grass/pest control, burning stubble after 16 harvest, bush clearing around homesteads, firebreaks, charcoal burning and hunting. The study showed 17 a higher frequency of fire use in the dry season for land preparation for cropping. Less than a fifth of 18 the respondents (17%) indicated that they do not use fire for any of the above activities. -

2021 PES Field Officer's Manual Download
2021 POPULATION AND HOUSING CENSUS POST ENUMERATION SURVEY (PES) FIELD OFFICER’S MANUAL STATISTICAL SERVICE, ACCRA July, 2021 1 Table of Content LIST OF ABBREVIATIONS ..................................................................................... 11 INTRODUCTION ........................................................................................................ 12 CHAPTER 1 ................................................................................................................. 13 1. THE CONCEPT OF PES AND OVERVIEW OF CENSUS EVALUATION ........................ 13 1.1 What is a Population census? .................................................................................................. 13 1.2 Why are we conducting the Census? ...................................................................................... 13 1.3. Census errors .............................................................................................................................. 13 1.3.1. Omissions ................................................................................................................................. 14 1.3.2. Duplications ............................................................................................................................. 14 1.3.3. Erroneous inclusions ............................................................................................................... 15 1.3.4. Gross versus net error ............................................................................................................ -
Nanumba North District Assembly
REPUBLIC OF GHANA THE COMPOSITE BUDGET OF THE NANUMBA NORTH DISTRICT ASSEMBLY FOR THE 2014 FISCAL YEAR Contents SECTION I: ASSEMBLY’S COMPOSITE BUDGET STATEMENT The District Assembly …................................................................................... 1 Location And Size ............................................................................................ 1 Topography and Drainage................................................................................. 2 Climate and Vegetation .................................................................................... 3 Human Settlement ……………............................................................................. 3 Demographic Characteristics ……….................................................................... 4 Economic Activity and Poverty……………………….................................................. 4 Strategic Direction, 2014-2016 ………………………………......................................... 5 Status of Implementation of Budget 2012 and 2013 …………………...................... 6 Summary of 2012 and 2013 Budget ………......................................................... 7 Achievements 2013 ………………………………………………........................................ 8 Challenges and Constraints ………………………………..…………………....................... 8 Budget 2014 ………………………………………......................................................... 10 Assumptions Underlying Budget Formulation…………......................................... 10 Revenue Improvement Strategies for 2014 …………………………......................... -

8 October, 2018 John Mahama Must Apol
PRESS CONFERENCE BY THE REGIONAL COMMUNICATIONS DIRECTORATE OF THE NEW PATRIOTIC PARTY – 8th OCTOBER, 2018 JOHN MAHAMA MUST APOLOGISE TO NORTHERNERS Ladies and gentlemen of the media. First and foremost, let me thank you sincerely for honoring our invitation. As you are aware already, the former president H. E John Dramani Mahama sneaked out of his native region-Northern Region, after spending five days, touring the region to campaign for himself to be elected as the Presidential candidate of the opposition NDC. Ladies and gentlemen, the former president arrived in the region together with some of his incompetent former appointees on Tuesday, the 2nd of this month, with a truck full of lies and propaganda. In view of all these, we have invited you all here to serve as a vehicle that will convey our concerns and reservations to the former President and all well-meaning northerners that, John Mahama must apologize unconditionally to us for his recklessness by selecting wrong gears that reversed the economic progress of our region in his days as leader of the nation and largely, the consistent lies he peddled throughout his tour. PURPORTED ABONDONED ROADS The Fufulso-Sawla Road, a $157M facility was partly diverted to do the Busunu-Daboya road after taking some aspects of the contract agreement off. This contract was awarded to yet another family member of John Mahama, Mr. Peter Mahama. Today, the road that was purported to have been done under John Mahama is still not completed after squandering the allocated resources for the road. The Larabanga-Sawla stretch of the Fufulso-Sawla road has developed “manholes” after several maintenance some few years after completion (Pictures attached). -

Nanumba North District Assembly Bimbilla
NANUMBA NORTH DISTRICT ASSEMBLY BIMBILLA MEDIUM TERM DEVELOPMENT PLAN (2014-2017) (BASED ON GHANA SHARED GROWTH AND DEVELOPMENT AGENDA-GSGDA II) PREPARED BY: DISTRICT PLANNINIG COORDINATION UNIT BIMBILLA NOVEMBER 2013 10 | P a g e NANUMBA NORTH DISTRICT (2014 - 2017 MEDIUM TERM DEVELOPMENT PLAN) ACRONYMS AC AREA COUNCIL AEA AGRICULTURAL EXTENSION AGENT AIDS ACQUIRED IMMUNED DEFICIENCY SYNDROME ART ANTI RETROVIRAL THERAPY CAPS COMMUNITY ACTION PLANS CBRDP COMMUNITY BASED RURAL DEVELOPMENT PROJECT CCBT COMMUNITY CAPACITY BUILDING TEAM CHPS COMMUNITY HEALTH PLANNING SERVICES CRS CATHOLIC RELIEF SERVICES CSIR COUNCIL FOR SCIENTIFIC AND INDUSTRIAL RESEARCH CWSA COMMUNITY WATER AND SANITATION AGENCY DA DISTRICT ASSEMBLY DADU DISTRICT AGRICULTURAL DEVELOPMENT UNIT DCE DISTRICT CHIEF EXECUTIVE DDF DISTRICT DEVELOPMENT FACILITY DFR DEPARTMENT OF FEEDER ROADS DHMT DISTRICT HEALTH MANAGEMENT TEAM DMTDP DISTRICT MEDIUM TERM DEVELOPMENT PLAN DPCU DISTRICT PLANNING CO-ORDINATING UNIT DWAP DISTRICT WIDE ASSISTANCE PROJECT EHU ENVIRONMENTAL HEALTH UNIT EU EUROPEAN UNION 11 | P a g e NANUMBA NORTH DISTRICT (2014 - 2017 MEDIUM TERM DEVELOPMENT PLAN) GDO GENDER DESK OFFICER GES GHANA EDUCATION SERVICE GSGDA GHANA SHARED GROWTH AND DEVELOPMENT AGENDA GOG GOVERNMENT OF GHANA GPRS II GROWTH AND POVERTY REDUCTION STRATEGY HIV HUMAN IMMUNED VIRUS JHS JUNIOJR HIGH SCHOOL KVIP KUMASI VENTILATED IMPROVED PIT LI LEGISLATIVE INSTRUMENT M&E MONITORING AND EVALUATION MOE MINISTRY OF ENERGY MOFA MINISTRY OF FOOD AND AGRICULTURE MTDP MEDIUM TERM DEVELOPMENT PLAN NDPC -

National Forest Forum
CIVIC RESPONSE NATIONAL FOREST FORUM REPORT OF THE NATIONAL FOREST FORUM HELD AT MIKLIN HOTEL, ACCRA SEPTEMBER 5 -9, 2011 2011 National Forest Forum Report (September 5-9, 2011) 1 ABBREVIATIONS AND ACRONYMS AFB African Foresters Brigade CFC Community Forest Committee CRMU Collaborative Resources Management Unit DCE District Chief Executives DOLTA Domestic Lumber Trade Association FAO Food and Agriculture Organization FC Forestry Commission FFC Forest Fringe Communities FLEGT Forest Law Enforcement, Governance and Trade FSD Forest Service Division GoG Government of Ghana IGF Internally Generated Funds KWC Kumasi Wood Cluster Association LAS Legality Assurance System MOFA Ministry of Food and Agriculture OASL Office of Administrator of Stool lands RMSC Resource Management Support Centre SRA Social Responsibility Agreement TVD Timber Verification Division VPA Voluntary Partnership Agreements WTS Wood Tracking System 2 2011 National Forest Forum Report (September 5-9, 2011) Table of Contents 1.0 INTRODUCTION 5 1.1 Workshop Objectives 5 1.2 Workshop Methodology and Presentations 5 1.3 Opening Session and participants Expectations 5 2.0 WORKING SESSIONS ON NEW FOREST INITIATIVES 7 2.1. Update on the Implementation of the Ghana-EU VPA 7 2.1.1 Forum Discussion and Recommendations on the VPA 8 2.2 Status of Forestry Sector Policy Reform and Initiatives 9 2.2.1 Revised Forest and Wildlife Policy 9 2.2.2 Update on the implementation of the National forestation programme 9 2.2.3 Forum Discussions and Conclusions on Plantation Development 11 2.2.5 -

Ministry of Health
REPUBLIC OF GHANA MEDIUM TERM EXPENDITURE FRAMEWORK (MTEF) FOR 2021-2024 MINISTRY OF HEALTH PROGRAMME BASED BUDGET ESTIMATES For 2021 Transforming Ghana Beyond Aid REPUBLIC OF GHANA Finance Drive, Ministries-Accra Digital Address: GA - 144-2024 MB40, Accra - Ghana +233 302-747-197 [email protected] mofep.gov.gh Stay Safe: Protect yourself and others © 2021. All rights reserved. No part of this publication may be stored in a retrieval system or Observe the COVID-19 Health and Safety Protocols transmitted in any or by any means, electronic, mechanical, photocopying, recording or otherwise without the prior written permission of the Ministry of Finance Get Vaccinated MINISTRY OF HEALTH 2021 BUDGET ESTIMATES The MoH MTEF PBB for 2021 is also available on the internet at: www.mofep.gov.gh ii | 2021 BUDGET ESTIMATES Contents PART A: STRATEGIC OVERVIEW OF THE MINISTRY OF HEALTH ................................ 2 1. NATIONAL MEDIUM TERM POLICY OBJECTIVES ..................................................... 2 2. GOAL ............................................................................................................................ 2 3. VISION .......................................................................................................................... 2 4. MISSION........................................................................................................................ 2 5. CORE FUNCTIONS ........................................................................................................ 2 6. POLICY OUTCOME