Gi-Map® Interpretive Guide Content
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Food Poisoning Toxins of Bacillus Cereus
toxins Review The Food Poisoning Toxins of Bacillus cereus Richard Dietrich 1,†, Nadja Jessberger 1,*,†, Monika Ehling-Schulz 2 , Erwin Märtlbauer 1 and Per Einar Granum 3 1 Department of Veterinary Sciences, Faculty of Veterinary Medicine, Ludwig Maximilian University of Munich, Schönleutnerstr. 8, 85764 Oberschleißheim, Germany; [email protected] (R.D.); [email protected] (E.M.) 2 Department of Pathobiology, Functional Microbiology, Institute of Microbiology, University of Veterinary Medicine Vienna, 1210 Vienna, Austria; [email protected] 3 Department of Food Safety and Infection Biology, Faculty of Veterinary Medicine, Norwegian University of Life Sciences, P.O. Box 5003 NMBU, 1432 Ås, Norway; [email protected] * Correspondence: [email protected] † These authors have contributed equally to this work. Abstract: Bacillus cereus is a ubiquitous soil bacterium responsible for two types of food-associated gastrointestinal diseases. While the emetic type, a food intoxication, manifests in nausea and vomiting, food infections with enteropathogenic strains cause diarrhea and abdominal pain. Causative toxins are the cyclic dodecadepsipeptide cereulide, and the proteinaceous enterotoxins hemolysin BL (Hbl), nonhemolytic enterotoxin (Nhe) and cytotoxin K (CytK), respectively. This review covers the current knowledge on distribution and genetic organization of the toxin genes, as well as mechanisms of enterotoxin gene regulation and toxin secretion. In this context, the exceptionally high variability of toxin production between single strains is highlighted. In addition, the mode of action of the pore-forming enterotoxins and their effect on target cells is described in detail. The main focus of this review are the two tripartite enterotoxin complexes Hbl and Nhe, but the latest findings on cereulide and CytK are also presented, as well as methods for toxin detection, and the contribution of further putative virulence factors to the diarrheal disease. -

The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio In
microorganisms Review The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio in the Treatment of Obesity and Inflammatory Bowel disease Spase Stojanov 1,2, Aleš Berlec 1,2 and Borut Štrukelj 1,2,* 1 Faculty of Pharmacy, University of Ljubljana, SI-1000 Ljubljana, Slovenia; [email protected] (S.S.); [email protected] (A.B.) 2 Department of Biotechnology, Jožef Stefan Institute, SI-1000 Ljubljana, Slovenia * Correspondence: borut.strukelj@ffa.uni-lj.si Received: 16 September 2020; Accepted: 31 October 2020; Published: 1 November 2020 Abstract: The two most important bacterial phyla in the gastrointestinal tract, Firmicutes and Bacteroidetes, have gained much attention in recent years. The Firmicutes/Bacteroidetes (F/B) ratio is widely accepted to have an important influence in maintaining normal intestinal homeostasis. Increased or decreased F/B ratio is regarded as dysbiosis, whereby the former is usually observed with obesity, and the latter with inflammatory bowel disease (IBD). Probiotics as live microorganisms can confer health benefits to the host when administered in adequate amounts. There is considerable evidence of their nutritional and immunosuppressive properties including reports that elucidate the association of probiotics with the F/B ratio, obesity, and IBD. Orally administered probiotics can contribute to the restoration of dysbiotic microbiota and to the prevention of obesity or IBD. However, as the effects of different probiotics on the F/B ratio differ, selecting the appropriate species or mixture is crucial. The most commonly tested probiotics for modifying the F/B ratio and treating obesity and IBD are from the genus Lactobacillus. In this paper, we review the effects of probiotics on the F/B ratio that lead to weight loss or immunosuppression. -
Pneumonia Types
Pneumonia Jodi Grandominico , MD Assistant Professor of Clinical Medicine Department of Internal Medicine Division of General Medicine and Geriatrics The Ohio State University Wexner Medical Center Pneumonia types • CAP- limited or no contact with health care institutions or settings • HAP: hospital-acquired pneumonia – occurs 48 hours or more after admission • VAP: ventilator-associated pneumonia – develops more than 48 to 72 hours after endotracheal intubation • HCAP: healthcare-associated pneumonia – occurs in non-hospitalized patient with extensive healthcare contact 2005 IDSA/ATS HAP, VAP and HCAP Guidelines Am J Respir Crit Care Med 2005; 171:388–416 1 Objectives-CAP • Epidemiology • Review cases: ‒ Diagnostic techniques ‒ Risk stratification for site of care decisions ‒ Use of biomarkers ‒ Type and length of treatment • Prevention Pneumonia Sarah Tapyrik, MD Assistant Professor – Clinical Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University Wexner Medical Center 2 Epidemiology American lung association epidemiology and statistics unit research and health education division. November 2015 3 Who is at Risk? • Children <5 yo • Immunosuppressed: • Adults >65 yo ‒ HIV • Comorbid conditions: ‒ Cancer ‒ CKD ‒ Splenectomy ‒ CHF • Cigarette Smokers ‒ DM • Alcoholics ‒ Chronic Liver Disease ‒ COPD Clinical Presentation • Fever • Elderly and • Chills Immunocompromised • Cough w/ purulent ‒ Confusion sputum ‒ Lethargy • Dyspnea ‒ Poor PO intake • Pleuritic pain ‒ Falls • Night sweats ‒ Decompensation of -

Family Practice
THE JOURNAL OF FAMILY ONLINE EXCLUSIVE PRACTICE Paul K. Carlton, Jr, MD, Brown recluse spider bite? FACS The Texas A&M University Consider this uniquely Health Science Center College Station, Tex conservative treatment [email protected] An antihistamine and observation work as well— and often better—than more intensive therapies. Practice recommendations oped it in 4 phases, which I describe in • Be concerned about brown recluse this article. Not only does this conser- envenomation when a patient vative approach consistently heal con- reports intensifying localized firmed brown recluse bite wounds, but pain disproportionate to physical should a bite be mistakenly attributed findings after a “bite” (C). to the brown recluse (or one of its rela- tives in the Loxosceles genus of spider), • Prescribe an oral antihistamine there is no harm to the patient, nor any alone to control symptoms, even big expense. with a necrotic wound, and mark the IN THIS ARTICLE patient’s progress over 24 hours (C). z Spider bite z Is a brown recluse • If the patient improves dramatically, to blame? or MRSA? continue the antihistamine; with little Due to limited experience among the Page E6 or no improvement, consider giving an wider medical community in identifying antibiotic with the antihistamine (C). spider envenomation,1-4 bite recognition and selection of appropriate therapy can Strength of recommendation (SOR) be difficult. A Good-quality patient-oriented evidence Early findings can be confusing. B Inconsistent or limited-quality patient-oriented evidence C Consensus, usual practice, opinion, disease-oriented Brown recluse bites typically feel like a evidence, case series pin prick. -

Peptic Ulcer Disease
Peptic Ulcer Disease orking with you as a partner in health care, your gastroenterologist Wat GI Associates will determine the best diagnostic and treatment measures for your unique needs. Albert F. Chiemprabha, M.D. Pierce D. Dotherow, M.D. Reed B. Hogan, M.D. James H. Johnston, III, M.D. Ronald P. Kotfila, M.D. Billy W. Long, M.D. Paul B. Milner, M.D. Michelle A. Petro, M.D. Vonda Reeves-Darby, M.D. Matt Runnels, M.D. James Q. Sones, II, M.D. April Ulmer, M.D., Pediatric GI James A. Underwood, Jr., M.D. Chad Wigington, D.O. Mark E. Wilson, M.D. Cindy Haden Wright, M.D. Keith Brown, M.D., Pathologist Samuel Hensley, M.D., Pathologist Jackson Madison Vicksburg 1421 N. State Street, Ste 203 104 Highland Way 1815 Mission 66 Jackson, MS 39202 Madison, MS 39110 Vicksburg, MS 39180 Telephone 601/355-1234 • Fax 601/352-4882 • 800/880-1231 www.msgastrodocs.com ©2010 GI Associates & Endoscopy Center. All rights reserved. A discovery that Table of contents brought relief to millions of ulcer What Is Peptic Ulcer Disease............... 2 patients...... Three Major Types Of Peptic Ulcer Disease .. 6 The bacterium now implicated as a cause of some ulcers How Are Ulcers Treated................... 9 was not noticed in the stomach until 1981. Before that, it was thought that bacteria couldn’t survive in the stomach because Questions & Answers About Peptic Ulcers .. 11 of the presence of acid. Australian pathologists, Drs. Warren and Marshall found differently when they noticed bacteria Ulcers Can Be Stubborn................... 13 while microscopically inspecting biopsies from stomach tissue. -

• Glycolysis • Gluconeogenesis • Glycogen Synthesis
Carbohydrate Metabolism! Wichit Suthammarak – Department of Biochemistry, Faculty of Medicine Siriraj Hospital – Aug 1st and 4th, 2014! • Glycolysis • Gluconeogenesis • Glycogen synthesis • Glycogenolysis • Pentose phosphate pathway • Metabolism of other hexoses Carbohydrate Digestion! Digestive enzymes! Polysaccharides/complex carbohydrates Salivary glands Amylase Pancreas Oligosaccharides/dextrins Dextrinase Membrane-bound Microvilli Brush border Maltose Sucrose Lactose Maltase Sucrase Lactase ‘Disaccharidase’ 2 glucose 1 glucose 1 glucose 1 fructose 1 galactose Lactose Intolerance! Cause & Pathophysiology! Normal lactose digestion Lactose intolerance Lactose Lactose Lactose Glucose Small Intestine Lactase lactase X Galactose Bacteria 1 glucose Large Fermentation 1 galactose Intestine gases, organic acid, Normal stools osmotically Lactase deficiency! active molecules • Primary lactase deficiency: อาการ! genetic defect, การสราง lactase ลด ลงเมออายมากขน, พบมากทสด! ปวดทอง, ถายเหลว, คลนไสอาเจยนภาย • Secondary lactase deficiency: หลงจากรบประทานอาหารทม lactose acquired/transient เชน small bowel เปนปรมาณมาก เชนนม! injury, gastroenteritis, inflammatory bowel disease! Absorption of Hexoses! Site: duodenum! Intestinal lumen Enterocytes Membrane Transporter! Blood SGLT1: sodium-glucose transporter Na+" Na+" •! Presents at the apical membrane ! of enterocytes! SGLT1 Glucose" Glucose" •! Co-transports Na+ and glucose/! Galactose" Galactose" galactose! GLUT2 Fructose" Fructose" GLUT5 GLUT5 •! Transports fructose from the ! intestinal lumen into enterocytes! -

Genomics 98 (2011) 370–375
Genomics 98 (2011) 370–375 Contents lists available at ScienceDirect Genomics journal homepage: www.elsevier.com/locate/ygeno Whole-genome comparison clarifies close phylogenetic relationships between the phyla Dictyoglomi and Thermotogae Hiromi Nishida a,⁎, Teruhiko Beppu b, Kenji Ueda b a Agricultural Bioinformatics Research Unit, Graduate School of Agricultural and Life Sciences, University of Tokyo, 1-1-1 Yayoi, Bunkyo-ku, Tokyo 113-8657, Japan b Life Science Research Center, College of Bioresource Sciences, Nihon University, Fujisawa, Japan article info abstract Article history: The anaerobic thermophilic bacterial genus Dictyoglomus is characterized by the ability to produce useful Received 2 June 2011 enzymes such as amylase, mannanase, and xylanase. Despite the significance, the phylogenetic position of Accepted 1 August 2011 Dictyoglomus has not yet been clarified, since it exhibits ambiguous phylogenetic positions in a single gene Available online 7 August 2011 sequence comparison-based analysis. The number of substitutions at the diverging point of Dictyoglomus is insufficient to show the relationships in a single gene comparison-based analysis. Hence, we studied its Keywords: evolutionary trait based on whole-genome comparison. Both gene content and orthologous protein sequence Whole-genome comparison Dictyoglomus comparisons indicated that Dictyoglomus is most closely related to the phylum Thermotogae and it forms a Bacterial systematics monophyletic group with Coprothermobacter proteolyticus (a constituent of the phylum Firmicutes) and Coprothermobacter proteolyticus Thermotogae. Our findings indicate that C. proteolyticus does not belong to the phylum Firmicutes and that the Thermotogae phylum Dictyoglomi is not closely related to either the phylum Firmicutes or Synergistetes but to the phylum Thermotogae. © 2011 Elsevier Inc. -

2.04.26 Fecal Analysis in the Diagnosis of Intestinal Dysbiosis and Irritable Bowel Syndrome
MEDICAL POLICY – 2.04.26 Fecal Analysis in the Diagnosis of Intestinal Dysbiosis and Irritable Bowel Syndrome BCBSA Ref. Policy: 2.04.26 Effective Date: July 1, 2021 RELATED MEDICAL POLICIES: Last Revised: June 8, 2021 None Replaces: N/A Select a hyperlink below to be directed to that section. POLICY CRITERIA | DOCUMENTATION REQUIREMENTS | CODING RELATED INFORMATION | EVIDENCE REVIEW | REFERENCES | HISTORY ∞ Clicking this icon returns you to the hyperlinks menu above. Introduction Intestinal dysbiosis is a condition that occurs when the microorganisms in the digestive tract are out of balance. This condition is believed to cause diseases of the digestive tract, including poor nutrient absorption, overgrowth of certain bacteria, and irritable bowel syndrome (IBS). Symptoms of these digestive problems are similar and may include: abdominal pain, excess gas, bloating, and changes in bowel movements (constipation or diarrhea, or both). One method of diagnosing digestive disorders is by testing a fecal sample. Using fecal analysis to diagnose intestinal dysbiosis, IBS, malabsorption, or small intestinal overgrowth of bacteria is unproven (investigational). More studies are needed to see if this testing improves health outcomes. Note: The Introduction section is for your general knowledge and is not to be taken as policy coverage criteria. The rest of the policy uses specific words and concepts familiar to medical professionals. It is intended for providers. A provider can be a person, such as a doctor, nurse, psychologist, or dentist. A provider also can be a place where medical care is given, like a hospital, clinic, or lab. This policy informs them about when a service may be covered. -
Infrastructure for a Phage Reference Database: Identification of Large-Scale Biases in The
bioRxiv preprint doi: https://doi.org/10.1101/2021.05.01.442102; this version posted May 1, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. 1 INfrastructure for a PHAge REference Database: Identification of large-scale biases in the 2 current collection of phage genomes 3 4 Ryan Cook1, Nathan Brown2, Tamsin Redgwell3, Branko Rihtman4, Megan Barnes2, Martha 5 Clokie2, Dov J. Stekel5, Jon Hobman5, Michael A. Jones1, Andrew Millard2* 6 7 1 School of Veterinary Medicine and Science, University of Nottingham, Sutton Bonington 8 Campus, College Road, Loughborough, Leicestershire, LE12 5RD, UK 9 2 Dept Genetics and Genome Biology, University of Leicester, University Road, Leicester, 10 Leicestershire, LE1 7RH, UK 11 3 COPSAC, Copenhagen Prospective Studies on Asthma in Childhood, Herlev and Gentofte 12 Hospital, University of Copenhagen, Copenhagen, Denmark 13 4 University of Warwick, School of Life Sciences, Coventry, UK 14 5 School of Biosciences, University of Nottingham, Sutton Bonington Campus, College Road, 15 Loughborough, Leicestershire, LE12 5RD, 16 17 Corresponding author: [email protected] bioRxiv preprint doi: https://doi.org/10.1101/2021.05.01.442102; this version posted May 1, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. -

THE SKY IS the LIMIT for WIND POWER Wind Energy Is One of the Best Sources of Alternative Energy
Mechanical Contractors July— Sept 2018 THE SKY IS THE LIMIT FOR WIND POWER Wind energy is one of the best sources of alternative energy. Wind refers to the movement of air from high pressure areas to low pressure areas. Wind is caused by uneven heating of the earth’s surface by the sun. Hot air rises up and cool air flows in to take its place. Winds will always exist as long as solar energy exists and peo- ple will be able to harness the energy forever. Windmills have been in use since 2000 B.C. and were first developed in Persia and China. Ancient mariners sailed to distant lands by making use of winds. Farmers used wind power to pump water and for grinding grains. Today the most popular use of wind energy is converting it to electrical energy to meet the critical energy needs of the planet. It is a renewable source of energy and does not produce any pollutants or emissions during opera- tion that could harm the environment. Wind power is one of the cleanest and safest method of generating renewable electricity. Wind farms can be created to trap wind energy by placing multiple wind turbines in the same location for the purpose of generating large amounts of electric power. Wind energy is mostly harnessed by wind turbines which are as high as 20 story buildings and usually have three blades which are 60 meters long. They resemble giant airplane propellers mounted on a stick. The blades are spun by the wind which transfers motion to a shaft connected to a generator which produces electricity. -

Pancreatic Cancer
A Patient’s Guide to Pancreatic Cancer COMPREHENSIVE CANCER CENTER Staff of the Comprehensive Cancer Center’s Multidisciplinary Pancreatic Cancer Program provided information for this handbook GI Oncology Program, Patient Education Program, Gastrointestinal Surgery Department, Medical Oncology, Radiation Oncology and Surgical Oncology Digestive System Anatomy Esophagus Liver Stomach Gallbladder Duodenum Colon Pancreas (behind the stomach) Anatomy of the Pancreas Celiac Plexus Pancreatic Duct Common Bile Duct Sphincter of Oddi Head Body Tail Pancreas ii A Patient’s Guide to Pancreatic Cancer ©2012 University of Michigan Comprehensive Cancer Center Table of Contents I. Overview of pancreatic cancer A. Where is the pancreas located?. 1 B. What does the pancreas do? . 2 C. What is cancer and how does it affect the pancreas? .....................2 D. How common is pancreatic cancer and who is at risk?. .3 E. Is pancreatic cancer hereditary? .....................................3 F. What are the symptoms of pancreatic cancer? ..........................4 G. How is pancreatic cancer diagnosed?. 7 H. What are the types of cancer found in the pancreas? .....................9 II. Treatment A. Treatment of Pancreatic Cancer. 11 1. What are the treatment options?. 11 2. How does a patient decide on treatment? ..........................12 3. What factors affect prognosis and recovery?. .12 D. Surgery. 13 1. When is surgery a treatment?. 13 2. What other procedures are done?. .16 E. Radiation therapy . 19 1. What is radiation therapy? ......................................19 2. When is radiation therapy given?. 19 3. What happens at my first appointment? . 20 F. Chemotherapy ..................................................21 1. What is chemotherapy? ........................................21 2. How does chemotherapy work? ..................................21 3. When is chemotherapy given? ...................................21 G. -
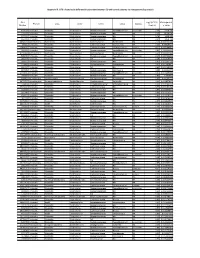
Appendix III: OTU's Found to Be Differentially Abundant Between CD and Control Patients Via Metagenomeseq Analysis
Appendix III: OTU's found to be differentially abundant between CD and control patients via metagenomeSeq analysis OTU Log2 (FC CD / FDR Adjusted Phylum Class Order Family Genus Species Number Control) p value 518372 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.16 5.69E-08 194497 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.15 8.93E-06 175761 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 5.74 1.99E-05 193709 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 2.40 2.14E-05 4464079 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 7.79 0.000123188 20421 Firmicutes Clostridia Clostridiales Lachnospiraceae Coprococcus NA 1.19 0.00013719 3044876 Firmicutes Clostridia Clostridiales Lachnospiraceae [Ruminococcus] gnavus -4.32 0.000194983 184000 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.81 0.000306032 4392484 Bacteroidetes Bacteroidia Bacteroidales Bacteroidaceae Bacteroides NA 5.53 0.000339948 528715 Firmicutes Clostridia Clostridiales Ruminococcaceae Faecalibacterium prausnitzii 2.17 0.000722263 186707 Firmicutes Clostridia Clostridiales NA NA NA 2.28 0.001028539 193101 Firmicutes Clostridia Clostridiales Ruminococcaceae NA NA 1.90 0.001230738 339685 Firmicutes Clostridia Clostridiales Peptococcaceae Peptococcus NA 3.52 0.001382447 101237 Firmicutes Clostridia Clostridiales NA NA NA 2.64 0.001415109 347690 Firmicutes Clostridia Clostridiales Ruminococcaceae Oscillospira NA 3.18 0.00152075 2110315 Firmicutes Clostridia