Yes No Yes No
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
You Never Call. You Never Write. How Many Times Have You Thought About Your Friends from College, but Didn’T Have a Clue About How to Actually Reach Them!
You never call. You never write. How many times have you thought about your friends from college, but didn’t have a clue about how to actually reach them! The NEW LU Alumni Online Community will help you get in touch. Log on today! www.lamar.edu/alumni Alumni Directory | e-mail an LU friend, update your personal data or post class notes. Groups | Reconnect with Greeks, organizations and affinity groups. News and Events | get the latest campus news and information on upcoming alumni and campus events. Career Networking | post or seek a resume, check out job postings from other alums, make business connections and mentor others. And Much More | Wallpapers and school song to personalize your desktop, message boards and chats! To register, follow the link to the Alumni Community for New User directions. Locate your user ID on the mailing label found on this page. NON-PROFIT ORG. U.S. POSTAGE LAMAR UNIVERSITY PAID Member of The Texas State University System PERMIT NO. 54 BEAUMONT, TX 77710 P.O. Box 10011 Now is the time to invest Beaumont, TX 77710 in Lamar, invest in our students, invest in the future of Southeast Texas... CadenceCARDINAL VOL. 36 NO. 2 | OCTOBER 2008 Magazine Design: Mike Rhodes From the President Cover illustration: Eugene Anderson CARDINAL DEPARTMENTS Cadence 4 On campus 32 DreamBuilders 46 Class notes 64 Arts & Culture Greetings from Lamar University, The Staff Hurricane Ike dealt a heavy blow to Southeast Texas—in particular 30 Campaign impact 37 Athletics 57 Giving report Cardinal Cadence is published by the Division of University to our coastal communities—but restoration is moving ahead. -

LAMAR UNIVERSITY PARKING LEGEND Outside Emergency Phones University Advancement 53 W Wimberly Student Services Bldg
LU BUILDING LEGEND BUILDING & PARKING MAP 2017-2018 ALPHABETICAL BLDG. NO. Admissions Visitors Center (Herman Iles Building) (C,6) . 15A Archer Building (D,2) . 55 The LU campus map is provided for reference and every effort is made for accuracy. Art (C,1). 69 Changes will occur during the course of the year. It is not intended for any official, legal or surveying use. Art House (B,2) . 63 Baptist Student Center (B,4) . 39 Barnes & Noble Bookstore (C,2) . 56 Brooks-Shivers Dining Hall (B,4). 38 Food Trucks (D-3) Campbell Hall (C,6) . 17 Campus Tours - Herman Iles Building - Admissions Visitor Center (C,6) . 15A East Lavaca Carl Parker Building (C,3) . 51 Undergraduate Advising Center University Press T1 N Center for Innovation, Commercialization, and Entrepreneurship (D,6) . 2 C-3 Port Management 72 C-5 Small Business Development Center 70 Chemistry (C,2) . 61 E. Irby St. 73 Cherry Building (D,4). 29 1 71 69 Charles & Eleanor Garrett Engineering Center A-6 Engineering Research Center Church of Christ Student Center (D,3) . 32 65 C-4 Combs Hall (A,4) . 41 64 67 Communication (B,3). 48 66 68 Disability Resource Center Caston C-2 Custodial Services (D,7) . 6 62 Dauphin Athletics Complex (F,3). 76 60 A-5 Digital Learning Center (D,7). 5 63 Dishman Art Museum (C,1). 70 61 E-1 Earth & Space Sciences (C,2). 58 59 Education (C,4) . 24 T2 Facilities Management (A,2) . 46 58 Maintenance & Operations (F,6) . 18 Jimmy Simmons Blvd. C-1 Dewey A-4 Planning & Construction (E,7) . -

New Head Coach Michelle Kuester Murielle Hlavac
2018 LAMAR UNIVERSITY VOLLEYBALL UNIVERSITY INFORMATION Location Beaumont, Texas School Founded 1923 Enrollment 14,516 (Fall 2017) Affiliation NCAA Division I Conference Southland Conference Nickname Cardinals Mascot Big Red Colors Red (Pantone 199) and White President Dr. Kenneth R. Evans Director of Athletics Marco Born Senior Woman Administrator Helene Thill ARENA INFORMATION Arena Name McDonald Gym Capacity 500 Year Opened 1958 (renovated in 2006) COACHING STAFF Head Coach Michelle Kuester Alma Mater, Year New Mexico State, 2011 Record at Lamar 0-0 (First Season) Record Overall 0-0 (First Season) Assistant Coach Chelsea Rose Alma Mater, Year New Mexico State, 2011 Graduate Assistant Amy Hollowell Alma Mater, Year Lamar University, 2018 TEAM INFORMATION PROGRAM HISTORY 2017 Overall Record 4-22 First Year of Volleyball 1973 Conference Record (Finish) 2-14 (11th) All-Time Record 962-752-9 Home Record 2-7 Conference Titles 4 New Head Coach Away Record 1-10 Conference Tourney Titles 5 Michelle Kuester Neutral Record 1-5 NCAA Appearances 5 Letterman Returning/Lost 8/6 Starting Position Player R/L 3/3 Newcomers 8 PERCENTAGE RETURNING Points 1055.5-1,326.5 (79.6%) Service Aces 64-97 (66%) Points per set 11.6 Service Aces per set 0.70 Kills 881-1072 (82.2%) Digs 656-1275 (51.5%) Kills per set 9.68 Digs per set 7.21 Assists 72-1020 (7.1%) Blocks 203-290 (70%) Assists per set 0.79 Blocks per set 2.23 TOP PLAYERS RETURNING Name SP Pts K K/S A A/S SA SA/S D D/S B B/S Tomar Thomas 77 318.5 282 3.66 3 0.04 15 0.19 58 0.75 37.0 0.48 Murielle Hlavac 88 221.5 199 2.26 16 0.18 11 0.13 258 2.93 23.0 0.26 Dannisha House 85 189.0 157 1.85 4 0.05 5 0.06 31 0.36 49.0 0.58 Ivette Dim 60 184.0 147 2.45 1 0.02 1 0.02 30 0.50 65.0 1.08 Murielle Hlavac Zahria Scott 89 27.0 0 0.00 42 0.47 27 0.30 225 2.53 0 0.00 2018 LAMAR UNIVERSITY VOLLEYBALL 2018 ROSTER # Name Pos. -

2019 Lamar University Volleyball Quick Facts
2019 LAMAR UNIVERSITY VOLLEYBALL QUICK FACTS UNIVERSITY INFORMATION Location Beaumont, Texas School Founded 1923 Enrollment 14,783 (Spring 2019) Affiliation NCAA Division I Conference Southland Conference Nickname Cardinals Mascot Big Red Colors Red (Pantone 199) and White President Dr. Kenneth R. Evans Director of Athletics Marco Born Senior Woman Administrator Helene Thill ARENA INFORMATION Arena Name McDonald Gym Capacity 500 Year Opened 1958 (renovated in 2006 and 2018) COACHING STAFF Head Coach Michelle Kuester Alma Mater, Year New Mexico State, 2011 Record at Lamar 7-20 (Second Season) Record Overall 7-20 (Second Season) Assistant Coach Haley Eckerman Alma Mater, Year University of Texas, 2017 Graduate Assistant Amy Hollowell Alma Mater, Year Lamar University, 2018 TEAM INFORMATION PROGRAM HISTORY 2018 Overall Record 7-20 First Year of Volleyball 1973 Conference Record (Finish) 4-12 (11th) All-Time Record 969-722-9 Home Record 6-5 Conference Titles 4 Michelle Kuester Away Record 1-12 Conference Tourney Titles 5 Head Coach Neutral Record 0-3 NCAA Appearances 5 Letterman Returning/Lost 7/8 Starting Position Player R/L 3/3 Newcomers 9 PERCENTAGE RETURNING Points 696-1,380.5 (50.4%) Service Aces 51-127 (40.2%) Points per set 13.94 Service Aces per set 1.28 Kills 562-1101 (51.0%) Digs 654-1120 (58.4%) Kills per set 11.12 Digs per set 11.31 Assists 407-1023 (39.8%) Blocks 143-152.5 (93.8%) Assists per set 10.33 Blocks per set 1.54 TOP PLAYERS RETURNING Name SP Pts K K/S A A/S SA SA/S D D/S B B/S Abigale Nash 82 180.0 156 1.90 19 0.23 18 0.22 193 2.35 11.0 0.13 Bre’Ala Box 91 168.5 131 1.44 9 0.10 12 0.13 47 0.52 44.0 0.48 Haley Eckerman Alyssa Legette 79 22.5 8 0.10 407 5.15 14 0.18 110 1.39 1.0 0.01 Erin Pequeno 81 2.5 0 0.00 54 0.67 2 0.02 239 2.95 1.0 0.01 Assistant Coach Dannisha House 83 154.0 122 1.47 2 0.02 7 0.08 36 0.43 42.0 0.51 2019 ROSTER # Name Pos. -

LAMAR UNIVERSITY PARKING LEGEND Outside Emergency Phones University Advancement 53 W Wimberly Student Services Bldg
LU BUILDING LEGEND BUILDING & PARKING MAP 2017-2018 ALPHABETICAL BLDG. NO. Admissions Visitors Center (Herman Iles Building) (C,6) . 15A Archer Building (D,2) . 55 The LU campus map is provided for reference and every effort is made for accuracy. Art (C,1). 69 Changes will occur during the course of the year. It is not intended for any official, legal or surveying use. Art House (B,2) . 63 Baptist Student Center (B,4) . 39 Barnes & Noble Bookstore (C,2) . 56 Brooks-Shivers Dining Hall (B,4). 38 Food Trucks (D-3) Campbell Hall (C,6) . 17 Campus Tours - Herman Iles Building - Admissions Visitor Center (C,6) . 15A East Lavaca Carl Parker Building (C,3) . 51 Undergraduate Advising Center University Press T1 N Center for Innovation, Commercialization, and Entrepreneurship (D,6) . 2 C-3 Port Management 72 C-5 Small Business Development Center 70 Chemistry (C,2) . 61 E. Irby St. 73 Cherry Building (D,4). 29 1 71 69 Charles & Eleanor Garrett Engineering Center A-6 Engineering Research Center Church of Christ Student Center (D,3) . 32 65 C-4 Combs Hall (A,4) . 41 64 67 Communication (B,3). 48 66 68 Disability Resource Center Caston C-2 Custodial Services (D,7) . 6 62 Dauphin Athletics Complex (F,3). 76 63 60 A-5 Digital Learning Center (D,7). 5 61 Dishman Art Museum (C,1). 70 59 E-1 Earth & Space Sciences (C,2). 58 Education (C,4) . 24 T2 Facilities Management (A,2) . 46 58 Maintenance & Operations (F,6) . 18 Jimmy Simmons Blvd. C-1 Dewey A-4 Planning & Construction (E,7) . -
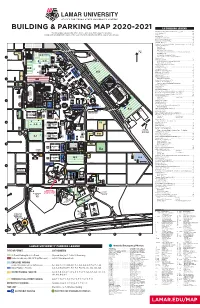
Building & Parking Map 2020-2021
BUILDING & PARKING MAP 2020-2021 LU BUILDING LEGEND Admissions Visitors Center (Herman Iles Building) (C,6) . 15A The LU campus map is provided for reference and every effort is made for accuracy. Archer Building (D,2) . 55 Changes will occur during the course of the year. It is not intended for any official, legal or surveying use. Art (C,1). 69 Art House (B,2) . 63 Baptist Student Center (B,4) . 39 Barnes & Noble Bookstore (C,2) . 56 Brooks-Shivers Dining Hall (B,4). 38 Campbell Hall (C,6) . 17 Campus Tours - Herman Iles Building - Admissions Visitor Center (C,6) . 15A Carl Parker Building (C,3) . 51 Post Office East Lavaca University Press Undergraduate Advising Center Center for Innovation, Commercialization, and Entrepreneurship (D,6) . 2 T1 N Port Management C-3 Small Business Development Center C-5 Center for Midstream Management and Science 1 70 Chemistry (C,2) . 61 E. Irby St. 71 69 73 Cherry Building (D,4). 29 C-4 A-6 Charles & Eleanor Garrett Engineering Center Engineering Research Center 65 Church of Christ Student Center (D,3) . 32 64 67 Combs Hall (A,4) . 41 66 68 Communication (B,3). 48 Caston C-2 Custodial Services (D,7) . 6 62 Dauphin Athletics Complex (F,3). 76 63 60 A-5 Digital Learning Center (D,7). 5 61 E-1 Dishman Art Museum (C,1). 70 59 Education (C,4) . 24 T2 Facilities Management (F,6) . 18 58 Maintenance & Operations 2 Jimmy Simmons Blvd. Dewey C-1 Family & Consumer Sciences (C,3) . 36 A-4 Galloway Business Building (D,2) . -
LAMAR UNIVERSITY O BEAUMONT-: C
/ LAMAR UNIVERSITY o BEAUMONT-: c. 1990-1991 TECHNICAL ARTS CATALOG LAMAR UNIVERSITY COLLEGE OF TECHNICAL ARTS 1990·91 • Bulletin • Volume 39 Number 3 Twentieth annual catalog issued with announcements for 1990-91. Founded in 1923, and established as a four-year coeducational, state supported college on Spetember 1, 1951. The provisions of this bulletin do not constitute a contract, expressed or implied, between any applicant, student, and faculty member in Lamar University. Lamar University reseJVes the right to withdraw courses at any time, change fees, calendars, curricula, graduation procedures, and any other requirement affecting stu· dents. Changes become effective when the proper authorities so determine the application to both prospective students and to the students already enrolled. For additional and complete informa· tion refer to the Lamar University General Bulletin. Lamar University is an equal opportunity/affirmative action educa tional institution and employer. Students, faculty and staff members are selected without regard to their race, color, creed, sex, or national origin, consistent with the Assurance of Compliance with Title VI of the Civil Rights Act of 1964; Executive Order 11246 as issued and amended; Title IX of the Education Amendments of 1972, as amended; Section 504 of the Rehabilitation Act of 1973. Inquiries concerning application of these regulations may be referred to the Office of the President. Bulletin of Lamar University. (USPS 074-420). Third class postage paid at Beaumont, Texas 77710. Published monthly except in June, July and August. 2 Lamar University-Technical Arts LAMAR UNIVERSITY SYSTEM BEAUMONT CAMPUS Lamar University-Technical Arts 3 LEGEND TO MAP OF LAMAR UNIVERSITY • BEAUMONT Administration (Plummer Bldg.) .•.••••••.••••••••••••• 54 Residences: Alumni House ..................................................... -
Cardinal Cadence for Web 6/04
CadenceCARDINAL From the President The Staff Whether the focus is on construction or instruction, summertime Cardinal Cadence is published by the Division of at Lamar University is a time of preparation for the approaching University Advancement, Lamar University, a member of The Texas State University System and an affirmative academic year. These months, you can find some Lamar faculty action, equal opportunity educational institution. teaching summer courses, while others are engaged in scholarly Brian Sattler, Executive Editor, Director of Public Relations Cynthia Hicks ’89, ’93, Editor activities, research or travel. Louise Wood, Writer The sounds of construction continue from the west side of Chris Castillo, Writer campus as the third phase of Cardinal Village nears completion. When the state-of- Contributors: Daucy Crizer, Amanda Rowell, writing the-art facility opens in August, it will bring Lamar’s residence hall capacity to 1,500 Allen Moore, Rohn Wenner, photography Cardinal Events 2004 students. The new 25,000-square-foot dining hall will follow in the construction Circulation includes 54,000 copies distributed to alumni, July 28-29 Sept. 13 faculty, staff and friends of Lamar University. If you have Orientation. (409) 880-8085 Nationally syndicated colum- schedule. Particularly exciting is the prospect of the renovation of McDonald Gym nist Leonard Pitts, 7 p.m. received more than one copy of this publication, please Aug. 10-11 let us know. University Theatre. Hosted by into a comprehensive fitness facility that is sure to become a center of activity for Orientation. (409) 880-8085 the College of Fine Arts and Changes of address may be sent to: Aug. -

Minutes of the Board of Regents of the Texas State
MINUTES OF THE BOARD OF REGENTS OF THE TEXAS STATE UNIVERSITY SYSTEM Quarterly Board Meeting February 20-21, 2009 Quarterly Board of Regents Meeting February 19-20, 2009 TABLE OF CONTENTS COMMITTEE MEETINGS ......................................................................................................... 1 CURRICULUM COMMITTEE .................................................................................................... 1 FINANCE AND AUDIT COMMITTEE ........................................................................................ 3 PLANNING AND CONSTRUCTION COMMITTEE ................................................................... 5 BOARD OF REGENTS MEETING .......................................................................................... 7 I. CALL TO ORDER ............................................................................................................... 7 II. ATTENDANCE ................................................................................................................... 7 III. RECESS TO EXECUTIVE SESSION ................................................................................. 7 IV. RECONVENE IN OPEN SESSION .................................................................................... 7 V. APPROVAL OF MINUTES ................................................................................................. 8 VI. CHAIRMAN’S REMARKS ................................................................................................... 8 VII. STUDENT ADVISORY BOARD REPORT -
Cadence Web 3/05
Cardinal Events 2005 April 6 April 28 College of Education Academic Reception honoring University Lecture Series presents Marlee Scholar. 2-3 p.m. University Matlin. 7:30 p.m. Montagne Center Reception Center, eighth floor, CARDINAL Gray Library April 11 Cadence Registration begins May 8 From the President The Tea Room & The Arts series April 11-24 The Staff presents Lamar Chamber Winds. High School Scholarship Exhibition. What a great weekend! Red, White & You, Homecoming and Brunch 10:30 a.m.-2 p.m. Concert at Cardinal Cadence is published by the Division of Reception 2-4 p.m. April 24. 3 p.m. Reservations required for Open House all came together into one exciting weekend on the University Advancement, Lamar University, a member of Dishman Art Museum brunch. (409) 861-1900 Lamar University campus. It was a pleasure to renew acquain- The Texas State University System and an affirmative action, equal opportunity educational institution. April 12 Student Choreography Concert. May 9-13 tances with many alumni and friends of the university. Just as Master’s Thesis Exhibition. 7:30 p.m. Rothwell Recital Hall exciting was seeing the anticipation in the eyes of thousands of Brian Sattler, Executive Editor, Director of Public Relations Reception 7-9 p.m. May 13. Cynthia Hicks ’89, ’93, Editor April 13 Dishman Art Museum prospective students and parents as they toured campus and SIXTH ANNUAL Louise Wood, Writer University Professor and Merit Award learned about opportunities at Lamar. winners announced at reception. May 11-23 Chris Castillo, Writer Summer Mini-Session The Friday evening concert was a fitting way to say “good- 2 p.m. -
Lamar Map Current
LAMAR UNIVERSITY Physical Plant N Lamar Institute of 2 M.L. King Pkwy Technology 3 4 5 14 1 E. Lavaca 10 6 7 9 11 12 13 8 15 24 16 21 23 19 18 25 17 20 22 1. Mamie McFaddin Ward 2. Dishman Art Museum 27 3. Art 26 28 4. University Theatre/KVLU 5. James M. “Jimmy” Simmons Music Building 29 and Rothwell Recital Hall irginia 6. Health & Human Performance Complex A&B E. V 7. Hayes Biology 35 31 8. Science Auditorium 30 9. Theater Arts 10. Social & Behavioral Sciences 34 32 33 11. Geology 36 12. Archer Building 40 13. Galloway Business 39 14. Montagne Center 41 42 15. Provost Umphrey Stadium, W.S. “Bud” Leonard Field and Dauphin Athletic Complex 38 16. Chemistry irginia 17. Ty Terrell Track E. V 37 18. Sheila Umphrey Recreational Sports Center and McDonald Gym 45 19. Setzer Student Center 43 46 20. Carl Parker Building Undergraduate Advising Center 21. Setzer Center Bookstore 22. Lucas Engineering 47 23. Wimberly (Admissions) Alabama 24. Visitors Parking 44 25. Plummer (Administration) 26. Communication Building 27. Post Office/Police 28. Family & Consumer Sciences 29. Mary & John Gray Library 48 30. Engineering Research Center Georgia 31. Cherry Engineering 32. Newman Catholic Center 33. Church of Christ Student Center 34. Honors Program Rolfe Christopher Rolfe 35. Latter Day Saints Student Center 49 36. Health Center Iowa 37. Combs Hall (Cardinal Village III) 38. Wesley Foundation Methodist Center 39. Baptist Student Center 52 40. Dining Hall 51 41. Texas Success Initiative/Developmental 50 Studies (former ROTC Bldg.) 42. -
Cadence Web Vol 33 11/04
Cardinal Events 2004 - 2005 Jan. 11 Feb. 26 SPRING REGISTRATION Homecoming. Events throughout the day. Basketball – Cards vs. Sam Houston Jan. 12 Feb. 26 CARDINAL CLASSES BEGIN Springfest.™ LU annual open house for Cadence Jan. 23 prospective students and their families. product From the President The Tea Room and the Arts presents (409) 880-8316 The Staff Lamar Chamber Winds. 3 p.m. This December, a record number of Lamar students joined the Art Museum of Southeast Texas. March 5-6 and is published by the Division of Cardinal Cadence Reservations required for brunch. “The Little Prince,” presented by Lamar University Advancement, Lamar University, a member of growing ranks of LU alumni as they received hard-won diplomas (10:30 a.m. - 2 p.m.). (409) 832-3432. Theatre. 2 p.m. University Theatre. The Texas State University System and an affirmative on the Montagne Center stage in one of the largest winter gradu- Tickets (409) 880-2250 potential action, equal opportunity educational institution. Jan. 24-March 3 ating classes ever. Even as they bask in the accolades of family and Dishman Competition. Reception 7-9 p.m. March 8 Lamarissimo! Jazz Bands. 7:30 p.m. Brian Sattler, Executive Editor, Director of Public Relations Jan. 16. Dishman Art Museum friends, scores of others are gaining valuable credits during the Julie Rogers Theatre. Tickets The power and reach of the Web is part of the Cynthia Hicks ’89, ’93, Editor winter mini-session or preparing for a terrific spring semester. Feb. 5 (409) 880-8144 formula students and the Institute for Louise Wood, Writer Basketball Players’ Reunion Weekend.