Cellular Pathways in Response to Ionizing Radiation and Their Targetability for Tumor Radiosensitization
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Download (1MB)
THE IN VITRO METABOLISM OF THREE ANTICANCER DRUGS by Yun Fan B.S., West China University of Medical Sciences, 1996 M.S., West China University of Medical Sciences, 2001 Submitted to the Graduate Faculty of School of Pharmacy in partial fulfillment of the requirements for the degree of Doctor of Philosophy University of Pittsburgh 2007 UNIVERSITY OF PITTSBURGH SCHOOL OF PHARMACY This dissertation was presented by Yun Fan It was defended on March 23, 2007 and approved by Samuel M. Poloyac, Assistant Professor, Pharmaceutical Sciences Raman Venkataramanan, Professor, Pharmaceutical Sciences Jack C. Yalowich, Associate Professor, Pharmacology Michael A. Zemaitis, Professor, Pharmaceutical Sciences Billy W. Day, Professor, Pharmaceutical Sciences ii Copyright © by Yun Fan 2007 iii THE IN VITRO METABOLISM OF THREE ANTICANCER DRUGS Yun Fan, Ph.D. University of Pittsburgh, 2007 Etoposide is a widely used topoisomerase II inhibitor particularly useful in the clinic for treatment of disseminated tumors, including childhood leukemia. However, its use is associated with the increased risk of development of secondary acute myelogenous leukemias. The mechanism behind this is still unclear. It was hypothesized that etoposide ortho-quinone, a reactive metabolite previously shown to be generated in vitro by myeloperoxidase, the major oxidative enzyme in the bone marrow cells from which the secondary leukemias arise, might be a contributor to the development of treatment-related secondary leukemias. Experiments showed that the glutathione adduct of etoposide ortho-quinone was formed in myeloperoxidase- expressing human myeloid leukemia HL60 cells treated with etoposide, that its formation was enhanced by addition of the myeloperoxidase substrate hydrogen peroxide, and that the glutathione adduct level was dependent on myeloperoxidase. -

Nuclear Energy in Everyday Life Nuclear Energy in Everyday Life
Nuclear Energy in Everyday Life Nuclear Energy in Everyday Life Understanding Radioactivity and Radiation in our Everyday Lives Radioactivity is part of our earth – it has existed all along. Naturally occurring radio- active materials are present in the earth’s crust, the floors and walls of our homes, schools, and offices and in the food we eat and drink. Our own bodies- muscles, bones and tissues, contain naturally occurring radioactive elements. Man has always been exposed to natural radiation arising from earth as well as from outside. Most people, upon hearing the word radioactivity, think only about some- thing harmful or even deadly; especially events such as the atomic bombs that were dropped on Hiroshima and Nagasaki in 1945, or the Chernobyl Disaster of 1986. However, upon understanding radiation, people will learn to appreciate that radia- tion has peaceful and beneficial applications to our everyday lives. What are atoms? Knowledge of atoms is essential to understanding the origins of radiation, and the impact it could have on the human body and the environment around us. All materi- als in the universe are composed of combination of basic substances called chemical elements. There are 92 different chemical elements in nature. The smallest particles, into which an element can be divided without losing its properties, are called atoms, which are unique to a particular element. An atom consists of two main parts namely a nu- cleus with a circling electron cloud. The nucleus consists of subatomic particles called protons and neutrons. Atoms vary in size from the simple hydro- gen atom, which has one proton and one electron, to large atoms such as uranium, which has 92 pro- tons, 92 electrons. -

Classification of Cell Death
Cell Death and Differentiation (2005) 12, 1463–1467 & 2005 Nature Publishing Group All rights reserved 1350-9047/05 $30.00 www.nature.com/cdd News and Commentary Classification of cell death: recommendations of the Nomenclature Committee on Cell Death G Kroemer*,1, WS El-Deiry2, P Golstein3, ME Peter4, D Vaux5, with or without, caspase activation and that ‘autophagic cell P Vandenabeele6, B Zhivotovsky7, MV Blagosklonny8, death’ represents a type of cell death with (but not necessarily W Malorni9, RA Knight10, M Piacentini11, S Nagata12 and through) autophagic vacuolization. This article details the G Melino10,13 2005 recommendations of NCCD. Over time, molecular definitions are expected to emerge for those forms of cell 1 CNRS-UMR8125, Institut Gustave Roussy, 39 rue Camille-Desmoulins, death that remain descriptive. F-94805 Villejuif, France 2 University of Pennsylvania School of Medicine, Philadelphia, PA 19104, USA Preface 3 Centre d’Immunologie INSERM/CNRS/Universite de la Mediterranee de Marseille-Luminy, Case 906, Avenue de Luminy, 13288 Marseille Cedex 9, It is obvious that clear definitions of objects that are only France shadows in Plato’s cage are difficult to be achieved. Cell death 4 The Ben May Institute for Cancer Research, University of Chicago, 924 E 57th and the different subroutines leading to cell death do not Street, Chicago, IL 60637, USA 5 escape this rule. Even worse, the notion of death is strongly Sir William Dunn School of Pathology, University of Oxford, Oxford OX1 3RE, influenced by religious and cultural beliefs, which may UK 6 Molecular Signalling and Cell Death Unit, Department for Molecular Biomedical subliminally influence the scientific view of cell death. -

Nicole Goodwin Macmillan Group Meeting April 21, 2004
Discodermolide A Synthetic Challenge Me Me Me HO Me O O OH O NH2 Me Me OH O Me Me OH Nicole Goodwin MacMillan Group Meeting April 21, 2004 Me Me Me HO Discodermolide Me O O OH O NH2 Isolation and Biological Activity Me Me OH O Me Me OH ! Isolated in 1990 by the Harbor Branch Oceanographic Institution from the Caribbean deep-sea sponge Discodermia dissoluta ! Not practical to produce discodermolide from biological sources ! 0.002% (by mass) isolation from frozen sponge ! must be deep-sea harvested at a depth in excess of 33 m ! Causes cell-cycle arrest at the G2/M phase boundary and cell death by apoptosis ! Member of an elite group of natural products that act as microtubule-stabilizing agent and mitotic spindle poisons ! Taxol, epothilones A and B, sarcodictyin A, eleutherobin, laulimalide, FR182877, peloruside A, dictyostatin ! Effective in Taxol-resistant carcinoma cells ! presence of a small concentration of Taxol amplified discodermolide's toxicity by 20-fold ! potential synergies with the combination of discodermolide with Taxol and other anticancer drugs ! Licensed by Novartis from HBOI in 1998 as a new-generation anticancer drug 1 Cell Apoptosis M - Mitosis G0 Discodermolide disrupts the G2/M phases of the cell cycle. Resting Discodermolide, like Taxol, inhibits microtubule depolymerization by binding G1 - Gap 1 to tubulin. G2 - Gap 2 cells increase in size, cell growth control checkpoint no microtubules = no spindle fiber new proteins formation S - Synthesis DNA replication Me Me Me HO Discodermolide Me O O OH O NH2 Isolation -

United States Patent (19) 11 Patent Number: 5,789,605 Smith, I Et Al
IIIUSOO5789605A United States Patent (19) 11 Patent Number: 5,789,605 Smith, I et al. 45) Date of Patent: Aug. 4, 1998 54 SYNTHETICTECHNIQUES AND Jacquesy et al., "Metabromation Du Dimethyl-2, 6 Phenol INTERMEDIATES FOR POLYHYDROXY, Et De Son Ether Methylique En Milieu Superacide", Tetra DENYL LACTONES AND MIMCS hedron, 1981, 37, 747-751. THEREOF Kim et al., "Conversion of Acetals into Monothioacetals, O-Alkoxyazides and O-Alkoxyalkyl Thioacetates with 75) Inventors: Amos B. Smith, III. Merion; Yuping Magnesium Bromide". Tetra, lett, 1989, 30(48), Qiu; Michael Kaufman, both of 6697-6700. Philadelphia; Hirokaza Arimoto, Longley et al., "Discodermolide-A New, Marine-Derived Drexel Hill, all of Pa.; David R. Jones, Immunosuppressive Compound". Transplantation, 1991. Milford, Ohio; Kaoru Kobayashi, 52(4) 650-656. Osaka, Japan Longley et al., "Discodermolide-A New, Marine-Derived Immunosuppressive Compound". Transplantation, 1991. 73 Assignee: Trustees of the University of 52(4), 657-661. Pennsylvania, Philadelphia, Pa. Longley et al., "Immunosuppression by Discodermolide". Ann. N.Y. Acad. Sci., 1993. 696, 94-107. (21) Appl. No.:759,817 Nerenburg et al., "Total Synthesis of the Immunosuppres 22 Filed: Dec. 3, 1996 sive Agent (-)-Discodermolide". J. Am. Chem, Soc., 1993, 115, 12621-12622. (51) Int. Cl. ................. C07D407/06; C07D 319/06; Paterson, I. et al., "Studies Towards the Total Synthesis of CO7D 309/10 the Marine-derived Immunosuppressant Discodermolide; (52) U.S. Cl. .......................... 549/370; 549/374; 549/417 Asymmetric Synthesis of a C-Cö-Lactone Subunit". J. (58) Field of Search ..................................... 549/370,374, Chen. Soc. Chen, Commun., 1993, 1790-1792. 549/417 Paterson, I. et al., "Studies Towards the Total Synthesis of the Marine-derived Immunosuppresant Discodermolide; 56 References Cited Asymmetric Synthesis of a C-C Subunit". -

Sources, Effects and Risks of Ionizing Radiation
SOURCES, EFFECTS AND RISKS OF IONIZING RADIATION United Nations Scientific Committee on the Effects of Atomic Radiation UNSCEAR 2016 Report to the General Assembly, with Scientific Annexes UNITED NATIONS New York, 2017 NOTE The report of the Committee without its annexes appears as Official Records of the General Assembly, Seventy-first Session, Supplement No. 46 and corrigendum (A/71/46 and Corr.1). The report reproduced here includes the corrections of the corrigendum. The designations employed and the presentation of material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations concerning the legal status of any country, territory, city or area, or of its authorities, or concerning the delimitation of its frontiers or boundaries. The country names used in this document are, in most cases, those that were in use at the time the data were collected or the text prepared. In other cases, however, the names have been updated, where this was possible and appropriate, to reflect political changes. UNITED NATIONS PUBLICATION Sales No. E.17.IX.1 ISBN: 978-92-1-142316-7 eISBN: 978-92-1-060002-6 © United Nations, January 2017. All rights reserved, worldwide. This publication has not been formally edited. Information on uniform resource locators and links to Internet sites contained in the present publication are provided for the convenience of the reader and are correct at the time of issue. The United Nations takes no responsibility for the continued accuracy of that information or for the content of any external website. -

Dissertation.Pdf (1.198Mb)
Syntheses and Bioactivities of Targeted and Conformationally Restrained Paclitaxel and Discodermolide Analogs Chao Yang Dissertation submitted to the faculty of the Virginia Polytechnic Institute and State University In the partial fulfillment of the requirement for the degree of Doctor of Philosophy In Chemistry Dr. David G. I. Kingston, Chairman Dr. Karen Brewer Dr. Paul R. Carlier Dr. Felicia. Etzkorn Dr. Harry W. Gibson August 26 2008 Blacksburg, Virginia Keywords: Taxol, drug targeting, , thio-taxol, tubulin-binding conformation, , T-taxol conformation, macrocyclic taxoids, discodermolide Copyright 2008, Chao Yang Syntheses and Bioactivities of Targeted and Conformationally Restrained Paclitaxel and Discodermolide Analogs Chao Yang Abstract Paclitaxel was isolated from the bark of Taxus brevifolia in the late 1960s. It exerts its biological effect by promoting tubulin polymerization and stabilizing the resulting microtubules. Paclitaxel has become one of the most important current drugs for the treatment of breast and ovarian cancers. Studies aimed at understanding the biologically active conformation of paclitaxel bound on β–tubulin are described. In this work, the synthesis of isotopically labeled taxol analogs is described and the REDOR studies of this compound complexed to tubulin agrees with the hypothesis that palictaxel adopts T-taxol conformation. Based on T-taxol conformation, macrocyclic analogs of taxol have been prepared and their biological activities were evaluated. The results show a direct evidence to support T-taxol conformation. (+) Discodermolide is a polyketide isolated from the Caribbean deep sea sponge Discodermia dissoluta in 1990. Similar to paclitaxel, discodermolide interacts with tubulin and stabilizes the microtubule in vivo. Studies aimed at understanding the biologically active conformation of discodermolide bound on β–tubulin are described. -
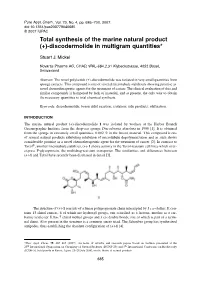
Total Synthesis of the Marine Natural Product (+)-Discodermolide in Multigram Quantities*
Pure Appl. Chem., Vol. 79, No. 4, pp. 685–700, 2007. doi:10.1351/pac200779040685 © 2007 IUPAC Total synthesis of the marine natural product (+)-discodermolide in multigram quantities* Stuart J. Mickel Novartis Pharma AG, CHAD, WKL-684.2.31 Klybeckstrasse, 4052 Basel, Switzerland Abstract: The novel polyketide (+)-discodermolide was isolated in very small quantities from sponge extracts. This compound is one of several microtubule stabilizers showing promise as novel chemotherapeutic agents for the treatment of cancer. The clinical evaluation of this and similar compounds is hampered by lack of material, and at present, the only way to obtain the necessary quantities is total chemical synthesis. Keywords: discodermolide; boron aldol reaction; isolation; side products; olefination. INTRODUCTION The marine natural product (+)-discodermolide 1 was isolated by workers at the Harbor Branch Oceanographic Institute from the deep-sea sponge Discodermia dissoluta in 1990 [1]. It is obtained from the sponge in extremely small quantities, 0.002 % in the frozen material. This compound is one of several natural products exhibiting inhibition of microtubule depolymerization and as such shows considerable promise as a novel chemotherapeutic agent for the treatment of cancer [2]. In contrast to Taxol®, another microtubule stabilizer, (+)-1 shows activity in the Taxol-resistant cell lines which over- express P-glycoprotein, the multidrug-resistant transporter. The similarities and differences between (+)-1 and Taxol have recently been discussed in detail [3]. The structure of (+)-1 consists of a linear polypropionate chain interrupted by 3 cis-olefins. It con- tains 13 chiral centers, 6 of which are hydroxyl groups, one esterified as a lactone, another as a car- bamic acid ester. -

4 Mitotic Catastrophe
4 Mitotic Catastrophe Fiorenza Ianzini, FI, PhD, and Michael A. Mackey, MAM, PhD Summary Mitotic catastrophe (MC) is the result of premature or inappropriate entry of cells into mitosis, usually occurring because of chemical or physical stresses. MC is characterized by changes in nuclear morphology and the eventual appearance of polyploid cell progeny in affected cell populations, is markedly enhanced in cells lacking p53 function, and is the result of overaccumulation of cyclin B1 in cells delayed late in the cell cycle by the inducing agent. Thus, MC is considered to be the predominant mechanism underlying mitotic-linked cell death. Along with characteristic features associated with MC, a delayed DNA damage phenotype has been noted in these populations, suggesting a potential role for MC in mutagenesis and the acquisition of genomic instability. Although generally lethal, some cells can survive MC through mechanisms that are incompletely understood. Cytological features associated with meiotic cell division have been noted in polyploid cell populations produced through MC, a finding that might be particularly relevant in the understanding of tumor progression and that might provide a novel mechanism for the generation of quasi-diploid progeny from MC-induced polyploid cell populations. This review summarizes the literature pertaining to MC and describes current lines of research in this interesting research area. Key Words: Mitotic catastrophe; cell cycle regulation; cyclin B1; endopoly- ploid cells; mitosis; meiosis; carcinogenesis; tumor progression; delayed DNA damage; SPCC. 1. MOLECULAR MECHANISMS UNDERLYING MITOTIC CATASTROPHE 1.1. Mitotic Catastrophe is the Result of Premature Entry into Mitosis Following Abrogation of G2/M Checkpoint Function Exposure of some cell types to a broad class of agents can lead to a loss of regulation of cell division, such that cells enter into a premature mitosis, an event that culminates in a phenomenon called mitotic catastrophe (MC). -
Low Dose and Low Dose-Rate Radiation Effects and Models
Forty-Fourth Annual Meeting Program Low Dose and Low Dose-Rate Radiation Effects and Models April 14–15, 2008 Bethesda North Marriott Hotel & Conference Center 5701 Marinelli Road North Bethesda, MD 20852 On the cover: • top: Two nuclei have each been “hit” by three alpha particles from a microbeam and show activated γH2AX foci at the site of the traversal. • center: Chromosome painting technology makes it possible to identify each human chromosome and characterize the number, location and types of aberrations produced by ionizing radiation. • bottom: Measuring the frequency of micronuclei provides a rapid measure of cytogenetic damage, which increases as a function of radiation dose. Introduction Low Dose and Low Dose-Rate Radiation Effects and Models Forty-Fourth Annual Meeting of the National Council on Radiation Protection and Measurements (NCRP) Potential human health effects of low doses of ionizing models of the biological responses and human health radiation such as those experienced in occupational impacts of exposure to low doses of radiation. The and medical exposures are of great contemporary meeting will feature presentations by international interest. Considerable debate exists over the applica- experts on the topics of (1) molecular, cellular, tissue, bility of a linear-nonthreshold model for characterizing and laboratory animal studies on the effects of expo- the biological responses and health effects of expo- sure to low dose and low dose-rate radiation, (2) sure to low radiation doses, and alternative models results of epidemiological studies on human health have been proposed. A related subject of interest and effects of low radiation doses in occupational, medical debate is the effect of the rate of delivery of radiation and other exposure scenarios, (3) potential impacts of doses on the biological and health outcomes of expo- these findings on future regulatory guidance and pub- sure. -

Radioresistance of Brain Tumors
cancers Review Radioresistance of Brain Tumors Kevin Kelley 1, Jonathan Knisely 1, Marc Symons 2,* and Rosamaria Ruggieri 1,2,* 1 Radiation Medicine Department, Hofstra Northwell School of Medicine, Northwell Health, Manhasset, NY 11030, USA; [email protected] (K.K.); [email protected] (J.K.) 2 The Feinstein Institute for Molecular Medicine, Hofstra Northwell School of Medicine, Northwell Health, Manhasset, NY 11030, USA * Correspondence: [email protected] (M.S.); [email protected] (R.R.); Tel.: +1-516-562-1193 (M.S.); +1-516-562-3410 (R.R.) Academic Editor: Zhe-Sheng (Jason) Chen Received: 17 January 2016; Accepted: 24 March 2016; Published: 30 March 2016 Abstract: Radiation therapy (RT) is frequently used as part of the standard of care treatment of the majority of brain tumors. The efficacy of RT is limited by radioresistance and by normal tissue radiation tolerance. This is highlighted in pediatric brain tumors where the use of radiation is limited by the excessive toxicity to the developing brain. For these reasons, radiosensitization of tumor cells would be beneficial. In this review, we focus on radioresistance mechanisms intrinsic to tumor cells. We also evaluate existing approaches to induce radiosensitization and explore future avenues of investigation. Keywords: radiation therapy; radioresistance; brain tumors 1. Introduction 1.1. Radiotherapy and Radioresistance of Brain Tumors Radiation therapy is a mainstay in the treatment of the majority of primary tumors of the central nervous system (CNS). However, the efficacy of this therapeutic approach is significantly limited by resistance to tumor cell killing after exposure to ionizing radiation. This phenomenon, termed radioresistance, can be mediated by factors intrinsic to the cell or by the microenvironment. -

Positron Emission Tomography
Positron emission tomography A.M.J. Paans Department of Nuclear Medicine & Molecular Imaging, University Medical Center Groningen, The Netherlands Abstract Positron Emission Tomography (PET) is a method for measuring biochemical and physiological processes in vivo in a quantitative way by using radiopharmaceuticals labelled with positron emitting radionuclides such as 11C, 13N, 15O and 18F and by measuring the annihilation radiation using a coincidence technique. This includes also the measurement of the pharmacokinetics of labelled drugs and the measurement of the effects of drugs on metabolism. Also deviations of normal metabolism can be measured and insight into biological processes responsible for diseases can be obtained. At present the combined PET/CT scanner is the most frequently used scanner for whole-body scanning in the field of oncology. 1 Introduction The idea of in vivo measurement of biological and/or biochemical processes was already envisaged in the 1930s when the first artificially produced radionuclides of the biological important elements carbon, nitrogen and oxygen, which decay under emission of externally detectable radiation, were discovered with help of the then recently developed cyclotron. These radionuclides decay by pure positron emission and the annihilation of positron and electron results in two 511 keV γ-quanta under a relative angle of 180o which are measured in coincidence. This idea of Positron Emission Tomography (PET) could only be realized when the inorganic scintillation detectors for the detection of γ-radiation, the electronics for coincidence measurements, and the computer capacity for data acquisition and image reconstruction became available. For this reason the technical development of PET as a functional in vivo imaging discipline started approximately 30 years ago.