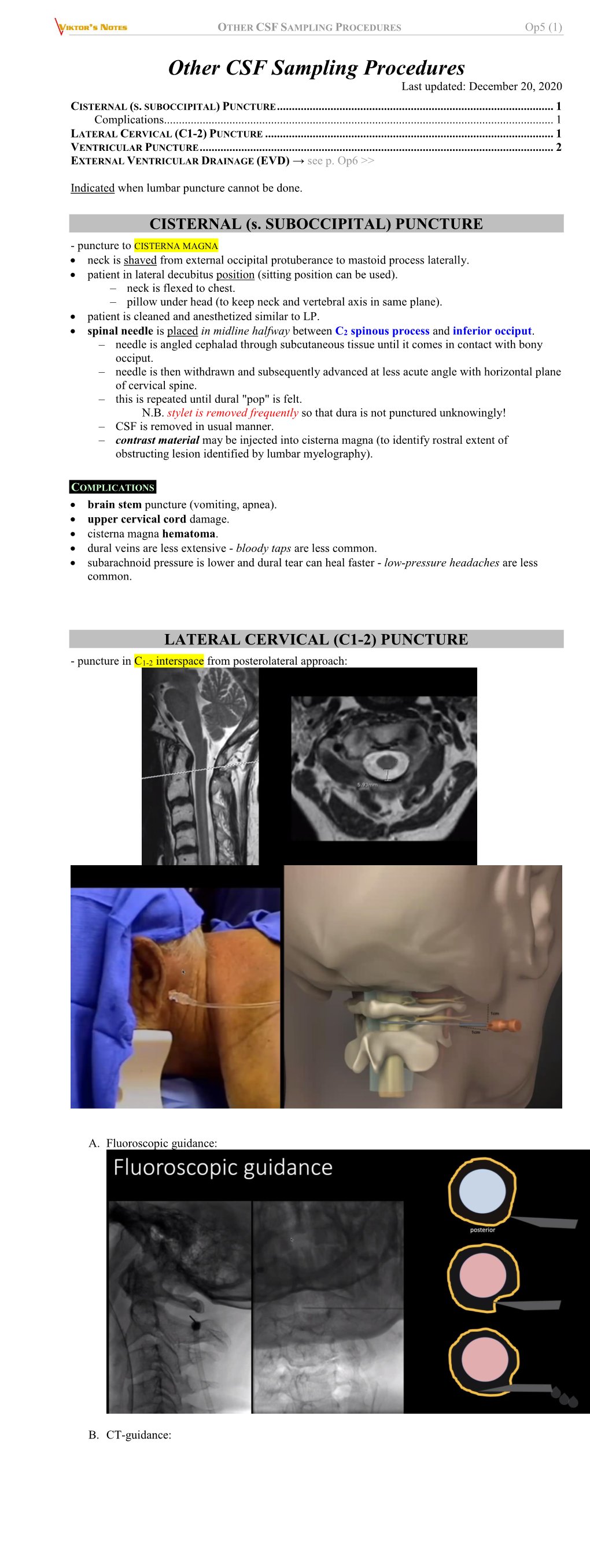
OTHER CSF SAMPLING PROCEDURES Op5 (1)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Evaluation of the Effects of Quercetin on Brain Lesions Secondary to Experimental Hydrocephalus in Rats
Child's Nervous System (2019) 35:2299–2306 https://doi.org/10.1007/s00381-019-04184-2 ORIGINAL ARTICLE Evaluation of the effects of quercetin on brain lesions secondary to experimental hydrocephalus in rats G. B. Sampaio1 & S. C. Da Silva2 & T. H. Romeiro2 & P. D. S. Beggiora2 & H. R. Machado2 & L. D. S. Lopes2 Received: 31 March 2019 /Accepted: 28 April 2019 /Published online: 27 May 2019 # Springer-Verlag GmbH Germany, part of Springer Nature 2019 Abstract Introduction Hydrocephaly is a disease that affects not only the dynamics of the cerebrospinal fluid, but also other structures of the central nervous system. Although shunt is effective in reducing ventriculomegaly, many neurological damages are not reversed with surgery. Several studies demonstrate that oxidative stress is involved in the genesis of hydrocephalus lesions. Objective Evaluate the neuroprotective response of quercetin in hydrocephalus. Materials and methods Male newborns rats were used, which received the 15% kaolin injection in the cisterna magna for induction of hydrocephalus. They were divided into control group (C), untreated hydrocephalic (HN), shunted hydrocephalic (HD), hydrocephalic treated with distilled water (HA), hydrocephalic treated with distilled water and shunt (HDA), hydroce- phalic treated with quercetin peritoneal (HQp), hydrocephalic treated with quercetin peritoneal and shunt (HDQp), hydrocephalic treated with quercetin by gavage (HQg), and hydrocephalus treated with quercetin by gavage and shunt (HDQg). Results Quercetin significantly improved the immunohistochemical markers, mainly caspase and GFAP. There were no signif- icant changes in clinical/behavioral assessment. The use of isolated quercetin does not alter the volume and ventricular size, and the realization of ventriculo-subcutaneous shunt in newborn rats with hydrocephalus presents a high morbi-mortality. -
Flat Panel Detector-CT with Endovenous Injection. Description
Romanian Neurosurgery Journal, Volume XXXII, September 2018, SUPPLEMENT 44th Congress of the Romanian Society of Neurosurgery 5th Danube Carpathian Region Congress 23rd French Course in Neurosurgery Pre-Congress course – September 5, 2018 2nd Nurse Symposium September 5-8, 2018, Timisoara | Romania ABSTRACTS 2 | ABSTRACTS Romanian Neurosurgery Journal, Volume XXXII, September 2018, Supplement | 3 CUPRINS FUNCTIONAL NEUROSURGERY – SURGERY FOR PAIN 2 ............................. 15 CERVICAL DREZ-OTOMY IN PAIN TREATMENT ........................................................... 16 IOANA SOFIA NISTOR, CLAUDIU MATEI, IULIA DANCU SURGERY FOR PAIN IN CANCER PATIENTS .................................................................... 17 ANDREI BRINZEU DORSAL RHIZOTOMY FOR CHILDREN WITH SPASTIC DIPLEGIA – QUADRIPLEGIA OF CEREBRAL PALSY ORIGIN: INTRAOPERATIVE NEUROMONITORING .............................................................................................................. 18 GEORGE GEORGOULIS, ANDREI BRINZEU, MARC SINDOU TRIGEMINAL NEURALGIA AND MICROVASCULAR DECOMPRESSION .... 20 RELIABILITY OF MRI FOR PREDICTING CHARACTERISTICS OF THE NEUROVASCULAR CONFLICTS IN TRIGEMINAL NEURALGIA. IMPLICATION IN SURGICAL DECISION MAKING FOR MICROVASCULAR DECOMPRESSION ......... 21 ANDREI BRINZEU, MARC SINDOU MICROVASCULAR DECOMPRESSION FOR THE TREATMENT OF AN UNUSUAL CASE OF PAINFUL SPASMS IN FACIAL, MASTICATORY, AND MOTOR OCULAR MUSCLES ..................................................................................................................................... -

Uva-DARE (Digital Academic Repository)
UvA-DARE (Digital Academic Repository) Lumbar puncture in bacterial meningitis Costerus, J.M. Publication date 2018 Document Version Other version License Other Link to publication Citation for published version (APA): Costerus, J. M. (2018). Lumbar puncture in bacterial meningitis. General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl) Download date:01 Oct 2021 TECHNOLOGICAL ADVANCES AND CHANGING INDICATIONS FOR LUMBAR PUNCTURE IN NEUROLOGICAL DISORDERS Joost M. Costerus Matthijs C. Brouwer Diederik van de Beek Lancet Neurology. 2018 Mar;17(3): 268-278 15475-J-Costerus_BNW.indd 87 728-08-18 16:37 Chapter 7 Abstract Technological advances have changed the indications for and the way in which lumbar puncture is done. Suspected CNS infection remains the most common indication for lumbar puncture, but new molecular techniques have broadened CSF analysis indications, such as the determination of neuronal autoantibodies in autoimmune encephalitis. -

Congruence of the Topography of Intracranial Calcifications and Epileptic Foci
CONGRUENCE OF THE TOPOGRAPHY OF INTRACRANIAL CALCIFICATIONS AND EPILEPTIC FOCI A. CUKIERT, R PUGLIA, H.B. SCAPOLAN, MM VILELA, R MARINO JR. SUMMARY - Nodular intracranial calcifications (NIC) are frequent findings in CT scans of epileptic patients in countries where granulomatous central nervous disease such as neurocysticercosis is endemic. In 34 consecutive epileptic patients with NIC submitted teo EEG, CT and CSF analysis, the correlation between the electroclinical localization of the focus and the topography of the NIC was studied. Twenty-nine patients had partial (Group I) and 5 had primarily generalized seizures (Group II). Twenty group I and 1 group II patients showed abnormal EEGs. CSF abnormalities consisted of increased protein content (n=3) and positive Weinberg's reaction (n=2). In 2 cases, viable neurocysticercotic vesicles were seen. Twenty-one patients had single NICs. No correlation could be stablished in group II patients. Within group 1,15 patients had a positive and 14 a negative correlation. Sixty-six percent of the patients with single NICs had negative correlations. These findings strongly suggest that the calcifications themselves are not the epileptogenic lesions in at least 50% of the studied cases. KEY WORDS: epilepsy, calcifications, CT, EEG. Congruência da topografia de calcificações intracranianas e focos epilépticos RESUMO - Calcificações nodulares intracranianas (CIN) representam achado frequente em pacientes epilépticos de países onde doenças granulomatosas do SNC (p.e.: neurocisticercose) são endêmicas. Trinta e quatro pacientes epilépticos consecutivos com CINs foram submetidos a exame de EEG, TC e LCR. A correlação entre a topografia do foco e das calcificações foi estudada em cada caso. -

DWI in Transient Global Amnesia and TIA: Proposal for an Ischaemic Origin of TGA K Winbeck, T Etgen, H G Von Einsiedel, M Ro¨Ttinger, D Sander
438 J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.2004.048058 on 16 February 2005. Downloaded from SHORT REPORT DWI in transient global amnesia and TIA: proposal for an ischaemic origin of TGA K Winbeck, T Etgen, H G von Einsiedel, M Ro¨ttinger, D Sander ............................................................................................................................... J Neurol Neurosurg Psychiatry 2005;76:438–441. doi: 10.1136/jnnp.2004.042432 TGA was diagnosed strictly according to well established There are conflicting reports concerning signal intensity criteria.910 TIA was defined as an acute transient focal changes in transient global amnesia (TGA) using diffusion neurological deficit caused by vascular disease that reversed weighted imaging (DWI). We prospectively analysed DWI totally within 24 hours.11 All TIA and TGA patients under- signal intensity changes in TIA and TGA patients, and went an intensive diagnostic investigation including physical compared the clinical characteristics and risk factors of both and neurological examination, duplex sonography of the groups. Using DWI and conventional T1 and T2 weighted carotid arteries, transcranial dopplersonography, 12 lead turbo spin echo sequences, 28 patients with acute TGA (13 ECG, transthoracic echocardiography, and analysis of cardio- men, mean age 61.5 years) and 74 TIA patients (47 men, vascular risk factors such as body mass index, prevalence of mean age 62.4 years) were studied within 48 hours after smoking, hypercholesterolaemia, arterial hypertension, dia- symptom onset. Every patient underwent an intensive betes mellitus, ischaemic heart disease, and carotid athero- diagnostic investigation. In 10/28 (36%) of the TGA patients sclerosis. We also determined the intima2media thickness and 21/74 (28%) of the TIA patients, DWI signal intensity (IMT) of the common carotid artery, as described pre- changes occurred. -
![[6] on the Basal Ganglia.-G. VERCELLINI. Jour. Nerv. Ment. Di)., 1924, Ix, 449](https://docslib.b-cdn.net/cover/8599/6-on-the-basal-ganglia-g-vercellini-jour-nerv-ment-di-1924-ix-449-3318599.webp)
[6] on the Basal Ganglia.-G. VERCELLINI. Jour. Nerv. Ment. Di)., 1924, Ix, 449
J Neurol Psychopathol: first published as 10.1136/jnnp.s1-7.25.60 on 1 July 1926. Downloaded from Go ABSTRACTS [6] On the basal ganglia.-G. VERCELLINI. Jour. Nerv. Ment. Di)., 1924, Ix, 449. THis is a fairly comprehensive study of recent literature on the function of the basal ganglia, from which the author draws the following conclusions: (1) The function of 'tonus' is a purely vegetative function under the control of part of the corpus striatum. Its normal function gives the required plasticity to contraction of muscles and its partial or total lack of control is exhibited in degrees from the impossibility of complete relaxation to tremor and rigidity. (2) The other part of the corpus striatum and lower centres connected with it (in addition to the general tonic function) must control automatic or in any other way stereotyped movements, as this system represents the highest motor centre in those low forms of life where there is no cortical function. It is an instance of loss of independence on the part of a centre which otherwise sticks to its functional characteristics. The human corpus striatum may be compared to a horse which has found its rider. The horseman has the leader- ship, but the motions are the horse's motions and not those of the rider. Protected by copyright. (3) The thalamus is exclusively a sense organ, and through its three connections (with (1) cortex, (2) corpus striatum, (3) subthalamus) are obtained, in line of motor reaction respectively, voluntary motions, tonus, automatic motions, and 'vegetative proper' motor phenomena. -
Basilar Impression and Arnold-Chiarimalformation
J. Neurol. Neurosurg. Psychiat., 1968, 31, 596-605 Basilar impression and Arnold-Chiari malformation A study of 66 cases1 M. CAETANO DE BARROS, W. FARIAS, L. ATAIDE, AND S. LINS From the Institute of Neurology and Neurosurgery, Medical School, Federal University ofPernambuco, Brazil We have been interested for a long time in the Fischgold, David, and Bregeat (1952) described problem of the deformation of the base of the skull two lines, both of them drawn in anteroposterior known as basilar impression and described by the view of the skull. The first joining the tips of the anatomists since 1790 (Ackermann), although only mastoid processes usually passes at the level of the recently recognized from the clinical point of view. atlanto-occipital joints and to 3 mm above or This condition has attracted our attention partic- below the tips of the odontoid process. In patients ularly because of its high incidence in the North- with basilar impression the atlanto-occipital joints east of Brazil and has given rise to other papers and the odontoid process are clearly above this line. written by one of us (de Barros, 1957, 1959). The second line drawn between the two digastric The possibility of precise pre-operative diagnosis grooves passes well above the tip of the odontoid has been established by Chamberlain's paper (1939). process in normal skulls (Fig. 2). As routine for the This author described a line in plain radiograph of radiological diagnosis of basilar impression we use the skull which permits recognition of the mal- the Chamberlain's and Fischgold's lines taken in formation under discussion. -

R J M E HORT ISTORICAL EVIEW Romanian Journal of S H R Morphology & Embryology
Rom J Morphol Embryol 2019, 60(1):333–336 R J M E HORT ISTORICAL EVIEW Romanian Journal of S H R Morphology & Embryology http://www.rjme.ro/ Remember the Romanian pioneers: Alexandru Obregia (1860–1937) – first in vivo suboccipital puncture MIRCEA VICENŢIU SĂCELEANU1), ANDREI ALEXANDRU MARINESCU2), AUREL GEORGE MOHAN3), MIHAI POPESCU4), ALEXANDRU VLAD CIUREA2,5) 1)Department of Neurosurgery, “Victor Papilian” Faculty of Medicine, “Lucian Blaga” University, Sibiu, Romania; Department of Neurosurgery, Emergency County Hospital, Sibiu, Romania 2)“Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania 3)Department of Neurosurgery, Faculty of Medicine and Pharmacy, University of Oradea, Romania; Department of Neurosurgery, Bihor Emergency County Hospital, Oradea, Romania 4)Department of Medical Assistance and Kinetotherapy, Faculty of Sciences, Physical Education and Informatics, University of Piteşti, Romania; Department of Neurosurgery, Emergency Hospital of Argeş County, Piteşti, Romania 5)Department of Neurosurgery, “Sanador Medical Center” Hospital, Bucharest, Romania Abstract In a time when doctors had limited knowledge about neuroanatomy and were focused primarily on clinical data, paraclinical investigations were overlooked even though they offered much needed information about the patients. Prof. Dr. Alexandru Obregia (1860–1937) is one of the forgotten pioneers of cerebrospinal fluid (CSF) investigation techniques. He envisioned, performed, and wrote about the very first in vivo suboccipital puncture, in 1908. The invention of this investigation technique was a considerable step forward in understanding the CSF and was Prof. Alexandru Obregia’s most important scientific work. This, in turn, inspired Thoma Ionescu (1860–1926) to create the general rachianesthesia technique, in 1919, which allowed surgeons to perform a new range of procedures safely. -

Cisternal Puncture Complications-Treatment of Coccidioidal Meningitis with Amphotericin B
Refer to: Keane JR: Cisternal puncture complications-Treatment of coccidioidal meningitis with amphotericin B. Calif Med 119:10-15, Sep 1973 Cisternal Puncture Complications Treatment of Coccidioidal Meningitis with Amphotericin B JAMES R. KEANE, MD, Los Angeles Of two patients who had acute neurologic damage from cis- ternal punctures, one died 17 hours following a tap which produced major subarachnoid hemorrhage, the other patient recovered from probable brain stem infarction associated with cisterna magna amphotericin injection. Subarachnoid hemorrhage is the commonest major com- plication of cisternal puncture, with at least 30 reported fatal- ities. Other serious complications result from direct puncture of brain substance. Cisternal puncture is not an appropriate alternative to a difficult lumbar puncture, and indications for its use are limited. The occasional required cisternal tap should be performed only by persons carefully trained in the technique, preferably utilizing fluoroscopic guidance, and only where neurosurgical assistance is readily available. Post-puncture subarachnoid hemorrhage accompanied by progressive obtundation requires emergency evaluation and consideration of posterior fossa decompression. INTRATHECAL AMPHOTERICIN B TREATMENT of and the need for exacting technique to avoid pos- coccidioidal meningitis has greatly increased the sibly disastrous complications, but recent descrip- number of cisternal punctures performed in Cali- tions are more inclined to stress patient acceptance, fornia and Arizona. technical ease, and a low incidence of post-punc- Ayer and other clinicians performing early per- ture headache. cutaneous punctures of the cisterna magna stressed The following two case reports illustrate the the importance of preliminary practice on cadavers hazards of cisternal puncture. From the Department of Neurology, Los Angeles County/Uni- CASE 1. -

Cerebrospinal Fluid by A. Tipold; B0235.0803
In: Clinical Neurology in Small Animals - Localization, Diagnosis and Treatment, K.G. Braund (Ed.) Publisher: International Veterinary Information Service (www.ivis.org), Ithaca, New York, USA. Cerebrospinal Fluid (22-Aug-2003) A. Tipold Small Animal Clinic, Tierärztliche Hochschule Hannover, Hannover, Germany. Introduction The presence of cerebrospinal fluid (CSF) within the cavities of the brain was already known to the ancients. Probably, the first report of the existence of CSF was performed in the 17th century B.C., and Hippocrates described the occurrence of fluid in brain cavities in the 4th century B.C.; however, it was thought to be pathological. Galen described the ventricular cavities in the 2nd century A.D. For a long time these cavities were thought to be filled with "vital spirit". Only in the 16th century A.D. did Vesalius again discover a watery humor. Systematic studies of this fluid started later and in 1825 Magendie performed the first tap of the cisterna magna in animals. The examination of CSF was introduced by Quincke 1891, and in 1901 cytological techniques were established by Widal and others [1]. CSF and the Ventricular System Normal and Pathological Findings Anatomy Color - Ventricles Cell Counts - Choroid Plexus Glucose - Brain Capillaries Protein - Ependyma - IgG-Index - Leptomeninges Antigen Detection - Extracellular Interstitial Fluid Enzymes - Dura Mater Other Metabolites Physiology Intracranial Pressure - Secretion - Absorption - Function - Composition - Acquisition Cerebrospinal Fluid and the Ventricular System Anatomy Cerebrospinal fluid is mostly located in the ventricular system and the subarachnoid space. The ventricular system develops from the neural tube and includes the lateral ventricles, third ventricle, the mesencephalic aqueduct and the fourth ventricle, which continues into the central canal of the spinal cord. -

Laceration of the Posterior Inferior Cerebellar Artery by Suboccipital Puncture of the Cisterna Magna
Arq Neuropsiquiatr 2004;62(3-B):882-884 LACERATION OF THE POSTERIOR INFERIOR CEREBELLAR ARTERY BY SUBOCCIPITAL PUNCTURE OF THE CISTERNA MAGNA Case report Luiz Antonio Pezzi Portela1, Valéria Souza1, Félix Hendrick Pahl2, Alberto Cappel Cardoso2, Eduardo de Arnaldo Silva Vellutini2, Eduardo Genaro Mutarelli2, Luis dos Ramos Machado3, José Antonio Livramento3 ABSTRACT - We report the case of a 27 year old man who presented to the emergency room of a hospital with headache, vomiting and an episode of loss of conciousness. A cranial CT scan was normal and the pa- tient discharged. Ten hours later he came to the emergency room of our hospital with the same complaints. A technically difficult cisternal puncture in an anxious patient who moved during the needle introduction was done. The CSF sample showed 1600 intact red blood cells without other alterations. His headache worse- ned and after 6 hours he became drowsy, numb and exhibited decerebration signs. A new CT scan showed diffuse subarachnoid and intraventricular blood. An emergency angiogram demonstrated laceration of a left posterior-inferior cerebellar artery in its retrobulbar loop with a pseudoaneurysm. He was succesfully treated by surgical clipping without injury. Sixteen days later he was discharged with a normal neurologi- cal exam. KEY WORDS: CSF, suboccipital puncture, angiogram, posterior inferior cerebellar artery, pseudoaneurysm, laceration. Laceração da artéria cerebelar póstero-inferior causada por punção suboccipital: relato de caso RESUMO - Relatamos o caso de um homem de 27 anos que procurou o pronto atendimento de um hospi- tal com cefaléia intensa, vômitos e um episódio de perda de consciência. Uma tomografia de crânio foi nor- mal e o paciente foi dispensado. -

Sinal De Lhermitte Durante Punção Cervical Lateral
SINAL DE LHERMITTE DURANTE PUNÇÃO CERVICAL LATERAL SUMARIO DOS ACIDENTES POSSÍVEIS NA PUNÇÃO LATERAL, C1-C2 E RELATO DE DOIS CASOS DE PENETRAÇÃO MEDULAR SANDRO L. R0SSITTI * — ROQUE J. BALBO ** RESUMO — O sinal de Lhermitte foi referido por dois pacientes durante punção lateral C1-C2 (PCL), devido a penetração acidental da medula espinhal. Apresentamos breve revisão da literatura sobre a lesão nervosa e/ou vascular acidental durante a PCL e fazemos reco mendações técnicas para a sua prevenção. Lhermitte's sign during lateral cervical puncture: a survey on possible accidents on lateral C1-C2 puncture with report of two cases of spinal cord puncture. SUMMARY — Lhermitte's sign was referred by two patients during lateral cervical puncture (LCP) due to accidental puncture of the spinal cord; no sequelae were observed in these patients. A brief review of the literature is presented, concerning: 1. Lhermitte's sign; 2. reported accidents during LCP. Avoidance of neural and/or vascular injuries is possible by employing the posterior approach to LCP (puncture of the dorsal spinal subarachnoid space at C1-C2). The lateral suboccipital puncture (at the atlanto-occipital space) of the cisterna magna is also recommended. A punção cervical (no espaço C1-C2) e sub-occipital (no espaço atlanto-occipi tal) pela via lateral (PCL e PSOL, respectivamente) prestam-se a coleta de liqüido cefalorraqueano (LCR) e a procedimentos neurorradiológicos. A técnica é simples, empregando-se controle radioscópico opcional. 0 paciente é posicionado, prono ou supino, com seu pescoço absoluta e necessariamente retificado. Segue-se antissepsia e infiltração anestésica sobre os pontos de referência para a inserção da agulha: 10 mm dorsal e 10 mm abaixo do ápice da mastóide para a PCL; de 10 a 25 mm dorsal ao ápice da mastóide para a PSOL, sendo observado o plano horizontal ana tômico 11.22.