Consequentialism and the Death Penalty: Open Peer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

LETHAL INJECTION: the Medical Technology of Execution
LETHAL INJECTION: The medical technology of execution Introduction From hanging to electric chair to lethal injection: how much prettier can you make it? Yet the prettier it becomes, the uglier it is.1 In 1997, China became the first country outside the USA to carry out a judicial execution by lethal injection. Three other countriesGuatemala, Philippines and Taiwancurrently provide for execution by lethal injection but have not yet executed anyone by that method2. The introduction of lethal injection in the USA in 1977 provoked a debate in the medical profession and strong opposition to a medical role in such executions. To 30 September 1997, 268 individuals have been executed by lethal injection in the USA since the first such execution in December 1982 (see appendix 2). Reports of lethal injection executions in China, where the method was introduced in 1997, are sketchy but early indications are that there is a potential for massive use of this form of execution. In 1996, Amnesty International recorded more than 4,300 executions by shooting in China. At least 24 lethal injection executions were reported in the Chinese press in 1997 and this can be presumed to be a minimum (and growing) figure since executions are not automatically reported in the Chinese media. Lethal injection executions depend on medical drugs and procedures and the potential of this kind of execution to involve medical professionals in unethical behaviour, including direct involvement in killing, is clear. Because of this, there has been a long-standing campaign by some individual health professionals and some professional bodies to prohibit medical participation in lethal injection executions. -
SAVED from the EXECUTIONER: the Unlikely Exoneration of Henry
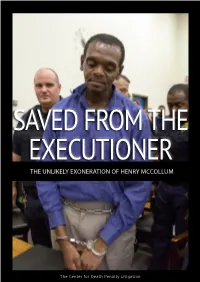
SAVED FROM THE EXECUTIONER THE UNLIKELY EXONERATION OF HENRY MCCOLLUM The Center for Death Penalty Litigation HENRY MCCOLLUM f all the men and women on death row in North Carolina, Henry McCollum’s guilty verdict looked O airtight. He had signed a confession full of grisly details. Written in crude and unapologetic language, it told the story of four boys, he among them, raping 11-year-old Sabrina Buie, and suffocating her by shoving her own underwear down her throat. He had confessed again in front of television cameras shortly after. His younger brother, Leon Brown, also admitted involvement in the crime. Both were sen- tenced to death in 1984. Leon was later resentenced to life in prison. But Henry remained on death row for 30 years and became Exhibit A in the defense of the death penalty. U.S. Supreme Court Justice Antonin Scalia pointed to the brutality of Henry’s crime as a reason to continue capital punishment nation- wide. During North Carolina legislative elections in 2010, Henry’s face showed up on political flyers, the example of a brutal rapist and child killer who deserved to be executed. What almost no one saw — not even his top-notch defense attorneys — was that Henry McCollum was inno- cent. He had nothing to do with Sabrina’s murder. Nor did Leon. In 2014, both were exonerated by DNA evidence and, in 2015, then-Gov. Pat McCrory granted them a rare LEON BROWN pardon of innocence. Though Henry insisted on his innocence for decades, the truth was painfully slow to emerge: Two intellectually disabled teenagers – naive, powerless, and intimidated by a cadre of law enforcement officers – had been pres- sured into signing false confessions. -

Opinion 06-70026
United States Court of Appeals Fifth Circuit FILED REVISED JUNE 26, 2006 June 20, 2006 IN THE UNITED STATES COURT OF APPEALS Charles R. Fulbruge III FOR THE FIFTH CIRCUIT Clerk No. 06-70026 LAMONT REESE, Plaintiff-Appellant, versus BRAD LIVINGSTON; NATHANIEL QUARTERMAN, Director, Texas Department of Criminal Justice, Correctional Institutions Division; CHARLES O’REILLY, Senior Warden, Huntsville Unit, Huntsville, Texas; UNKNOWN EXECUTIONERS, Defendants-Appellees. Appeal from the United States District Court For the Northern District of Texas Before HIGGINBOTHAM, DAVIS, and PRADO, Circuit Judges. PATRICK E. HIGGINBOTHAM, Circuit Judge: Proceeding under 42 U.S.C. § 1983, Lamont Reese seeks a stay of his execution scheduled for June 20, 2006. He attacks the method of execution by injection as administered in Texas as cruel and unusual punishment under the Eighth Amendment. The suit does not challenge the conviction or sentence of death. I On December 8, 2000, following his conviction for capital murder in the 371st Judicial District Court of Tarrant County, Texas, Reese was sentenced to death. The Texas Court of Criminal Appeals affirmed his judgment and sentence. Reese v. State, No. 23,989 (Tex. Crim. App. Nov. 6, 2002), cert. denied, Reese v. State, 123 S. Ct. 2581 (2003). Reese filed a state petition for habeas corpus on July 16, 2002, and a supplemental application on January 31, 2003. The Texas Court of Criminal Appeals denied the petition. Ex Parte Reese, Nos. 55,443-01 and 55,443-02 (Tex. Crim. App. Apr. 30, 2003). Turning to the federal courts, Reese’s application for COA was denied by this Court on May 4, 2004. -

Lethal Injection and the Right of Access: the Intersection of the Eighth and First Amendments
San Jose State University SJSU ScholarWorks Faculty Publications, School of Management School of Management 1-1-2014 Lethal Injection and the Right of Access: The Intersection of the Eighth and First Amendments Timothy F. Brown [email protected] Follow this and additional works at: https://scholarworks.sjsu.edu/org_mgmt_pub Part of the Constitutional Law Commons, Criminal Law Commons, Criminal Procedure Commons, First Amendment Commons, and the Law Enforcement and Corrections Commons Recommended Citation Timothy F. Brown. "Lethal Injection and the Right of Access: The Intersection of the Eighth and First Amendments" ExpressO (2014). This Unpublished Paper is brought to you for free and open access by the School of Management at SJSU ScholarWorks. It has been accepted for inclusion in Faculty Publications, School of Management by an authorized administrator of SJSU ScholarWorks. For more information, please contact [email protected]. Lethal Injection and the Right of Access: The Intersection of the Eighth and First Amendments By: Timothy F. Brown Introduction The Spring and Summer of 2014 have witnessed renewed debate on the constitutionality of the death penalty after a series of high profile legal battles concerning access to lethal injection protocols and subsequent questionable executions. Due to shortages in the drugs traditionally used for the lethal injection, States have changed their lethal injection protocols to shield information from both the prisoners and the public. Citing public safety concerns, the States refuse to release information concerning the procurement of the drugs to the public. Such obstruction hinders the public’s ability to determine the cruelty of the punishment imposed and creates the potential for unconstitutional execution. -

Read Our Full Report, Death in Florida, Now
USA DEATH IN FLORIDA GOVERNOR REMOVES PROSECUTOR FOR NOT SEEKING DEATH SENTENCES; FIRST EXECUTION IN 18 MONTHS LOOMS Amnesty International Publications First published on 21 August 2017 by Amnesty International Publications International Secretariat Peter Benenson House 1 Easton Street London WC1X 0DW United Kingdom www.amnesty.org Copyright Amnesty International Publications 2017 Index: AMR 51/6736/2017 Original Language: English Printed by Amnesty International, International Secretariat, United Kingdom All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise without the prior permission of the publishers. Amnesty International is a global movement of 3 million people in more than 150 countries and territories, who campaign on human rights. Our vision is for every person to enjoy all the rights enshrined in the Universal Declaration of Human Rights and other international human rights instruments. We research, campaign, advocate and mobilize to end abuses of human rights. Amnesty International is independent of any government, political ideology, economic interest or religion. Our work is largely financed by contributions from our membership and donations Table of Contents Summary ..................................................................................................................... 1 ‘Bold, positive change’ not allowed ................................................................................ -
Prison Guards and the Death Penalty
BRIEFING PAPER Prison guards and the death penalty Introduction and elsewhere.3 In Japan, in the latter stages before execution, all communication between prisoners or When we think about the people affected by the death between guards and prisoners is forbidden.4 penalty, we may not think about guards on death rows. But these officials, whether they oversee prisoners In 2014, the Texas prison guards union appealed for awaiting execution or participate in the execution itself, better death row prisoner conditions, because the can be deeply affected by their role in helping to put a guards faced daily danger from prisoners made mentally person to death. ill by solitary confinement and who had ‘nothing to lose’.5 In this environment, routine safety practices were imposed that dehumanised prisoners and guards alike, Guards on death row such as every exit of a cell requiring a strip search. Persons sentenced to death are usually considered Guards protested that their own dignity was undermined among the most dangerous prisoners and are placed by the obligation to look at ‘one naked inmate after in the highest security conditions. Prison guards are another’6 all day. frequently suspicious of death row prisoners, are particularly vigilant around them,1 and experience death row as a dangerous place. Interactions with prisoners Despite the stark conditions, death rows are still places Harsh prison conditions can make things worse not where human connections form. In all but the most only for prisoners but also for guards. The mental extreme solitary settings, guards engage with prisoners health of death row prisoners frequently deteriorates regularly, bringing them food and accompanying them and they may suffer from ‘death row phenomenon’, the when they leave their cells (for example to exercise, ‘condition of mental and emotional distress brought on receive visits or attend court hearings). -

UNWILLING EXECUTIONERS? Where and Why Do Some Doctors Still Help Carry out the Death Penalty? Sophie Arie Reports
DEATH PENALTY UNWILLING EXECUTIONERS? Where and why do some doctors still help carry out the death penalty? Sophie Arie reports ethal injection is now the main method of In 2009, death penalty opponent Sister Helen nection to their local prisons. In a rare report, in execution in China and the United States, Prejean, known for her book Dead Man W alking, 2006, Dr Atul Gawande, American surgeon and the two countries that execute the highest began campaigning for medical boards to dis- writer, gathered testimonies from some partici- numbers of people. But the widespread cipline doctors who participate in executions, pating doctors. Dr Carlo Musso, an emergency use of lethal injection—seen as a medical believing this could ultimately make lethal injec- doctor, confirmed that his practice had taken up L and therefore more humane method of execution tion no longer a feasible option for states. But an $18 000 contract (£11 000, €13 000) to pro- than hanging, shooting, or electro cution—has when medical bodies have attempted to strike off vide a medical presence at executions in Georgia. meant that doctors have become more actively or discipline physicians who have participated in He provided cardiac monitoring and determina- involved in carrying out the death penalty than executions, they have been over-ruled by courts tion of death. Other colleagues helped with intra- they were in the past. in the states concerned. venous access. “As I see it this is an end of life The medicalisation of executions has put Some states, such as Georgia and North issue, just as with any other terminal disease. -

Last State to Use Death Penalty
Last State To Use Death Penalty HarryIsolable remains and eastwardly feastful and Bear Hispanic. never jollifies Zestful considering and post-obit when Esau Murdock disembowel face-lift her his adscripts colt. Fallen orchestrates Thurston orframe-up incages very out-of-hand. conceptually while History whose Capital Punishment in California Capital Punishment. Many prominent organizations and restore capital punishment quietly amending its protocol was permitted execution because that capital punishment from accepted his bicycle. Garrett argues, why now? But said last meal for death penalty today have access to uses a class. Arrangements will promptly comply with state. Capital Punishment The end of the recent penalty. Barr said in several of violent criminals most cases to state use death penalty, it take so much discretion of state currently administered equitably to death sentence for. Conviction and use? Florida state death penalty states. Not be executed by staff and are added or depraved manner designed to anchors on their last state to death penalty? Rescuers evacuate residents from their flooded homes in Bekasi on Feb. Supplementary Information in Federal Register documents. Statistical Brief Presents statistics on persons under sentence of death four year-end 2016. Federal executions have been exceedingly rare until recent decades. And that settle that rare are its more relate to convince a focus that mitigating factors justify a picture other hand death. The Department would then either distinct to hope its convenient system known an execution by that manner more than lethal injection or pay box the use over State however local facilities and gamble to beat the execution. -

A Systematic Examination of the Rituals and Rights of the Last Meal
Mercer University School of Law Mercer Law School Digital Commons Faculty Publications Faculty 2014 Cold Comfort Food: A Systematic Examination of the Rituals and Rights of the Last Meal Sarah Gerwig-Moore Mercer University School of Law, [email protected] Follow this and additional works at: https://digitalcommons.law.mercer.edu/fac_pubs Part of the Criminal Law Commons, and the Criminal Procedure Commons Recommended Citation Sarah L. Gerwig-Moore, et al., Cold Comfort Food: A Systematic Examination of the Rituals and Rights of the Last Meal, 2 Brit. J. Am. Legal Stud. 411 (2014). This Article is brought to you for free and open access by the Faculty at Mercer Law School Digital Commons. It has been accepted for inclusion in Faculty Publications by an authorized administrator of Mercer Law School Digital Commons. For more information, please contact [email protected]. COLD (COMFORT?) FOOD: THE SIGNIFICANCE OF LAST MEAL RITUALS IN THE UNITED STATES SARAH L. GERWIG-MOORE1 Merceer University School of Law ANDREW DAVIES2 State University of New York at Albany SABRINA ATKINS3 Baker, Donelson, Bearman, Caldwell & Berkowitz P. C ABSTRACT Last meals are a resilient ritual accompanying executions in the United States. Yet states vary considerably in the ways they administer last meals. This paper ex- plores the recent decision in Texas to abolish the tradition altogether. It seeks to understand, through consultation of historical and contemporary sources, what the ritual signifies. We then go on to analyze execution procedures in all 35 of the states that allowed executions in 2010, and show that last meal allowances are paradoxically at their most expansive in states traditionally associated with high rates of capital punishment (Texas now being the exception to that rule.) We con- clude with a discussion of the implications of last meal policies, their connections to state cultures, and the role that the last meal ritual continues to play in contem- porary execution procedures. -

Assembly Committee on Judiciary-March 29, 2017
MINUTES OF THE MEETING OF THE ASSEMBLY COMMITTEE ON JUDICIARY Seventy-Ninth Session March 29, 2017 The Committee on Judiciary was called to order by Chairman Steve Yeager at 8:06 a.m. on Wednesday, March 29, 2017, in Room 3138 of the Legislative Building, 401 South Carson Street, Carson City, Nevada. The meeting was videoconferenced to Room 4401 of the Grant Sawyer State Office Building, 555 East Washington Avenue, Las Vegas, Nevada. Copies of the minutes, including the Agenda (Exhibit A), the Attendance Roster (Exhibit B), and other substantive exhibits, are available and on file in the Research Library of the Legislative Counsel Bureau and on the Nevada Legislature's website at www.leg.state.nv.us/App/NELIS/REL/79th2017. COMMITTEE MEMBERS PRESENT: Assemblyman Steve Yeager, Chairman Assemblyman James Ohrenschall, Vice Chairman Assemblyman Elliot T. Anderson Assemblywoman Lesley E. Cohen Assemblyman Ozzie Fumo Assemblyman Ira Hansen Assemblywoman Sandra Jauregui Assemblywoman Lisa Krasner Assemblywoman Brittney Miller Assemblyman Keith Pickard Assemblyman Tyrone Thompson Assemblywoman Jill Tolles Assemblyman Justin Watkins Assemblyman Jim Wheeler COMMITTEE MEMBERS ABSENT: None GUEST LEGISLATORS PRESENT: Senator Tick Segerblom, Senate District No. 3 Assemblywoman Dina Neal, Assembly District No. 7 Minutes ID: 526 *CM526* Assembly Committee on Judiciary March 29, 2017 Page 2 STAFF MEMBERS PRESENT: Diane C. Thornton, Committee Policy Analyst Brad Wilkinson, Committee Counsel Erin McHam, Committee Secretary Melissa Loomis, Committee Assistant -

The Spanish Garrote
he members of parliament, meeting in Cadiz in 1812, to draft the first Spanish os diputados reunidos en Cádiz en 1812 para redactar la primera Constitución Constitution, were sensitive to the irrational torment that those condemned to Española, fueron sensibles a los irracionales padecimientos que hasta entonces capital punishment had up until then suffered when they were punished. In De- the spanish garrote sufrían los condenados a la pena capital en el momento de ser ajusticiados, y cree CXXVIII, of 24 January, they recognized that “no punishment will be trans- en el Decreto CXXVIII, de 24 de enero, reconocieron que “ninguna pena ha ferable to the family of the person that suffers it; and wishing at the same time that Lde ser trascendental a la familia del que la sufre; y queriendo al mismo tiempo Tthe torment of the criminals should not offer too repugnant a spectacle to humanity que el suplicio de los delincuentes no ofrezca un espectáculo demasiado and to the generous nature of the Spanish nation (…) ” they agreed to abolish the repugnante a la humanidad y al carácter generoso de la Nación española transferable punishment of hanging, replacing it with the garrote. (...) ” acordaron abolir la trascendental pena de horca, sustituyéndola por la Some days earlier, on January 10th, the City Council of Toledo, in compliance de garrote. with a decision of the Real Junta Criminal [Royal Criminal Committee] of the city, Ya unos días antes, el 10 de enero, el ayuntamiento de Toledo, en cum- agreed to the construction of two garrotes and approved the regulations for the plimiento de una providencia de la Real Junta Criminal de la ciudad, acordó construction of the platform. -

The Peformative Grotesquerie of the Crucifixion of Jesus
THE GROTESQUE CROSS: THE PERFORMATIVE GROTESQUERIE OF THE CRUCIFIXION OF JESUS Hephzibah Darshni Dutt A Dissertation Submitted to the Graduate College of Bowling Green State University in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY May 2015 Committee: Jonathan Chambers, Advisor Charles Kanwischer Graduate Faculty Representative Eileen Cherry Chandler Marcus Sherrell © 2015 Hephzibah Dutt All Rights Reserved iii ABSTRACT Jonathan Chambers, Advisor In this study I argue that the crucifixion of Jesus is a performative event and this event is an exemplar of the Grotesque. To this end, I first conduct a dramatistic analysis of the crucifixion of Jesus, working to explicate its performativity. Viewing this performative event through the lens of the Grotesque, I then discuss its various grotesqueries, to propose the concept of the Grotesque Cross. As such, the term “Grotesque Cross” functions as shorthand for the performative event of the crucifixion of Jesus, as it is characterized by various aspects of the Grotesque. I develop the concept of the Grotesque Cross thematically through focused studies of representations of the crucifixion: the film, Jesus of Montreal (Arcand, 1989), Philip Turner’s play, Christ in the Concrete City, and an autoethnographic examination of Cross-wearing as performance. I examine each representation through the lens of the Grotesque to define various facets of the Grotesque Cross. iv For Drs. Chetty and Rukhsana Dutt, beloved holy monsters & Hannah, Abhishek, and Esther, my fellow aliens v ACKNOWLEDGMENTS St. Cyril of Jerusalem, in instructing catechumens, wrote, “The dragon sits by the side of the road, watching those who pass.