2000 TRAI{SACTIOI\}5 Americal\ OTOLOGICAL SOCIETY, II{C
Total Page:16
File Type:pdf, Size:1020Kb
Recommended publications
-
2015 Topps UFC Chronicles Checklist
BASE FIGHTER CARDS 1 Royce Gracie 2 Gracie vs Jimmerson 3 Dan Severn 4 Royce Gracie 5 Don Frye 6 Vitor Belfort 7 Dan Henderson 8 Matt Hughes 9 Andrei Arlovski 10 Jens Pulver 11 BJ Penn 12 Robbie Lawler 13 Rich Franklin 14 Nick Diaz 15 Georges St-Pierre 16 Patrick Côté 17 The Ultimate Fighter 1 18 Forrest Griffin 19 Forrest Griffin 20 Stephan Bonnar 21 Rich Franklin 22 Diego Sanchez 23 Hughes vs Trigg II 24 Nate Marquardt 25 Thiago Alves 26 Chael Sonnen 27 Keith Jardine 28 Rashad Evans 29 Rashad Evans 30 Joe Stevenson 31 Ludwig vs Goulet 32 Michael Bisping 33 Michael Bisping 34 Arianny Celeste 35 Anderson Silva 36 Martin Kampmann 37 Joe Lauzon 38 Clay Guida 39 Thales Leites 40 Mirko Cro Cop 41 Rampage Jackson 42 Frankie Edgar 43 Lyoto Machida 44 Roan Carneiro 45 St-Pierre vs Serra 46 Fabricio Werdum 47 Dennis Siver 48 Anthony Johnson 49 Cole Miller 50 Nate Diaz 51 Gray Maynard 52 Nate Diaz 53 Gray Maynard 54 Minotauro Nogueira 55 Rampage vs Henderson 56 Maurício Shogun Rua 57 Demian Maia 58 Bisping vs Evans 59 Ben Saunders 60 Soa Palelei 61 Tim Boetsch 62 Silva vs Henderson 63 Cain Velasquez 64 Shane Carwin 65 Matt Brown 66 CB Dollaway 67 Amir Sadollah 68 CB Dollaway 69 Dan Miller 70 Fitch vs Larson 71 Jim Miller 72 Baron vs Miller 73 Junior Dos Santos 74 Rafael dos Anjos 75 Ryan Bader 76 Tom Lawlor 77 Efrain Escudero 78 Ryan Bader 79 Mark Muñoz 80 Carlos Condit 81 Brian Stann 82 TJ Grant 83 Ross Pearson 84 Ross Pearson 85 Johny Hendricks 86 Todd Duffee 87 Jake Ellenberger 88 John Howard 89 Nik Lentz 90 Ben Rothwell 91 Alexander Gustafsson -

Bantamweight Superstar 'The California Kid' Urijah Faber
BANTAMWEIGHT SUPERSTAR ‘THE CALIFORNIA KID’ URIJAH FABER MEETS SCOTT ‘YOUNG GUNS’ JORGENSEN ON APRIL 13 AT MANDALAY BAY IN LAS VEGAS Las Vegas, Nevada – Fresh off a brilliant submission victory over Ivan Menjivar at UFC 157, “The California Kid” Urijah Faber returns to the Octagon® Saturday, April 13 at the Mandalay Bay Events Center in Las Vegas to meet Scott Jorgensen in a can’t-miss bantamweight showdown. Faber, the former WEC featherweight champion ranked second in the bantamweight division, is known for his explosive athleticism and finishing ability, and the 33-year-old Sacramento native owns wins over the likes of Jens Pulver (twice), Raphael Assuncao, Takeya Mizugaki, Eddie Wineland and Brian Bowles. A three-time Pac-10 wrestling champion at Boise State University, the 30-year-old Jorgensen defeated John Albert in a performance that earned him Fight and Submission of the Night honors in his most recent bout this past December. “Young Guns” also holds notable victories over Jeff Curran and Brad Pickett and has developed a reputation as one of the division’s most exciting fighters. “Urijah Faber is one of the best bantamweights in the world and he proved it at UFC 157 by submitting Ivan Menjivar in the first round,” UFC President Dana White said. “He’s ready to jump right back in the Octagon on April 13 with Scott Jorgensen, who’s ranked seventh in the world at 135 pounds. Both of these guys like to finish fights. This is a really exciting main event for the TUF Finale!” In addition to the Faber-Jorgensen main event, this season’s The Ultimate Fighter® winner will be crowned when the Octagon® makes its way back to the Mandalay Bay Events Center. -

2017: Fight Card and Results: Events 386 to 424
2017: Fight Card and Results: Events 386 to 424 Event 424 UFC 219: Cyborg vs. Holm December 30, 2017 Las Vegas, Nevada Weight Winner Loser Method Round Time Women's Featherweight Championship Women's Feather Cris Cyborg © Holly Holm Decision (unanimous) (49‐46, 48‐47, 48‐47) 5 5:00 Lightweight Khabib Nurmagomedov Edson Barboza Decision (unanimous) (30‐25, 30‐25, 30‐24) 3 5:00 Lightweight Dan Hooker Marc Diakiese Submission (guillotine choke) 3 0:42 Women's Straw Carla Esparza Cynthia Calvillo Decision (unanimous) (29‐28, 29‐28, 29‐28) 3 5:00 Welterweight Neil Magny Carlos Condit Decision (unanimous) (30‐27, 30‐27, 29‐28) 3 5:00 Light Heavyweight Michał Oleksiejczuk Khalil Rountree Jr. Decision (unanimous) (30‐27, 30‐27, 30‐27) 3 5:00 Featherweight Myles Jury Rick Glenn Decision (unanimous) (30‐27, 30‐27, 30‐27) 3 5:00 Middleweight Marvin Vettori Omari Akhmedov Draw (majority) (28‐28, 29‐28, 28‐28) 3 5:00 Flyweight Matheus Nicolau Louis Smolka Decision (unanimous) (30‐26, 30‐26, 30‐25) 3 5:00 Bantamweight Tim Elliott Mark De La Rosa Submission (anaconda choke) 2 1:41 For the UFC Women's Featherweight Championship. Event 423 UFC on Fox 26: Lawler vs. dos Anjos December 16, 2017 Winnipeg, Manitoba, Canada Weight Winner Loser Method Round Time Welterweight title eliminator Welterweight Rafael dos Anjos Robbie Lawler Decision (unanimous) (50‐45, 50‐45, 50‐45) 5 5:00 Catchweight 148.5 lb Josh Emmett Ricardo Lamas KO (punch) 1 4:33 Welterweight Santiago Ponzinibbio Mike Perry Decision (unanimous) (29‐28, 29‐28, 29‐28) 3 5:00 Light Heavyweight -
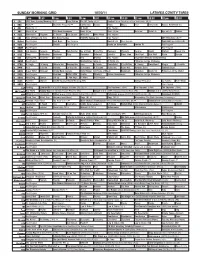
Sunday Morning Grid 10/30/11 Latimes.Com/Tv Times
SUNDAY MORNING GRID 10/30/11 LATIMES.COM/TV TIMES 7 am 7:30 8 am 8:30 9 am 9:30 10 am 10:30 11 am 11:30 12 pm 12:30 2 CBS CBS News Sunday Morning (N) Å Face/Nation The NFL Today (N) Å Football Miami Dolphins at New York Giants. (N) Å 4 NBC News Å Meet the Press (N) Å Conference George House House Paid Travel Cafe Access Hollywood (N) 5 CW News (N) Å In Touch Paid Program 7 ABC News (N) Å This Week-Amanpour News (N) Å News (N) Å News Å Vista L.A. Eye on L.A. Motion 9 KCAL Tomorrow’s Kingdom K. Shook Joel Osteen Ministries Mike Webb Paid Program 11 FOX Hour of Power (N) (TVG) Fox News Sunday FOX NFL Sunday (N) Paid Program UFC Primetime (N) Å 13 MyNet Paid Program Best Buys Paid Program Best of L.A. Paid Program From Hell ›› (2001) (R) 18 KSCI Paid Program Church Paid Program Hecho en Guatemala Iranian TV Paid Program 22 KWHY Paid Program Paid Program 24 KVCR Sid Science Curiosity Thomas Bob Builder Joy of Paint Paint This Dewberry Wyland’s Cuisine Cook’s Kitchen Sweet Life 28 KCET Cons. Wubbulous Busytown Peep Pancakes Pufnstuf Lidsville Place, Own Chef Paul Burt Wolf Pépin Venetia 30 ION Turning Pnt. Discovery In Touch Paid Beyond Paid Program Inspiration Ministry Campmeeting 34 KMEX Paid Program Muchachitas Como Tu Al Punto (N) Fútbol de la Liga Mexicana 40 KTBN K. Hagin Ed Young Miracle-You Redemption Love In Touch PowerPoint It Is Written B. -

Profil Úspěšného Bojovníka MMA
UNIVERZITA KARLOVA V PRAZE FAKULTA TĚLESNÉ VÝCHOVY A SPORTU Profil úspěšného bojovníka MMA Diplomová práce Vedoucí diplomové práce: Vypracovala: PhDr. Radim Pavelka Ph.D. Bc. Renáta Vesecká Prohlašuji, že jsem závěrečnou diplomovou práci zpracovala samostatně a že jsem uvedla všechny použité informační zdroje a literaturu. Tato práce ani její podstatná část nebyla předložena k získání jiného nebo stejného akademického titulu. V Praze, dne …………………………… podpis diplomanta Evidenční list Souhlasím se zapůjčením své diplomové práce ke studijním účelům. Uživatel svým podpisem stvrzuje, že tuto diplomovou práci použil ke studiu a prohlašuje, že ji uvede mezi použitými prameny. Jméno a příjmení: Fakulta / katedra: Datum vypůjčení: Podpis: ______________________________________________________________________ Poděkování Na tomto místě bych ráda poděkovala vedoucímu práce PhDr. Radimovi Pavelkovi, Ph.D. za odborné vedení práce a všem svým konzultantům a samozřejmě rodině za podporu při studiu. Abstrakt Název: Profil úspěšného bojovníka MMA Cíle: Hlavním cílem této práce je sestavení profilu úspěšného bojovníka MMA prestižní organizace UFC, která sdružuje nejúspěšnější bojovníky různých stylů z celého světa. Dalším cílem bylo zjištění, který bojový styl je dnes v těchto prestižních utkáních nejvhodnější vzhledem k úspěšnosti v soutěži. Metody: Jedná se o teoretickou deskriptivní práci. Metodou byla rešeršně kompilační studie z několika dostupných literárních a elektronických zdrojů. Byly uvedeny bojové statistiky a jejich vyhodnocení na základě věcné významnosti. Výsledky: Bylo zjištěno, že nejúspěšnějším stylem současných zápasů MMA organizace UFC je wrestler a dále byl z dostupných informací sestaven profil úspěšného bojovníka MMA. Klíčová slova: MMA, UFC, bojové sporty. Abstract Title: Profile of a successful MMA fighter Objectives: The main objective of this dissertation is to put together a profile of a successful MMA fighter of the prestigious organization UFC which brings together the most successful fighters of various styles from all around the world. -

1 Cain Velasquez Heavyweight 2 Tarec Saffiedine Welterweight 3
Base 1 Cain Velasquez Heavyweight 2 Tarec Saffiedine Welterweight 3 Chan Sung Jung Featherweight 4 Jussier Formiga Flyweight 5 Lyoto Machida Light Heavyweight 6 Vitor Belfort Middleweight 7 Dan Hardy Welterweight 8 Ryan Couture Lightweight 9 Max Holloway Featherweight 10 Siyar Bahadurzada Welterweight 11 Alexis Davis Women's Bantamweight 12 Mike Pierce Welterweight 13 Urijah Faber Bantamweight 14 Nick Ring Middleweight 15 Wanderlei Silva Middleweight 16 Gunnar Nelson Welterweight 17 Cub Swanson Featherweight 18 Johnny Hendricks Welterweight 19 Brian Caraway Bantamweight 20 Rich Franklin Middleweight 21 Ricardo Lamas Featherweight 22 Rustam Khabilov Lightweight 23 Chris Weidman Middleweight 24 Frankie Edgar Featherweight 25 Jose Aldo Featherweight 26 Denis Siver Featherweight 27 Brad Tavares Middleweight 28 Eddie Yagin Featherweight 29 Clay Guida Featherweight 30 Cyrille Diabate Light Heavyweight 31 Raphael Assunçao Bantamweight 32 Nate Diaz Middleweight 33 Brad Pickett Bantamweight 34 Antonio Silva Heavyweight 35 Michael McDonald Bantamweight 36 Renan Barao Bantamweight 37 Ross Pearson Lightweight 38 Chad Mendes Featherweight 39 Pat Barry Heavyweight 40 Carlos Condit Welterweight 41 Fabricio Werdum Heavyweight 42 Khabib Nurmagomedov Lightweight 43 Cat Zingano Women's Bantamweight 44 Rafael dos Anjos Lightweight 45 Hector Lombard Middleweight 46 Mike Rio Lightweight 47 Eddie Wineland Bantamweight 48 TJ Grant Lightweight 49 Akira Corassani Featherweight 50 Mike Pyle Welterweight 51 Erick Silva Welterweight 52 Dominick Cruz Bantamweight 53 Takanori Gomi Lightweight 54 Francis Carmont Middleweight 55 Gray Maynard Lightweight 56 Costa Philippou Middleweight 57 Brian Stann Middleweight 58 Patrick Cote Welterweight 59 Gian Villante Light Heavyweight 60 Josh Barnett Heavyweight 61 Bobby Green Lightweight 62 Joe Lauzon Lightweight 63 Vinny Magalhaes Light Heavyweight 64 Jacare Souza Middleweight 65 Roy Nelson Heavyweight 66 Mike Ricci Lightweight 67 Ovince St. -

Ufc® Interim Bantamweight Champion Renan Barao Set to Clash with Eddie Wineland in Thrilling Matchup on June 15
UFC® INTERIM BANTAMWEIGHT CHAMPION RENAN BARAO SET TO CLASH WITH EDDIE WINELAND IN THRILLING MATCHUP ON JUNE 15 Toronto, Canada – UFC® interim bantamweight champion Renan Barao will look for his second straight title defense against No.4 ranked contender Eddie Wineland on Saturday, June 15 when the Ultimate Fighting Championship® brings its first-ever event to Winnipeg, Manitoba with UFC® 161: BARAO vs. WINELAND at the MTS Centre. Riding one of the longest unbeaten streaks in mixed martial arts history, Barao (32-1, 1NC, fighting out of Rio de Janeiro, Brazil) defeated Urijah Faber in Calgary in July 2012 to win the interim title. He defended the belt in February against Michael McDonald with an impressive arm triangle choke that earned him his first Submission of the Night honours. Barao has gone 31 straight fights without a loss (30 victories, 1 no-contest). He is on an exciting 20-fight win streak and is 5-0 since making his UFC debut in May 2011. Wineland (20-8-1, fighting out of Chesterton, Indiana) is a former WEC bantamweight champion who comes into this title shot with two straight wins. Wineland defeated Scott Jorgensen in June 2012 in a Fight of the Night performance that marked the first time Jorgensen had ever been stopped via knockout. Wineland followed that up with a win over Brad Pickett in December. In the night’s co-main event, light heavyweights Rogerio “Lil Nog” Nogueira and Mauricio “Shogun” Rua, will have a rematch of their legendary 2005 PRIDE® fight. The fifth-ranked Nogueira (21-5, fighting out of Rio de Janeiro, Brazil) has won his last two fights, both of which have been against former UFC® light heavyweight champions. -
1 Ronda Rousey 43 Junior Dos Santos 85 Yushin Okami 2 Thiago Alves 44 Donald Cerrone 86 Bryan Caraway 3 Wagner Prado 45 Urijah F
Base Set 1 Ronda Rousey 43 Junior dos Santos 85 Yushin Okami 2 Thiago Alves 44 Donald Cerrone 86 Bryan Caraway 3 Wagner Prado 45 Urijah Faber 87 Miesha Tate 4 Wanderlei Silva 46 Gunnar Nelson 88 Daniel Cormier 5 Benson Henderson 47 Erick Silva 89 Johny Hendricks 6 Stefan Struve 48 Renan Barao 90 Rory MacDonald 7 Gray Maynard 49 Phil Davis 91 Chris Cariaso 8 BJ Penn 50 Michael McDonald 92 John Dodson 9 Ryan Bader 51 Dennis Siver 93 Khabib Nurmagomedov 10 Ivan Menjivar 52 Max Holloway 94 Erik Koch 11 Jake Shields 53 Tom Watson 95 Dominick Cruz 12 Jay Hieron 54 George Sotiropolis 96 Cain Velasquez 13 Ryan Jimmo 55 Demetrious Johnson 97 Frankie Edgar 14 Nate Diaz 56 Anderson Silva 98 Louis Gaudinot 15 Brian Stann 57 Forrest Griffin 99 Mike Easton 16 Ricardo Lamas 58 Michael Bisping 100 Georges St-Pierre 17 Brad Pickett 59 Jimy Hettes 101 Clay Guida 18 Lyoto Machida 60 Luke Rockhold 102 Dan Henderson 19 Rashad Evans 61 Ian McCall 103 Tim Boetsch 20 Constantinos Phillippou 62 Mark Munoz 104 Jake Ellenberger 21 Antonio Rodrigo Nogueira 63 Diego Brandao 105 Stephen Thompson 22 Nate Marquardt 64 Carlos Condit 106 Travis Browne 23 Anthony Pettis 65 Stipe Miocic 107 Eddie Wineland 24 Nick Diaz 66 Robbie Peralta 108 Sarah Kaufman 25 Jon Jones 67 Charles Oliveira 109 Paul Sass 26 James Te Huna 68 Chael Sonnen 110 Alexander Gustafsson 27 Diego Sanchez 69 Gilbert Melendez 111 Vitor Belfort 28 Chad Mendes 70 Frank Mir 112 Hatsu Hioki 29 Chris Weidman 71 Josh Koscheck 113 Rich Franklin 30 Cub Swanson 72 Brian Ebersole 114 Jon Fitch 31 Mark Hunt 73 Siyar -

Yates Wins Pyrenees Tour Stage
15 FRIDAY, JULY 19, 2019 sports UK MMA Pioneers excited Yates wins Pyrenees Tour stage about Brave’s London event TDT | Manama Simon Yates sprints • RAVE Combat Federa- to fine stage 12 victory as Btion’s first-trip to London, Tour reaches Pyrenees in which the promotion will host an exclusive, invite-only British rider outwits event on July 25th, has a few fellow• escapees on more VIP guests confirmed. Aaron chalmers The British combat sports first Pyrenean stage community will be gathered at the Copper Box Arena, inside Alaphilippe still in the Queen Elizabeth Olympic yellow,• with leaders Park, as more big names have finishing together been confirmed to attend. Both Pickett and Daley have been recognized for the role Brad pickett AFP | Bagneres-de-Bigorre, they have played as ambassa- France dors for the sport in the United Kingdom and as true pioneers ritain’s Simon Yates won of MMA in Europe. Both men stage 12 of the Tour de are big names that have had a BFrance yesterday, beating huge early impact in the mixed two other survivors of a mass martial arts scene in England breakaway in the Pyrenees. and beyond. Paul Daley Defending champion Geraint Great Britain’s Simon Yates celebrates as he wins on the finish line Meanwhile, Aaron Chalm- Thomas and overall leader Ju- ers, a reality show star turned to take MMA to a new level of lian Alaphilippe finished the outwitting his rivals to add this ual time-trial around Pau. MMA fighter has been praised empowerment and influence. slog over two tough climbs Tour de France stage to victories “Everyone was thinking about for turning more eyes to the In the main event of the together as a top 10 shake-up in the Vuelta and Giro. -

P16.E$S Layout 1
MONDAY, FEBRUARY 29, 2016 SPORTS Huck sets sights on Glowacki after Afolabi win BERLIN: Marco Huck has set his sights USA, last August. That was Huck’s first IBF. “The training paid off. I have been crowd courtesy of 116-112 counts in his Well done @RealCFrampton! Fought a on regaining his WBO title after his tech- defeat in six years and after 13 defenses. very diligent and now you have the favour by two judges, with the other giv- smart fight. Get your wallet out nical knock-out win over Britain’s Ola “I really wanted to fight him straight result,” he said. “I’m back again and it’s an ing it to local fighter Quigg 115-113. The @WayneRooney!!,” tweeted the 26-year- Afolabi gave him the IBO cruiserweight away, but now more than ever,” said the indescribable feeling. “When I have hotly-anticipated bout also led to a old. Frampton paid tribute to Quigg belt. Huck became a world champion for 31-year-old Huck, a Serbian-born trained well, no one can beat me in the good-natured Twitter duel between golf with whom he had fought a fierce war of the second time on Saturday night German, as he chases Glowacki for a ring.” star McIlroy and Manchester United words in the build-up to the fight-over when Afolabi, 35, retired after failing to rematch. striker Rooney. “Both top fighters mate the choice of dressing rooms. “That’s the come out for the 11th round in Halle, “We offered him a bag of money, but McIlroy tops Rooney but @scottquigg for me. -

UFC® on FUEL TV OFFICAL WEIGH-IN RESULTS
UFC® on FUEL TV OFFICAL WEIGH-IN RESULTS Las Vegas, Nevada – The Ultimate Fighting Championship® organization returns to FUEL TV tomorrow with what UFC president Dana White called one of the best televised cards of the year. All 22 fighters have weighed-in, and are ready to fight tomorrow. Emanating from the Capital FM Arena in the historic City of Nottingham, England, the FUEL TV televised event features six sick fights including a heavyweight eliminator, a clash between a hometown hero and an Ultimate Fighter winner, an all-British welterweight battle, a bantamweight clash between a top five contender and an exciting talent looking to make a name for himself, an undefeated lightweight prodigy taking on a four-time ‘fight of the night’ winner, plus, a throwdown between two ‘bombs away’ welterweight punchers. “If you don’t think this is a great card – you know nothing about mixed martial arts because this card is awesome,” said White. “The main event between Struve and Miocic is awesome and the winner of this fight becomes a top five heavyweight. These are the fights you have to win to get the world title – and it should be a great fight. These two have gone to a decision only once each – it could be the fight of the night. But I could say that about all the fights, though. You could throw a dart at the card and hit the fight of the night. Dan Hardy always, always brings it, and so does Amir Sadollah. That should be great too, especially with Dan fighting in front of his hometown fans. -

World Extreme Cagefighting
World Extreme Cagefighting Event WEC 53: Henderson vs. Pettis December 16, 2010 Jobing.com Arena WEC 52: Faber vs. Mizugaki November 11, 2010 The Pearl at The Palms WEC 51: Aldo vs. Gamburyan September 30, 2010 1stBank Center WEC 50: Cruz vs. Benavidez August 18, 2010 The Pearl at The Palms WEC 49: Varner vs. Shalorus June 20, 2010 Rexall Place WEC 48: Aldo vs. Faber April 24, 2010 ARCO Arena WEC 47: Bowles vs. Cruz March 6, 2010 Nationwide Arena WEC 46: Varner vs. Henderson January 10, 2010 ARCO Arena WEC 45: Cerrone vs. Ratcliff December 19, 2009 The Pearl at The Palms WEC 44: Brown vs. Aldo November 18, 2009 The Pearl at The Palms WEC 43: Cerrone vs. Henderson October 10, 2009 AT&T Center WEC 42: Torres vs. Bowles August 9, 2009 Hard Rock Hotel and Casino WEC 41: Brown vs. Faber II June 7, 2009 ARCO Arena WEC 40: Torres vs. Mizugaki April 5, 2009 UIC Pavilion WEC 39: Brown vs. Garcia March 1, 2009 American Bank Center WEC 38: Varner vs. Cerrone January 25, 2009 San Diego Sports Arena WEC 37: Torres vs. Tapia December 3, 2008 Hard Rock Hotel and Casino WEC 36: Faber vs. Brown November 5, 2008 Seminole Hard Rock Hotel and Casino WEC 35: Condit vs. Miura August 3, 2008 Hard Rock Hotel and Casino WEC 34: Faber vs. Pulver June 1, 2008 ARCO Arena WEC 33: Marshall vs. Stann March 26, 2008 Hard Rock Hotel and Casino WEC 32: Condit vs. Prater February 13, 2008 Santa Ana Star Center WEC 31: Faber vs.