Anatomical Arrangement of the Subclavian Artery Branches in the Rabbit and European Hare
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ipsilateral Subclavian Steal in Association with Aberrant Origin of the Left Vertebral Artery from the Aortic Arch
411 Ipsilateral Subclavian Steal in Association with Aberrant Origin of the Left Vertebral Artery from the Aortic Arch John Holder1 Five cases are reported of left subclavian steal syndrome associated with anomalous Eugene F. Binet2 origin of the left vertebral artery from the aortic arch. In all five instances blood flow at Bernard Thompson3 the origin of the left vertebral artery was in an antegrade direction contrary to that usually reported in this condition. The distal subclavian artery was supplied via an extensive collateral network of vessels connecting the vertebral artery to the thyro cervical trunk. If a significant stenosis or occlusion is present within the left subc lavi an artery proximal to the origin of the left vertebral artery, the direction of the bl ood fl ow within the vertebral artery will reverse toward the parent vessel (retrograde flow). This phenomenon occurs when a negative pressure gradient of 20-40 torr exists between the vertebral-basilar artery junction and th e vertebral-subc lavian artery junction [1-3]. We describe five cases of subclavian steal confirmed by angiography where a significant stenosis or occlusion of the left subclavian artery was demonstrated in association with anomalous origin of th e left vertebral artery directly from the aortic arch. In all five cases blood flow at the origin of the left vertebral artery was in an antegrade direction contrary to that more commonly reported in the subclavian steal syndrome. Materials and Methods The five patients were all 44- 58-year-old men. Three sought medical attention for symptoms specificall y related to th e left arm . -

Vessels and Circulation
CARDIOVASCULAR SYSTEM OUTLINE 23.1 Anatomy of Blood Vessels 684 23.1a Blood Vessel Tunics 684 23.1b Arteries 685 23.1c Capillaries 688 23 23.1d Veins 689 23.2 Blood Pressure 691 23.3 Systemic Circulation 692 Vessels and 23.3a General Arterial Flow Out of the Heart 693 23.3b General Venous Return to the Heart 693 23.3c Blood Flow Through the Head and Neck 693 23.3d Blood Flow Through the Thoracic and Abdominal Walls 697 23.3e Blood Flow Through the Thoracic Organs 700 Circulation 23.3f Blood Flow Through the Gastrointestinal Tract 701 23.3g Blood Flow Through the Posterior Abdominal Organs, Pelvis, and Perineum 705 23.3h Blood Flow Through the Upper Limb 705 23.3i Blood Flow Through the Lower Limb 709 23.4 Pulmonary Circulation 712 23.5 Review of Heart, Systemic, and Pulmonary Circulation 714 23.6 Aging and the Cardiovascular System 715 23.7 Blood Vessel Development 716 23.7a Artery Development 716 23.7b Vein Development 717 23.7c Comparison of Fetal and Postnatal Circulation 718 MODULE 9: CARDIOVASCULAR SYSTEM mck78097_ch23_683-723.indd 683 2/14/11 4:31 PM 684 Chapter Twenty-Three Vessels and Circulation lood vessels are analogous to highways—they are an efficient larger as they merge and come closer to the heart. The site where B mode of transport for oxygen, carbon dioxide, nutrients, hor- two or more arteries (or two or more veins) converge to supply the mones, and waste products to and from body tissues. The heart is same body region is called an anastomosis (ă-nas ′tō -mō′ sis; pl., the mechanical pump that propels the blood through the vessels. -

Cervical Arterial Collateral Network References Reply: Reference Age
Cervical Arterial Collateral Network Age and Gender Effects on Normal Regional Cerebral Purkayastha et al1 reported 3 cases of proatlantal intersegmental Blood Flow arteries of external carotid artery origin associated with Galen’s vein We read with great interest the article of Takahashi et al.1 The article malformation; however, because of their configuration, I believe that points out the use of 3D stereotactic surface projections (3D-SSP) to the 3 cases do not demonstrate this rare arterial variation, but rather study the age-effect on regional cerebral blood flow (rCBF). The show collateral blood flow from the occipital artery (OA) to the ver- greatest rCBF reduction observed was in the bilateral anterior cingu- tebral artery (VA). In patients with a vein of Galen malformation, the late. Although we generally agree with the conclusions, we would like intra-arterial blood pressure in the VA is lower than that in the OA to emphasize some methodologic issues that may have had an impact because of blood steal phenomenon at the malformation. It is well on the obtained results. known that there is a cervical arterial collateral network between OA, In the study, 31 healthy volunteers between 50 and 79 years were classified in 3 different age classes (50–59, 60–69, and 70–79 years). VA, and the deep cervical artery arising from the subclavian artery.2 If Statistical analysis was performed 2 by 2 by using unpaired Student t test. one of these arteries is occluded, the remaining arteries and their Rather than considering age as a discrete variable, the analysis would have branches are dilated and supply the distal segment of the occluded been strengthened by performing a multivariate analysis based on the artery. -

The Variations of the Subclavian Artery and Its Branches Ahmet H
Okajimas Folia Anat. Jpn., 76(5): 255-262, December, 1999 The Variations of the Subclavian Artery and Its Branches By Ahmet H. YUCEL, Emine KIZILKANAT and CengizO. OZDEMIR Department of Anatomy, Faculty of Medicine, Cukurova University, 01330 Balcali, Adana Turkey -Received for Publication, June 19,1999- Key Words: Subclavian artery, Vertebral artery, Arterial variation Summary: This study reports important variations in branches of the subclavian artery in a singular cadaver. The origin of the left vertebral artery was from the aortic arch. On the right side, no thyrocervical trunk was found. The two branches which normally originate from the thyrocervical trunk had a different origin. The transverse cervical artery arose directly from the subclavian artery and suprascapular artery originated from the internal thoracic artery. This variation provides a short route for posterior scapular anastomoses. An awareness of this rare variation is important because this area is used for diagnostic and surgical procedures. The subclavian artery, the main artery of the The variations of the subclavian artery and its upper extremity, also gives off the branches which branches have a great importance both in blood supply the neck region. The right subclavian arises vessels surgery and in angiographic investigations. from the brachiocephalic trunk, the left from the aortic arch. Because of this, the first part of the right and left subclavian arteries differs both in the Subjects origin and length. The branches of the subclavian artery are vertebral artery, internal thoracic artery, This work is based on a dissection carried out in thyrocervical trunk, costocervical trunk and dorsal the Department of Anatomy in the Faculty of scapular artery. -

The Descending Thoracic Aorta Morphological Characteristics
ARS Medica Tomitana - 2016; 3(22): 186 - 191 10.1515/arsm-2016-0031 Malik S., Bordei P., Rusali A., Iliescu D. M. The descending thoracic aorta morphological characteristics Faculty of Medicine, “Ovidius” University, Constanta ABSTRACT Introduction Our study was conducted by consulting angioCT sites made on a CT GE LightSpeed VCT64 Slice CT and a CT GE LightSpeed 16 Slice CT, following the path and relationships of the descending thoracic aorta against the vertebral column, outside diameters thereof at the Descending thoracic aorta extends from the thoracic vertebrae T4, T7, T12 and posterior intercostal aortic arch (which it continues) and aortic hiatus of arteries characteristics. The origin of of the descending the diaphragm at level of T12 vertebra [1,2,3,4,5] thoracic aorta we found most commonly on the left corresponding to the front of T10 [6], level that flank of the lower edge of the vertebral body T4, but continues with the abdominal descending aorta. She I have encountered cases where it had come above the enters the posterior mediastinum at the T4 vertebra and lower edge of T4 on level of intervertebral disc T4-T5 or describes a trajectory which is vertically downward as even at the upper edge of T5 vertebral body. At thoracic a whole, being slightly inferior oblique and to the right, vertebra T4, on a total of 30 cases, the descending thoracic aorta present a diameter of 20.0 to 32.6 mm, then, first at a distance of 2-3 cm midline, progressive values that correspond to male gender and to females approach to become median and prevertebral at the diameter ranging from 25.5 to 27, 4 mm. -

Embolization for Hemoptysis—Angiographic Anatomy of Bronchial and Systemic Arteries
THIEME 184 Pictorial Essay Embolization for Hemoptysis—Angiographic Anatomy of Bronchial and Systemic Arteries Vikash Srinivasaiah Setty Chennur1 Kumar Kempegowda Shashi1 Stephen Edward Ryan1 1 1 Adnan Hadziomerovic Ashish Gupta 1Division of Angio-Interventional Radiology, Department of Medical Address for correspondence Ashish Gupta, MD, Division of Imaging, University of Ottawa, The Ottawa Hospital, Ottawa, Angio-Interventional Radiology, Department of Medical Imaging, Ontario, Canada University of Ottawa, The Ottawa Hospital, 501 Smyth Road, Ottawa, ON K1H 8L6, Canada (e-mail: [email protected]). J Clin Interv Radiol ISVIR 2018;2:184–190 Abstract Massive hemoptysis is a potentially fatal respiratory emergency. The majority of these patients are referred to interventional radiology for bronchial artery embolization (BAE). Immediate clinical success in stopping hemoptysis ranges from 70 to 99%. However, recurrent hemoptysis after BAE is seen in 10 to 55% patients. One of the main reasons for recurrence is incomplete embolization due to unidentified aberrant Keywords bronchial and/or non-bronchial systemic arterial supply. This pictorial essay aims to ► bronchial describe the normal and variant bronchial arterial anatomy and non-bronchial systemic ► embolization arterial feeders to the lungs on conventional angiography; the knowledge of which is ► hemoptysis critical for interventional radiologists involved in the care of patients with hemoptysis. Introduction Angiographic Anatomy of Bronchial Arteries Massive hemoptysis is a respiratory -
The Vertebral Artery in the Vascular Lab: What Does It Mean?
The Vertebral Artery in the Vascular Lab: What Does It Mean? Caron Rockman MD Frances and Joseph Ritroto Professor of Surgery Program Director, Vascular Surgery New York University Langone Medical Center Disclosures •None Division of Vascular and Endovascular Surgery Subclavian Steal Occlusion of proximal Subclavian Art Vertebral artery supplies retrograde flow Posterior brain receives decreased flow 55 years + Men > Women more than 2:1 LSA affected 3x more than RSA Division of Vascular and Endovascular Surgery Subclavian Steal Causes: - Arteriosclerosis of subclavian artery (>95% cases) - Embolism - Takayasu’s Arteritis -Dissecting Aneurysm Risk Factors: (similar to CAD) -Smoking -Hypertension -Hyperlipidemia -Hypertension Division of Vascular and Endovascular Surgery Symptoms of Subclavian Steal Vertebrobasilar Insufficiency (posterior circulation symptoms) Light headedness or dizziness Ataxia or Vertigo Visual Disturbance Headache Syncope Confusion Division of Vascular and Endovascular Surgery Symptoms of Subclavian Steal Subclavian Insufficiency Arm weakness, coldness Numbness or “tingling” Arm Claudication with exercise Symptoms can be exacerbated with: Vigorous exercise Sudden turning of head to affected side Division of Vascular and Endovascular Surgery Signs of Subclavian Steal Diminished pulses (radial/ulnar) Discrepant blood pressures in upper extremities (>20mmHg) (Pitfall with bilateral disease) Subclavian Bruit 7 Division of Vascular and Endovascular Surgery Subclavian steal on Duplex Exam Incomplete steal •Striking deceleration of velocity in mid or late systole •High grade stenosis of subclavian rather than occlusion Complete Steal •Complete reversal of flow within the vertebral artery Division of Vascular and Endovascular Surgery Vertebral Retrograde Flow • Reversal of flow in the vertebral artery is a common finding identified on cerebrovascular duplex ultrasound. • The clinical significance and natural history of patients presenting with this finding, however, is poorly understood. -

Intercostal Arteries a Single Posterior & Two Anterior Intercostal Arteries
Intercostal Arteries •Each intercostal space contains: . A single posterior & .Two anterior intercostal arteries •Each artery gives off branches to the muscles, skin, parietal pleura Posterior Intercostal Arteries In the upper two spaces, arise from the superior intercostal artery (a branch of costocervical trunk of the subclavian artery) In the lower nine spaces, arise from the branches of thoracic aorta The course and branching of the intercostal arteries follow the intercostal Posterior intercostal artery Course of intercostal vessels in the posterior thoracic wall Anterior Intercostal Arteries In the upper six spaces, arise from the internal thoracic artery In the lower three spaces arise from the musculophrenic artery (one of the terminal branch of internal thoracic) Form anastomosis with the posterior intercostal arteries Intercostal Veins Accompany intercostal arteries and nerves Each space has posterior & anterior intercostal veins Eleven posterior intercostal and one subcostal vein Lie deepest in the costal grooves Contain valves which direct the blood posteriorly Posterior Intercostal Veins On right side: • The first space drains into the right brachiocephalic vein • Rest of the intercostal spaces drain into the azygos vein On left side: • The upper three spaces drain into the left brachiocephalic vein. • Rest of the intercostal spaces drain into the hemiazygos and accessory hemiazygos veins, which drain into the azygos vein Anterior Intercostal Veins • The lower five spaces drain into the musculophrenic vein (one of the tributary of internal thoracic vein) • The upper six spaces drain into the internal thoracic vein • The internal thoracic vein drains into the subclavian vein. Lymphatics • Anteriorly drain into anterior intercostal nodes that lie along the internal thoracic artery • Posterioly drain into posterior intercostal nodes that lie in the posterior mediastinum . -

A Functional Perspective on the Embryology and Anatomy of the Cerebral Blood Supply
Journal of Stroke 2015;17(2):144-158 http://dx.doi.org/10.5853/jos.2015.17.2.144 Review A Functional Perspective on the Embryology and Anatomy of the Cerebral Blood Supply Khaled Menshawi,* Jay P Mohr, Jose Gutierrez Department of Neurology, Columbia University Medical Center, New York, NY, USA The anatomy of the arterial system supplying blood to the brain can influence the develop- Correspondence: Jose Gutierrez ment of arterial disease such as aneurysms, dolichoectasia and atherosclerosis. As the arteries Department of Neurology, Columbia University Medical Center, 710 W 168th supplying blood to the brain develop during embryogenesis, variation in their anatomy may Street, New York, NY, 10032, USA occur and this variation may influence the development of arterial disease. Angiogenesis, Tel: +1-212-305-1710 Fax: +1-212-305-3741 which occurs mainly by sprouting of parent arteries, is the first stage at which variations can E-mail: [email protected] occur. At day 24 of embryological life, the internal carotid artery is the first artery to form and it provides all the blood required by the primitive brain. As the occipital region, brain Received: December 18, 2014 Revised: February 26, 2015 stem and cerebellum enlarge; the internal carotid supply becomes insufficient, triggering the Accepted: February 27, 2015 development of the posterior circulation. At this stage, the posterior circulation consists of a primitive mesh of arterial networks that originate from projection of penetrators from the *This work was done while Mr. Menshawi was visiting research fellow at Columbia distal carotid artery and more proximally from carotid-vertebrobasilar anastomoses. -
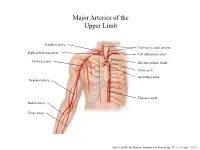
Major Arteries of the Upper Limb
Major Arteries of the Upper Limb Vertebral artery Common carotid arteries Right subclavian artery Left subclavian artery Axillary artery Brachiocephalic trunk Aortic arch Ascending aorta Brachial artery Thoracic aorta Radial artery Ulnar artery Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.23 Major Arteries of the Abdominal Region Renal artery Celiac trunk Abdominal aorta Superior mesenteric artery Gonadal artery Inferior mesenteric artery Common iliac artery Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.24 Common iliac artery Internal iliac artery Major Arteries of the External iliac artery Lower Limb Femoral artery Popliteal artery Anterior tibial artery Fibular artery Posterior tibial artery Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.25 Major Veins of the Upper Limb Internal jugular vein (left) Subclavian vein (right) External jugular vein (left) Axillary vein Brachiocephalic veins Cephalic vein Superior vena cava Brachial vein Basilic vein Median cubital vein Inferior vena cava Radial vein Ulnar vein Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.28 Major Veins of the Abdominal Cavity – Part 1 Hepatic veins Inferior vena cava Renal vein (left) Gonadal vein (left) Gonadal vein (right) Common iliac vein (left) Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.29 Major Veins of the Abdominal Cavity – Part 2 (Hepatic portal circulation) Hepatic portal vein Splenic vein Inferior mesenteric vein Superior mesenteric vein Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.29 Common iliac vein (left) Internal iliac vein Major Veins of the External iliac vein Lower Limb Great saphenous vein Femoral vein Popliteal vein Fibular vein Small saphenous vein Anterior tibial Posterior tibial vein vein Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.30 . -

Comparing the Organs and Vasculature of the Head and Neck
in vivo 31 : 861-871 (2017) doi:10.21873/invivo.11140 Comparing the Organs and Vasculature of the Head and Neck in Five Murine Species MIN JAE KIM 1* , YOO YEON KIM 2* , JANET REN CHAO 3, HAE SANG PARK 1,4 , JIWON CHANG 1,4 , DAWOON OH 5, JAE JUN LEE 4,6 , TAE CHUN KANG 7, JUN-GYO SUH 2 and JUN HO LEE 1,4 1Department of Otorhinolaryngology-Head and Neck Surgery, College of Medicine, Hallym University, Chuncheon, Republic of Korea; 2Department of Medical Genetics, College of Medicine, Hallym University, Chuncheon, Republic of Korea; 3School of Medicine, George Washington University, Washington, DC, U.S.A.; 4Institute of New Frontier Research, Hallym University College of Medicine, Chuncheon, Republic of Korea; 5Department of Anesthesiology and Pain Medicine, Dongtan Sacred Heart Hospital, Hallym University, Dongtan, Republic of Korea; 6Department of Anesthesiology and Pain Medicine, College of Medicine, Hallym University, Chuncheon, Republic of Korea; 7Department of Anatomy and Neurobiology, College of Medicine, Hallym University, Chuncheon, Republic of Korea Abstract. Background/Aim: The purpose of the present Unique morphological characteristics were demonstrated by study was to delineate the cervical and facial vascular and comparing the five species, including symmetry of the associated anatomy in five murine species, and compare common carotid origin bilaterally in the Mongolian Gerbil, them for optimal use in research studies focused on a large submandibular gland in the hamster and an enlarged understanding the pathology and treatment of diseases in buccal branch in the Guinea Pig. In reviewing the humans. Materials and Methods: The specific adult male anatomical details, this staining technique proves superior animals examined were mice (C57BL/6J), rats (F344), for direct surgical visualization and identification. -

Aorta and the Vasculature of the Thorax
Aorta and the Vasculature of the Thorax Ali Fırat Esmer, MD Ankara University Faculty of Medicine Department of Anatomy THE AORTA After originating from left ventricle, it ascends for a short distance, arches backward and to the left side, descends within the thorax on the left side of the vertebral column It is divided for purposes of The aorta is the main arterial trunk description into: that delivers oxygenated blood from Ascending aorta the left ventricle of the heart to the Arch of the aorta and tissues of the body. Descending aorta (thoracic and abdominal aorta) Ascending Aorta The ascending aorta begins at the base of the left ventricle runs upward and forward at the level of the sternal angle, where it becomes continuous with the arch of the aorta it possesses three bulges, the sinuses of the aorta Branches Right coronary artery Left coronary artery ARCH OF THE AORTA The aortic arch is a continuation of the ascending aorta and begins at the level of the second sternocostal joint. • It arches superiorly, posteriorly and to the left before moving inferiorly. • The aortic arch ends at the level of the T4 vertebra / at level of sternal angle. Branches; Brachiocephalic artery (Innominate artery) Left common carotid artery Left subclavian artery It begins when the ascending aorta emerges from the pericardial sac and courses upward, backward, and to the left as it passes through the superior mediastinum, ending on the left side at vertebral level TIV/V. Extending as high as the midlevel of the manubrium of the sternum, the arch is initially anterior and finally lateral to the trachea.