Meteorology) By
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Sr. No College Name District Gender Division Contact 1 GOVT
Sr. College Name District Gender Division Contact No 1 GOVT. COLLEGE FOR WOMEN ATTOCK ATTOCK Female RAWALPINDI 572613336 2 GOVT. DEGREE COLLEGE FOR WOMEN FATEH JANG, ATTOCK ATTOCK Female RAWALPINDI 572212505 3 GOVT. COLLEGE FOR WOMEN PINDI GHEB, ATTOCK ATTOCK Female RAWALPINDI 4 GOVT. DEGREE COLLEGE FOR WOMEN, JAND ATTOCK ATTOCK Female RAWALPINDI 572621847 5 GOVT. DEGREE COLLEGE FOR WOMEN HASSAN ABDAL ATTOCK ATTOCK Female RAWALPINDI 6 GOVT. DEGREE COLLEGE FOR WOMEN HAZRO, ATTOCK ATTOCK Female RAWALPINDI 572312884 7 GOVT. POST GRADUATE COLLEGE ATTOCK ATTOCK Male RAWALPINDI 579316163 8 Govt. Commerce College, Attock ATTOCK Male RAWALPINDI 9 GOVT. DEGREE COLLEGE FATEH JANG ATTOCK ATTOCK Male RAWALPINDI 10 GOVT. INTER COLLEGE OF BOYS, BAHTAR, ATTOCK ATTOCK Male RAWALPINDI 11 GOVT. DEGREE COLLEGE (BOYS) PINDI GHEB ATTOCK ATTOCK Male RAWALPINDI 572352909 12 Govt. Institute of Commerce, Pindigheb ATTOCK Male RAWALPINDI 572352470 13 GOVT. DEGREE COLLEGE BOYS, JAND, ATTOCK ATTOCK Male RAWALPINDI 572622310 14 GOVT. INTER COLLEGE NARRAH KANJOOR CHHAB ATTOCK ATTOCK Male RAWALPINDI 572624005 15 GOVT. DEGREE COLLEGE BASAL ATTOCK ATTOCK Male RAWALPINDI 572631414 16 Govt. Institute of Commerce, Jand ATTOCK Male RAWALPINDI 572621186 17 GOVT. DEGREE COLLEGE FOR BOYS HASSAN ABDAL, ATTOCK ATTOCK Male RAWALPINDI 18 GOVT.SHUJA KHANZADA SHAHEED DEGREE COLLEGE, HAZRO, ATTOCK ATTOCK Male RAWALPINDI 572312612 19 GOVT. COLLEGE FOR WOMEN CHAKWAL CHAKWAL Female RAWALPINDI 543550957 20 GOVT. DEGREE COLLEGE FOR WOMEN , DHADIAL , CHAKWAL CHAKWAL Female RAWALPINDI 543590066 21 GOVT. DEGREE COLLEGE FOR WOMEN MULHAL MUGHLAN, CHAKWAL CHAKWAL Female RAWALPINDI 543585081 22 GOVT. DEGREE COLLEGE FOR WOMEN BALKASSAR , CHAKWAL CHAKWAL Female RAWALPINDI 543569888 23 Govt Degree College for women Ara Basharat tehsil choa Saidan Shah chakwal CHAKWAL Female RAWALPINDI 543579210 24 GOVT. -

Eid-Ul-Adha Plan
Eid ul Adha Plan 2017 Page 0 PREFACE This is LWMC’s Eid-ul-Azha plan 2017. This plan will cover detailed information regarding Solid Waste Management (SWM) services, which shall be provided by LWMC during Eid days. LWMC is going to make special arrangements for Solid Waste Management (SWM) on the eve of Eid-ul-Azha. LWMC in coordination with Turkish Contractors (M/s. Albayrak & M/s. Ozpak) will attempt to offer exemplary cleanliness arrangements on the eve of Eid-ul-Azha. The standard SWM activities will mainly focus on prompt collection, storage, transportation and disposal of animal waste during all three days of Eid. All the staff of LWMC will remain on board during Eid days to provide efficient SWM services to the citizens of Lahore. LWMC will establish Eid Camps in each Union Council of Lahore, not only to address the complaints of the citizens but to efficiently coordinate cleanliness activities in the respective UC’s as well. Moreover, awareness material and garbage bags for animal waste will also be available in these camps. A control room will be established in LWMC head office with special focus to coordinate collective operational activities during Eid days. In order to manage animal waste, LWMC is going to distribute 2 Million garbage bags in Lahore. The garbage bags will be made available free of cost in respective UC Camps / Zonal Office, Major Masajids / Eid Gahs. Similarly, for prompt collection of animal waste, LWMC will hire pickups 2 days before Eid for garbage bag distribution, awareness & waste collection. 1089 pickups will be hired on first day, 1025 on second and 543 on third day of Eid. -

GIPE-071956.Pdf (4.127Mb)
1$oarb of Ql!ronomit Jlnquirp ~unjab (iaakistan) PUBLICATION No. 111 General Editor : Prof. M. HASSAN SOIL EROSION. IN THE PUNJAB Suroeyed by ABDUL AZIZ ANWAR, M.A., LL.B. 1955 Pri~e:-, Rs. 1/8/- Taoarb of Qeronomic;·~nqui~p 1)lunjah (~akistan~ PUBLICATION No. 111 ' ' General Editor : Prof. M. HASSAN SOIL EROSION IN THE PUNJAB Suroeyed by ABDUL AZIZ ANWAR, M.A., LL.B. 1955 (The Board of Eoonomio Inquiry, Punjab (Pakis\an), does not hold itself reaponsible for uy opinion e:z:preSBed or conclusions reached by the writ.er). PREFACE Soil erosion is called the 'creeping death' of the soil. It is a world-wide problem, but it is much more assertive in under developed countries where the modern discoveries in scientific know ledge have not been applied commensurate with their needs in agriculture. It works out its serious effects through this process : loss of surface soil, plant-food and sub-soil water, silting up of water channels, disruption of communications, reduction in productivity of land and ultimately lowering the already low standard of living of the peasantry. Soil erosion has affected vast areas of our fertile land, rendering them completely unfit for cultivation. In Rawalpindi Division alone about 5 lakh acres of productive land have become uncultivable while another 10 Jakh acres are seriously affected. The menace of soil erosion is fast spreading. 1t needs effective measures for combating it. It need hardly be emphasiseC: that soil is a basic national resource and its conservation is the prime necessity. For, without ita due care, we may not be left with enough land to raise food and commercial crops for our growing economy. -

Corporate Class)
PROVISIONAL LIST OF VOTERS 2021 (CORPORATE CLASS) 00001 101 GROUP (PVT) LTD 00002 1ST 4 CONNECT (PVT) LTD. 131-Y, COMMERCIAL AREA, PHASE-III, DHA, LAHORE 2ND FLOOR, ASHRAF PLAZA, 17, MCLEOD ROAD, LAHORE MR. FARRUKH SAEED - Chief Executive MR. WALEED SANAULLAH - Director Phone:042-35694723,042-35694724 Phone:___-________,___-________ NTN: 2938238-6 CNIC: 35202-5032175-5 NTN: 3754572-8 CNIC: 35202-5378534-5 GSTN: 3277876134468 Mship #: 85703 - C GSTN: Mship #: 76068 - C 00003 2-K ENGINEERING (PVT) LTD 00004 3-A ENTERPRISES KHASRA # 2871, OPPOSITE MIAN TOWN UNDER PASS, 295- UPPER MALL SCHEME, LAHORE NEAR SHARIF PURA, QABRISTAN, BHAINI ROAD, LAKHO DAIR, LAHORE MR. MUHAMMAD ASHAQUE RAMAY - Partner MR. KHALID IDREES - Chief Executive Phone:___-________,___-________ Phone:042-35754112,042-35750441 NTN: 3679340-0 CNIC: 35202-2384379-1 NTN: 3059196-1 CNIC: 35202-2379267-5 GSTN: 03-00-3679-340-19 Mship #: 64825 - C GSTN: 03-92-9999-866 Mship #: 5251 - C 00005 4 M (PVT) LTD 00006 4 SQUARE COMMUNICATION (PVT.) LTD 15-L, 2ND FLOOR, COMMERCIAL AREA,PHASE-I, DHA, 180-Y, COMMERCIAL, PHASE-III, D.H.A., LAHORE LAHORE MR. ATA UR REHMAN - Chief Executive SYED SHAD MUSTAFA - Director Phone:042-35732134,042-35732135 Phone:042-35692615,042-35692616 NTN: 2632575-6 CNIC: 35201-7026056-3 NTN: 3539182-7 CNIC: 35200-1495763-5 GSTN: Mship #: 63214 - C GSTN: Mship #: 97652 - C 00007 49TH NORTH (SMC-PVT) LTD 00008 4B GENTEL INTERNATIONAL (PVT) LTD HOUSE NO.147-B, IZMIR SOCIETY, CANAL BANK, OFF 77-D/1, IST FLOOR, LAHORE CENTRE,MAIN MULTAN ROAD, LAHORE BOULEVARD, GULBERG III, LAHORE MR. -
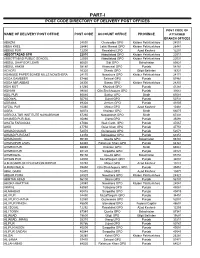
Part-I: Post Code Directory of Delivery Post Offices
PART-I POST CODE DIRECTORY OF DELIVERY POST OFFICES POST CODE OF NAME OF DELIVERY POST OFFICE POST CODE ACCOUNT OFFICE PROVINCE ATTACHED BRANCH OFFICES ABAZAI 24550 Charsadda GPO Khyber Pakhtunkhwa 24551 ABBA KHEL 28440 Lakki Marwat GPO Khyber Pakhtunkhwa 28441 ABBAS PUR 12200 Rawalakot GPO Azad Kashmir 12201 ABBOTTABAD GPO 22010 Abbottabad GPO Khyber Pakhtunkhwa 22011 ABBOTTABAD PUBLIC SCHOOL 22030 Abbottabad GPO Khyber Pakhtunkhwa 22031 ABDUL GHAFOOR LEHRI 80820 Sibi GPO Balochistan 80821 ABDUL HAKIM 58180 Khanewal GPO Punjab 58181 ACHORI 16320 Skardu GPO Gilgit Baltistan 16321 ADAMJEE PAPER BOARD MILLS NOWSHERA 24170 Nowshera GPO Khyber Pakhtunkhwa 24171 ADDA GAMBEER 57460 Sahiwal GPO Punjab 57461 ADDA MIR ABBAS 28300 Bannu GPO Khyber Pakhtunkhwa 28301 ADHI KOT 41260 Khushab GPO Punjab 41261 ADHIAN 39060 Qila Sheikhupura GPO Punjab 39061 ADIL PUR 65080 Sukkur GPO Sindh 65081 ADOWAL 50730 Gujrat GPO Punjab 50731 ADRANA 49304 Jhelum GPO Punjab 49305 AFZAL PUR 10360 Mirpur GPO Azad Kashmir 10361 AGRA 66074 Khairpur GPO Sindh 66075 AGRICULTUR INSTITUTE NAWABSHAH 67230 Nawabshah GPO Sindh 67231 AHAMED PUR SIAL 35090 Jhang GPO Punjab 35091 AHATA FAROOQIA 47066 Wah Cantt. GPO Punjab 47067 AHDI 47750 Gujar Khan GPO Punjab 47751 AHMAD NAGAR 52070 Gujranwala GPO Punjab 52071 AHMAD PUR EAST 63350 Bahawalpur GPO Punjab 63351 AHMADOON 96100 Quetta GPO Balochistan 96101 AHMADPUR LAMA 64380 Rahimyar Khan GPO Punjab 64381 AHMED PUR 66040 Khairpur GPO Sindh 66041 AHMED PUR 40120 Sargodha GPO Punjab 40121 AHMEDWAL 95150 Quetta GPO Balochistan 95151 -

The Study on Improvement of Management Information Systems in Health Sector in the Islamic Republic of Pakistan Dhis Manual
JAPAN INTERNATIONAL COOPERATION AGENCY (JICA) MINISTRY OF HEALTH, ISLAMIC REPUBLIC OF PAKISTAN THE STUDY ON IMPROVEMENT OF MANAGEMENT INFORMATION SYSTEMS IN HEALTH SECTOR IN THE ISLAMIC REPUBLIC OF PAKISTAN DHIS MANUAL FEBRUARY 2007 NATIONAL HEALTH INFORMATION RESOURCE CENTER HM SYSTEM SCIENCE CONSULTANTS INC. JR 06-46 Japan International Cooperation Agency Ministry of Health, Islamic Republic of Pakistan THE STUDY ON IMPROVEMENT OF MANAGEMENT INFORMATION SYSTEMS IN HEALTH SECTOR IN THE ISLAMIC REPUBLIC OF PAKISTAN FINAL REPORT DHIS MANUAL February 2007 System Science Consultants Inc PART I PROCEDURES MANUAL Procedures Manual For District Health Information System (DHIS) Pakistan The Study on Improvement of Management Information Systems in Health Sector in the Islamic Republic of Pakistan National Health Information Resource Center, Ministry of Health, Pakistan Japan International Cooperation Agency (JICA) Systems Science Consultants, Inc. Contents Table 1 List of DHIS Instruments......................................................................................1 Table 2 When and Who Fills the DHIS Instruments.........................................................2 Table 3 Source of Data for DHIS Monthly Reports ........................................................82 Table 4 Detail Description of Data Source for DHIS Monthly Report ...........................83 Procedures Manual 1. Central Registration Point Register .................................................................................4 2. OPD Ticket ....................................................................................................................8 -

FLOOD RISK ASSESSMENT REPORT a Hi-Tech Knowledge Management Tool for Disaster Risk Assessment at UNION COUNCIL Level
2015 FLOOD RISK ASSESSMENT REPORT A Hi-Tech Knowledge Management Tool for Disaster Risk Assessment at UNION COUNCIL Level A PROPOSAL IN VIEW OF LESSONS LEARNED ISBN (P) 978-969-638-093-1 ISBN (D) 978-969-638-094-8 205-C 2nd Floor, Evacuee Trust Complex, F-5/1, Islamabad 195-1st Floor, Deans Trade Center, Peshawar Cantt; Peshawar Landline: +92.51.282.0449, +92.91.525.3347 E-mail: [email protected], Website: www.alhasan.com ALHASAN SYSTEMS PRIVATE LIMITED A Hi-Tech Knowledge Management, Business Psychology Modeling, and Publishing Company 205-C, 2nd Floor, Evacuee Trust Complex, Sector F-5/1, Islamabad, Pakistan 44000 195-1st Floor, Dean Trade Center, Peshawar Can ; Peshawar, Pakistan 25000 Landline: +92.51.282.0449, +92.91.525.3347 Fax: +92.51.835.9287 Email: [email protected] Website: www.alhasan.com Facebook: www.facebook.com/alhasan.com Twi er: @alhasansystems w3w address: *Alhasan COPYRIGHT © 2015 BY ALHASAN SYSTEMS All rights reserved. No part of this publica on may be reproduced, stored in a retrieval system, or transmi ed, in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the prior wri en permission of ALHASAN SYSTEMS. 58 p.; 8.5x11.5 = A3 Size Map ISBN (P) 978-969-638-093-1 ISBN (D) 978-969-638-094-8 CATALOGING REFERENCE: Disaster Risk Reduc on – Disaster Risk Management – Disaster Risk Assessment Hyogo Framework for Ac on 2005-2015 Building the Resilience of Na ons and Communi es to Disasters IDENTIFY, ACCESS, AND MONITOR DISASTER RISKS AND ENHANCE EARLY WARNING x Risk assessments -

Ehsaas Emergency Cash Payments
Consolidated List of Campsites and Bank Branches for Ehsaas Emergency Cash Payments Campsites Ehsaas Emergency Cash List of campsites for biometrically enabled payments in all 4 provinces including GB, AJK and Islamabad AZAD JAMMU & KASHMIR SR# District Name Tehsil Campsite 1 Bagh Bagh Boys High School Bagh 2 Bagh Bagh Boys High School Bagh 3 Bagh Bagh Boys inter college Rera Dhulli Bagh 4 Bagh Harighal BISP Tehsil Office Harigal 5 Bagh Dhirkot Boys Degree College Dhirkot 6 Bagh Dhirkot Boys Degree College Dhirkot 7 Hattain Hattian Girls Degree Collage Hattain 8 Hattain Hattian Boys High School Chakothi 9 Hattain Chakar Boys Middle School Chakar 10 Hattain Leepa Girls Degree Collage Leepa (Nakot) 11 Haveli Kahuta Boys Degree Collage Kahutta 12 Haveli Kahuta Boys Degree Collage Kahutta 13 Haveli Khurshidabad Boys Inter Collage Khurshidabad 14 Kotli Kotli Govt. Boys Post Graduate College Kotli 15 Kotli Kotli Inter Science College Gulhar 16 Kotli Kotli Govt. Girls High School No. 02 Kotli 17 Kotli Kotli Boys Pilot High School Kotli 18 Kotli Kotli Govt. Boys Middle School Tatta Pani 19 Kotli Sehnsa Govt. Girls High School Sehnsa 20 Kotli Sehnsa Govt. Boys High School Sehnsa 21 Kotli Fatehpur Thakyala Govt. Boys Degree College Fatehpur Thakyala 22 Kotli Fatehpur Thakyala Local Govt. Office 23 Kotli Charhoi Govt. Boys High School Charhoi 24 Kotli Charhoi Govt. Boys Middle School Gulpur 25 Kotli Charhoi Govt. Boys Higher Secondary School Rajdhani 26 Kotli Charhoi Govt. Boys High School Naar 27 Kotli Khuiratta Govt. Boys High School Khuiratta 28 Kotli Khuiratta Govt. Girls High School Khuiratta 29 Bhimber Bhimber Govt. -

Population Census of Pakistan 1961
( ·~ " POPULATION CENSUS OF PAKISTAN 1961 ~ DISTRICT CENSUS REPORT -RAWALPINDI PART-V rV lllAGE STATISJ.ics· 'COMPIL~D BY i<i-iA ·~ BASHIR AHMED KAAN 'ASSJSTANT DIRECTOR OF cENSUS Ri\WALPINoi ~ lt ~':"",.a;ll!;. mn=-rr:n INTRODUCTION The village is the ba sic unit of revenue The Village Statistics contained in this administration and the need for basic statis part have been compiled from Block-wise tics for villages is quite obvious as au plan fi gures contained in the Summaries prepared ning depends on such statistics. They are a lso by the Census Supervisors and Charge indispensable fo r carrying out sample surveys Superintendents. Except for data on houses over limited areas and form the basis of contin and houseJ10lds they are based on the results uous collection ofs tatistics on different aspects of the "Circle Sort"' which was carried out in of rural life and economy. The village was ta ken the Hand Sorting Centres after the physical as the basic unit of enumeration if its popula counting of the individual enumeration tion was 600 or it was a continuous collection schedules. The literacy figures, however, have of about 150 houses on an average. Where been lifted from the Summaries prepared by the village approximated to this size, it was the Supervisors and Charge Superintendents. constituted into a Block. A large nu mber of villages ha d to be split up into a number of The plan of presentati on is that for each Blocks, but the boundaries of Census Block village, the Hadbast number, its name in did not go beyond the limits of a revenue English and Urdu a nd a rea in acres, the estate. -

Village List of Gujranwala , Pakistan
Census 51·No. 30B (I) M.lnt.6-18 300 CENSUS OF PAKISTAN, 1951 VILLAGE LIST I PUNJAB Lahore Divisiona .,.(...t..G.ElCY- OF THE PROVINCIAL TEN DENT CENSUS, JUr.8 1952 ,NO BAHAY'(ALPUR Prleo Ps. 6·8-0 FOREWORD This Village List has been pr,epared from the material collected in con" nection with the Census of Pakistan, 1951. The object of the List is to present useful information about our villages. It was considered that in a predominantly rural country like Pakistan, reliable village statistics should be avaflable and it is hoped that the Village List will form the basis for the continued collection of such statistics. A summary table of the totals for each tehsil showing its area to the nearest square mile. and Its population and the number of houses to the nearest hundred is given on page I together with the page number on which each tehsil begins. The general village table, which has been compiled district-wise and arranged tehsil-wise, appears on page 3 et seq. Within each tehsil the Revenue Kanungo holqos are shown according to their order in the census records. The Village in which the Revenue Kanungo usually resides is printed in bold type at the beginning of each Kanungo holqa and the remaining Villages comprising the ha/qas, are shown thereunder in the order of their revenue hadbast numbers, which are given in column o. Rokhs (tree plantations) and other similar areas even where they are allotted separate revenue hadbast numbers have not been shown as they were not reported in the Charge and Household summaries. -

Appendix - II Pakistani Banks and Their Branches (December 31, 2008)
Appendix - II Pakistani Banks and their Branches (December 31, 2008) Allied Bank Ltd. Bhalwal (2) Chishtian (2) -Grain Market -Grain Market (743) -Noor Hayat Colony -Mohar Sharif Road Abbaspur 251 RB Bandla Bheli Bhattar (A.K.) Chitral Chungpur (A.K.) Abbottabad (4) Burewala (2) Dadu -Bara Towers, Jinnahabad -Grain Market -Pineview Road -Housing Scheme Dadyal (A.K) (2) -Supply Bazar -College Road -The Mall Chak Jhumra -Samahni Ratta Cross Chak Naurang Adda Johal Chak No. 111 P Daharki Adda Nandipur Rasoolpur Chak No. 122/JB Nurpur Danna (A.K.) Bhal Chak No. 142/P Bangla Danyor Adda Pansra Manthar Darband Adda Sarai Mochiwal Chak No. 220 RB Dargai Adda Thikriwala Chak No. 272 HR Fortabbas Darhal Gaggan Ahmed Pur East Chak No. 280/JB (Dawakhri) Daroo Jabagai Kombar Akalgarh (A.K) Chak No. 34/TDA Daska Arifwala Chak No. 354 Daurandi (A.K.) Attock (Campbellpur) Chak No. 44/N.B. Deenpur Bagh (A.K) Chak No. 509 GB Deh Uddhi Bahawalnagar Chak No. 76 RB Dinga Chak No. 80 SB Bahawalpur (5) Chak No. 88/10 R Dera Ghazi Khan (2) Chak No. 89/6-R -Com. Area Sattelite Town -Azmat Road -Dubai Chowk -Model Town -Farid Gate Chakwal (2) -Ghalla Mandi -Mohra Chinna Dera Ismail Khan (3) -Settelite Town -Talagang Road -Circular Road -Commissionery Bazar Bakhar Jamali Mori Talu Chaman -Faqirani Gate (Muryali) Balagarhi Chaprar Balakot Charsadda Dhamke (Faisalabad) Baldher Chaskswari (A.K) Dhamke (Sheikhupura) Bucheke Chattar (A.K) Dhangar Bala (A.K) Chhatro (A.K.) Dheed Wal Bannu (2) Dina -Chai Bazar (Ghalla Mandi) Chichawatni (2) Dipalpur -Preedy Gate -College Road Dir Barja Jandala (A.K) -Railway Road Dunyapur Batkhela Ellahabad Behari Agla Mohra (A.K.) Chilas Eminabad More Bewal Bhagowal Faisalabad (20) Bhakkar Chiniot (2) -Akbarabad Bhaleki (Phularwan Chowk) -Muslim Bazar (Main) -Sargodha Road -Chibban Road 415 ABL -Factory Area -Zia Plaza Gt Road Islamabad (23) -Ghulam Muhammad Abad Colony Gujrat (3) -I-9 Industrial Area -Gole Cloth Market -Grand Trunk Road -Aabpara -Gole Kiryana Bazar -Rehman Saheed Road -Blue Area ABL -Gulburg Colony -Shah Daula Road. -

Rawalpindi 1 Rawalpindi Leprosy Hospital, Zafar-Ul-Haq Road P.O Box No
Valid X-ray License Holder Sr. Facility Rawalpindi 1 Rawalpindi Leprosy Hospital, Zafar-ul-Haq Road P.O Box No. 135, Rawalpindi 2 Al-Shifa Eye Hospital, Jehlum Road, Rawalpindi 3 Health Ways Medical Centre, 8-111, Murree Road Opp. Ministry of Defence Secretrait, Saddar, Rawalpindi 4 Habib Hospital, Saidpur Road, Banni, Rawalpindi 5 Armed Forces Institute of Cadialogy(AFIC), The Mall Road, Rawalpindi 6 Christian Hospital, Faisal Shahid Road, Taxila, Rawalpindi 7 Islamic International Medical Complex Trust, Railway Hospital, Westridge, Rawalpindi 8 Abrar Surgery (Pvt.) Ltd, 219-B(1), Peshawar Road, Rawalpindi 9 Abrar Diagnostic Centre, 312-E, Chairing Cross Peshawar Road, Rawalpindi 10 WAPDA Hospital, Marrier Hassan, Rawalpindi 11 Combined Military Hospital, Murree, Rawalpindi 12 Attock Hospital(Pvt.) Ltd., P. O. Refinary Morgah, Rawalpindi 13 Kahuta Research Laboratories (KRL) Hospital, P. O. Sumbulgah, Tehsil Kahuta, Rawalpindi 14 KRL Medical Center, Dr. A. Q. Khan Road, P. O. Box 502, Rawalpindi 15 Urgent Medical Centre, Medical Tower, 101-A 6th Road, Satellite Town, Rawalpindi 16 Adil Diagnostics, B-1315, Saidpur Road, Rawalpindi 17 Valley Clinic (Pvt.) Ltd., 213, Peshawar Road, Lane 4, Rawalpindi 18 Maryam Memorial Hospital, Peshawar Road, Rawalpindi 19 Dr. Aslam Uppal Hospital & Labs, 3-Quaid Avenue Near Aslam Uppal Square, Lalazar, Wah Cantt., Rawalpindi 20 C/o Dr. Amenah Dental Clinic, 167/3A, Adamjee Road, Rawalpindi, Rawalpindi 21 Margalla Hospital, Pirwadahi Road, Pirwadahi, Rawalpindi 22 Al-Noor Dental Clinic, Mushtaq Plaza Holy Family Chowk Saidpur Raod, Rawalpindi 23 Hearts International Hospital, 192-A, The Mall, Rawalpindi 24 Al-Mustafa Trust Medical Center, Street No. 14, Mini Market Chaklala Scheme-III, Rawalpindi 25 Aman Hospital, 519/8-A, Misrial Road, Rawalpindi 26 DHQ Hospital, Raja Bazar, Rawalpindi 27 HIT Hospital, Taxila Cantt., Taxila, Rawalpindi 28 Syed Mohd Hussain Govt.