Coding and Documentation for Minor Procedures My Background
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Recognizing When a Child's Injury Or Illness Is Caused by Abuse
U.S. Department of Justice Office of Justice Programs Office of Juvenile Justice and Delinquency Prevention Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE U.S. Department of Justice Office of Justice Programs 810 Seventh Street NW. Washington, DC 20531 Eric H. Holder, Jr. Attorney General Karol V. Mason Assistant Attorney General Robert L. Listenbee Administrator Office of Juvenile Justice and Delinquency Prevention Office of Justice Programs Innovation • Partnerships • Safer Neighborhoods www.ojp.usdoj.gov Office of Juvenile Justice and Delinquency Prevention www.ojjdp.gov The Office of Juvenile Justice and Delinquency Prevention is a component of the Office of Justice Programs, which also includes the Bureau of Justice Assistance; the Bureau of Justice Statistics; the National Institute of Justice; the Office for Victims of Crime; and the Office of Sex Offender Sentencing, Monitoring, Apprehending, Registering, and Tracking. Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE NCJ 243908 JULY 2014 Contents Could This Be Child Abuse? ..............................................................................................1 Caretaker Assessment ......................................................................................................2 Injury Assessment ............................................................................................................4 Ruling Out a Natural Phenomenon or Medical Conditions -

Nasolabial and Forehead Flap Reconstruction of Contiguous Alar
Journal of Plastic, Reconstructive & Aesthetic Surgery (2017) 70, 330e335 Nasolabial and forehead flap reconstruction of contiguous alareupper lip defects Jonathan A. Zelken a,b, Sashank K. Reddy c, Chun-Shin Chang a, Shiow-Shuh Chuang a, Cheng-Jen Chang a, Hung-Chang Chen a, Yen-Chang Hsiao a,* a Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital, College of Medicine, Chang Gung University, Taipei, Taiwan b Department of Plastic and Reconstructive Surgery, Breastlink Medical Group, Laguna Hills, CA, USA c Department of Plastic and Reconstructive Surgery, Johns Hopkins Hospital, Baltimore, MD, USA Received 4 May 2016; accepted 31 October 2016 KEYWORDS Summary Background: Defects of the nasal ala and upper lip aesthetic subunits can be Nasal reconstruction; challenging to reconstruct when they occur in isolation. When defects incorporate both Nasolabial flap; the subunits, the challenge is compounded as subunit boundaries also require reconstruc- Rhinoplasty; tion, and local soft tissue reservoirs alone may provide inadequate coverage. In such cases, Forehead flap we used nasolabial flaps for upper lip reconstructionandaforeheadflapforalarrecon- struction. Methods: Three men and three women aged 21e79 years (average, 55 years) were treated for defects of the nasal ala and upper lip that resulted from cancer (n Z 4) and trauma (n Z 2). Unaffected contralateral subunits dictated the flap design. The upper lip subunit was excised and replaced with a nasolabial flap. The flap, depending on the contralateral reference, determined accurate alar base position. A forehead flap resurfaced or replaced the nasal ala. Autologous cartilage was used in every case to fortify the forehead flap reconstruction. Results: Patients were followed for 25.6 months (range, 1e4 years). -
Instruction Manual for Citizen Digital Forehead And
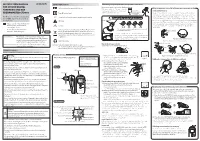
INSTRUCTION MANUAL Symbol Explanations Measuring body temperature (temperature detection) Remove the probe cap and check the probe tip. FOR CITIZEN DIGITAL Refer to instruction manual before use. How to measure correctly in the ear measurement mode * When using it for the first time, open the FOREHEAD AND EAR battery cap and remove the insulation Open the Temperature basics battery cap to THERMOMETER CTD710 Type BF applied part sheet under the battery cap. remove the All objects radiate heat. This device consists of a probe with a built-in insulation sheet. infrared sensor that measures body temperature by detecting the heat Thank you very much for purchasing IP22 Classification for water ingress and particulate matter. radiated by the eardrum and surrounding tissue. Figure 4 shows the the CITIZEN digital forehead and ear Keeping the probe window clean tortuous anatomy of a normal ear canal. As shown in Figure 5, hold the thermometer. Warning Probe window ear and gently pull it back at an angle or pull it straight back to straighten out the ear canal. The shape of the ear canal differs from individual, check • Please read all of the information in before measurement. Accurate temperature measurements make it this instruction manual before Caution essential to straighten the ear canal so that the probe tip directly faces operating the device. the eardrum. • Be sure to have this instruction Indicates this device is subject to the Waste Electrical and Dirt in the probe window will impact the accuracy of temperature detection. External auditory manual to hand during use. 1902LA Electronic Equipment Directive in the European Union. -

Ear and Forehead Thermometer
Ear and Forehead Thermometer INSTRUCTION MANUAL Item No. 91807 19.PJN174-14_GA-USA_HHD-Ohrthermometer_DSO364_28.07.14 Montag, 28. Juli 2014 14:37:38 USAD TABLE OF CONTENTS No. Topic Page 1.0 Definition of symbols 5 2.0 Application and functionality 6 2.1 Intended use 6 2.2 Field of application 7 3.0 Safety instructions 7 3.1 General safety instructions 7 3.3 Environment for which the DSO 364 device is not suited 9 3.4 Usage by children and adolescents 10 3.5 Information on the application of the device 10 4.0 Questions concerning body temperature 13 4.1 What is body temperature? 13 4.2 Advantages of measuring the body tempera- ture in the ear 14 4.3 Information on measuring the body tempera- ture in the ear 15 5.0 Scope of delivery / contents 16 6.0 Designation of device parts 17 7.0 LCD display 18 8.0 Basic functions 19 8.1 Commissioning of the device 19 8.2 Warning indicator if the body temperature is 21 too high 2 19.PJN174-14_GA-USA_HHD-Ohrthermometer_DSO364_28.07.14 Montag, 28. Juli 2014 14:37:38 TABLE OF CONTENTS USA No. Topic Page 8.3 Backlighting / torch function 21 8.4 Energy saving mode 22 8.5 Setting °Celsius / °Fahrenheit 22 9.0 Display / setting time and date 23 9.1 Display of time and date 23 9.2 Setting time and date 23 10.0 Memory mode 26 11.0 Measuring the temperature in the ear 28 12.0 Measuring the temperature on the forehead 30 13.0 Object temperature measurement 32 14.0 Disposal of the device 33 15.0 Battery change and information concerning batteries 33 16.0 Cleaning and care 36 17.0 “Cleaning” warning indicator 37 18.0 Calibration 38 19.0 Malfunctions 39 20.0 Technical specification 41 21.0 Warranty 44 3 19.PJN174-14_GA-USA_HHD-Ohrthermometer_DSO364_28.07.14 Montag, 28. -

Core Strength Exercises
CORE STRENGTH EXERCISES • The main muscles involved with Core Strength include muscles of the abdomen, hip flexors and low back postural muscles. • It is important to maintain proper strength of these muscles to prevent and rehabilitate from low back / pelvic dysfunction and pain. • All of these exercises should be comfortable and not produce pain or discomfort. Bracing: The Key to preventing low back injuries Abdominal Bracing – Lying down • Lie down, face up with your knees bent and feet on floor. • Contract your stomach muscles so that you imagine pushing your low back to the floor or that you are pulling your belly button to your spine. Abdominal Bracing - Standing • Stand up straight and place one hand on the small of the back and one hand on your abdomen. • Bend Forward at the waist and feel the lower back muscles contract (extensors). • Come back up to neutral to relax the low back muscles. • You will feel the low back muscles contract when you contract your abdominal and gluteal muscles. Bracing technique and curling • Lay on the ground on your back. • One leg is bent and the other leg remains flat on the floor. Your hands can be on your chest or at your side. • Fix your eyes on a spot on the ceiling directly above you. • Tighten your stomach muscles. • Holding the stomach contraction, lift your shoulder blades and head off the floor while looking at that spot on the ceiling. Hold for 3-10 seconds and repeat three times. • Switch leg positions and repeat the technique. Beginner to Intermediate position • Position yourself on your hands and knees with your pelvis and thighs at 90 degrees and upper back and arms at 90 degrees. -

Preoperative Skin Antisepsis with Chlorhexidine Gluconate Versus Povidone-Iodine: a Prospective Analysis of 6959 Consecutive Spinal Surgery Patients
CLINICAL ARTICLE J Neurosurg Spine 28:209–214, 2018 Preoperative skin antisepsis with chlorhexidine gluconate versus povidone-iodine: a prospective analysis of 6959 consecutive spinal surgery patients George M. Ghobrial, MD, Michael Y. Wang, MD, Barth A. Green, MD, Howard B. Levene, MD, PhD, Glen Manzano, MD, Steven Vanni, DO, DC, Robert M. Starke, MD, MSc, George Jimsheleishvili, MD, Kenneth M. Crandall, MD, Marina Dididze, MD, PhD, and Allan D. Levi, MD, PhD Department of Neurological Surgery and The Miami Project to Cure Paralysis, University of Miami Miller School of Medicine, Miami, Florida OBJECTIVE The aim of this study was to determine the efficacy of 2 common preoperative surgical skin antiseptic agents, ChloraPrep and Betadine, in the reduction of postoperative surgical site infection (SSI) in spinal surgery proce- dures. METHODS Two preoperative surgical skin antiseptic agents—ChloraPrep (2% chlorhexidine gluconate and 70% iso- propyl alcohol) and Betadine (7.5% povidone-iodine solution)—were prospectively compared across 2 consecutive time periods for all consecutive adult neurosurgical spine patients. The primary end point was the incidence of SSI. RESULTS A total of 6959 consecutive spinal surgery patients were identified from July 1, 2011, through August 31, 2015, with 4495 (64.6%) and 2464 (35.4%) patients treated at facilities 1 and 2, respectively. Sixty-nine (0.992%) SSIs were observed. There was no significant difference in the incidence of infection between patients prepared with Beta- dine (33 [1.036%] of 3185) and those prepared with ChloraPrep (36 [0.954%] of 3774; p = 0.728). Neither was there a significant difference in the incidence of infection in the patients treated at facility 1 (52 [1.157%] of 4495) versus facility 2 (17 [0.690%] of 2464; p = 0.06). -

Vivid Dreams/ Problems Sleeping: Nausea/Upset Stomach: Itching/Rash
Addressing NRT Barriers • Assess the severity of symptoms (Is it tolerable?). • Assess Hx: onset, duration and any troubleshooting that has already taken place. If indicated, get history of these symptoms when not taking these medications. You may also ask how Pt. would normally treat these symptoms. • If symptoms are tolerable àdevelop troubleshooting plan with Pt. Inform Pt. that many symptoms will go away after a few days. Reassess at next visit, but ask Pt. to call if symptoms persist/worsen or become intolerable before next call/visit. • If symptoms are not tolerableàconsider changing products or dosages as applicable. Consult study physician, as needed. Refer Pt. to their personal physician, if needed (e.g., prescription strength creams). • All potential cardiac symptoms should be promptly reported to study physician. Advise Pt. to discontinue NRT when indicated or instructed by study physician. Vivid Dreams/ Problems Sleeping: - Assess if sleep is being disrupted. Is night waking normal for Pt. – what is Pts.’ normal routine? - May try taking patch off at night, keeping in mind cravings may be stronger in the AM. After a couple of nights, try again to wear patch overnight. If using more than 1 patch, may consider only wearing 1 at night. - May try removing patch at night and putting on 2 hours before waking, especially when early morning waking is part of routine. Otherwise, can set an alarm, put on patch, and go back to sleep. - Regulate eating and sleeping patterns and use sleep hygiene tips (relaxation training, avoid caffeine). - Do not smoke or use short-acting NRT within 1-2 hours of bedtime (especially if sleep initiation is the major complaint.) Nausea/upset stomach: - Ask if nausea is only after using gum/lozenge or also after smoking a cigarette. -
Facial Image Comparison Feature List for Morphological Analysis
Disclaimer: As a condition to the use of this document and the information contained herein, the Facial Identification Scientific Working Group (FISWG) requests notification by e-mail before or contemporaneously to the introduction of this document, or any portion thereof, as a marked exhibit offered for or moved into evidence in any judicial, administrative, legislative, or adjudicatory hearing or other proceeding (including discovery proceedings) in the United States or any foreign country. Such notification shall include: 1) the formal name of the proceeding, including docket number or similar identifier; 2) the name and location of the body conducting the hearing or proceeding; and 3) the name, mailing address (if available) and contact information of the party offering or moving the document into evidence. Subsequent to the use of this document in a formal proceeding, it is requested that FISWG be notified as to its use and the outcome of the proceeding. Notifications should be sent to: Redistribution Policy: FISWG grants permission for redistribution and use of all publicly posted documents created by FISWG, provided the following conditions are met: Redistributions of documents, or parts of documents, must retain the FISWG cover page containing the disclaimer. Neither the name of FISWG, nor the names of its contributors, may be used to endorse or promote products derived from its documents. Any reference or quote from a FISWG document must include the version number (or creation date) of the document and mention if the document is in a draft status. Version 2.0 2018.09.11 Facial Image Comparison Feature List for Morphological Analysis 1. -

Incision & Drainage Informed Consent
Jeri Shuster, M.D., P.A. and Women’s Center, Inc. JERI SHUSTER, M.D., PA & WOMEN’SJeri Shuster, CENTER, INC M.D.,. P.A. Jeri Shuster, M.D., Fellowand of the Women’s American CollegeCenter, Obstetricians Inc. and Gynecologists Kathryn Cervi, C.R.N.P., Women’s Health Care Nurse Practitioner Jeri Shuster, M.D., Fellow of the American College Obstetricians and Gynecologists INFORMED CONSENT: Kathryn INCISION Cervi, C.R.N.P., AND Women’s DRAINAGE Health (I Care & D) Nurse Practitioner I hereby request and authorize Dr. to Jeri Shuster perform upon me the procedure: incision and drainage of _________________________________________________________________________ _____________________________________________________________________________________________ This procedure involves making an incision, either with a scalpel or with an electrical device, in order to enable fluid to drain from an area of the body. The procedure is intended to drain a cyst(s), abscess(es), or infected tissue. Risks include: bleeding, infection, burn injury, pain, scarring, failure to diagnose or cure the underlying condition, persistence or recurrence of the condition. To reduce risk of infection, after the procedure keep area as clean and dry as possible. Wash three times each day with lukewarm water and mild soap. Dry by gently dabbing with a soft wel to or carefully use a blow dryer on the cool setting. Follow each wash/dry with antibacterial ointment (such as Neosporin or Bacitracin). If genital incision and drainage ou is performed, y may also place antibiotic ointment onto cotton balls (not cosmetic puffs) to cover the wounds during urination or bowel movements. Benefits may include achieving a diagnosis (by distinguishing between a cyst and an abscss) and alleviating symptoms such as pain. -

The Complexity and Origins of the Human Eye: a Brief Study on the Anatomy, Physiology, and Origin of the Eye
Running Head: THE COMPLEX HUMAN EYE 1 The Complexity and Origins of the Human Eye: A Brief Study on the Anatomy, Physiology, and Origin of the Eye Evan Sebastian A Senior Thesis submitted in partial fulfillment of the requirements for graduation in the Honors Program Liberty University Spring 2010 THE COMPLEX HUMAN EYE 2 Acceptance of Senior Honors Thesis This Senior Honors Thesis is accepted in partial fulfillment of the requirements for graduation from the Honors Program of Liberty University. ______________________________ David A. Titcomb, PT, DPT Thesis Chair ______________________________ David DeWitt, Ph.D. Committee Member ______________________________ Garth McGibbon, M.S. Committee Member ______________________________ Marilyn Gadomski, Ph.D. Assistant Honors Director ______________________________ Date THE COMPLEX HUMAN EYE 3 Abstract The human eye has been the cause of much controversy in regards to its complexity and how the human eye came to be. Through following and discussing the anatomical and physiological functions of the eye, a better understanding of the argument of origins can be seen. The anatomy of the human eye and its many functions are clearly seen, through its complexity. When observing the intricacy of vision and all of the different aspects and connections, it does seem that the human eye is a miracle, no matter its origins. Major biological functions and processes occurring in the retina show the intensity of the eye’s intricacy. After viewing the eye and reviewing its anatomical and physiological domain, arguments regarding its origins are more clearly seen and understood. Evolutionary theory, in terms of Darwin’s thoughts, theorized fossilization of animals, computer simulations of eye evolution, and new research on supposed prior genes occurring in lower life forms leading to human life. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Clinical Practice Guideline for the Management of Anorectal Abscess, Fistula-In-Ano, and Rectovaginal Fistula Jon D
PRACTICE GUIDELINES Clinical Practice Guideline for the Management of Anorectal Abscess, Fistula-in-Ano, and Rectovaginal Fistula Jon D. Vogel, M.D. • Eric K. Johnson, M.D. • Arden M. Morris, M.D. • Ian M. Paquette, M.D. Theodore J. Saclarides, M.D. • Daniel L. Feingold, M.D. • Scott R. Steele, M.D. Prepared on behalf of The Clinical Practice Guidelines Committee of the American Society of Colon and Rectal Surgeons he American Society of Colon and Rectal Sur- and submucosal locations.7–11 Anorectal abscess occurs geons is dedicated to ensuring high-quality pa- more often in males than females, and may occur at any Ttient care by advancing the science, prevention, age, with peak incidence among 20 to 40 year olds.4,8–12 and management of disorders and diseases of the co- In general, the abscess is treated with prompt incision lon, rectum, and anus. The Clinical Practice Guide- and drainage.4,6,10,13 lines Committee is charged with leading international Fistula-in-ano is a tract that connects the perine- efforts in defining quality care for conditions related al skin to the anal canal. In patients with an anorec- to the colon, rectum, and anus by developing clinical tal abscess, 30% to 70% present with a concomitant practice guidelines based on the best available evidence. fistula-in-ano, and, in those who do not, one-third will These guidelines are inclusive, not prescriptive, and are be diagnosed with a fistula in the months to years after intended for the use of all practitioners, health care abscess drainage.2,5,8–10,13–16 Although a perianal abscess workers, and patients who desire information about the is defined by the anatomic space in which it forms, a management of the conditions addressed by the topics fistula-in-ano is classified in terms of its relationship to covered in these guidelines.