FY 2015 Nigeria Country Operational Plan (COP)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Biodiversity Conservation Friendliness Status of Rural Farmers in Abak Agricultural Zone of Akwa Ibom State
International Journal of Environment and Climate Change 10(9): 179-189, 2020; Article no.IJECC.59232 ISSN: 2581-8627 (Past name: British Journal of Environment & Climate Change, Past ISSN: 2231–4784) Biodiversity Conservation Friendliness Status of Rural Farmers in Abak Agricultural Zone of Akwa Ibom State J. T. Ekanem1*, N. U. Okorie1 and J. Ibanga1 1Department of Agricultural Economics and Extension, Akwa Ibom State University, Obio Akpa, Campus, P.M.B. 1167, Uyo, Akwa Ibom State, Nigeria. Authors’ contributions This work was carried out in collaboration among all authors. Author JTE designed the study, performed the statistical analysis and wrote the protocol. Author JI wrote the first draft of the manuscript. Authors JTE and JI managed the analyses of the study. Author NUO managed the literature searches. All authors read and approved the final manuscript. Article Information DOI: 10.9734/IJECC/2020/v10i930239 Editor(s): (1) Dr. Anthony R. Lupo, University of Missouri, USA. (2) Dr. Hani Rezgallah Al-Hamed Al-Amoush, Al al-Bayt University, Jordan. (3) Dr. Wen-Cheng Liu, National United University, Taiwan. Reviewers: (1) Madhulika Sahoo, Vellore Institute of Technology, School of Business, India. (2) Bulbul G. Nagrale, Maharashtra Animal & Fishery Sciences University, India. (3) Aditya Pratap Singh, Bidhan Chandra Krishi Viswavidyalaya (BCKV), India. Complete Peer review History: http://www.sdiarticle4.com/review-history/59232 Received 14 June 2020 Original Research Article Accepted 19 August 2020 Published 28 August 2020 ABSTRACT Consolidating on farmers’ agro-ecological knowledge to design environmental-friendly agricultural systems is crucial given the environmental impact of commercial agriculture. The study aimed at assessing the awareness level of the respondents on biodiversity conservation, their biodiversity conservation information source(s), respondents’ information seeking behaviour and their perception towards biodiversity conservation. -

4 YEARS Plus of GOV UDOM EMMANUEL.Cdr
F AK O WA T N IB E O M M N S R T E A V T O E G 4 YEARS TOUCHING LIVES May 2015 Job Creation 2016 Infrastructural Consolidation & Expansion 2017 Poverty Alleviation 2018 Economic & Political N Inclusion Wealth Creation May 2019 The Five-Point Agenda of Governor Udom Emmanuel AVIATION May 2019 INDUSTRIALIZATION DEVELOPMENT SMALL & RURAL & 2020 MEDIUM SCALE RIVERINE AREA ENTERPRISES DEVELOPMENT The next COMPLETION four 2021 years AGENDA INFRASTRUCTURE AGRICULTURE 2022 May 2023 SECURITY HUMAN CAPACITY DEVELOPMENT 02 www.akwaibomstate.gov.ng TOUCHING LIVES IN MORE WAYS ... n 11,000 hectares of coconut plantation n Over 1700km of roads n 3,240 hectares of cassava plantation in 15 LGAs (FADAMA) n 40 bridges n 49,318 registered rice farmers n Completion of the State Secretariat Annex n 450 youths trained on cocoa maintenance n Construction of 2nd airport runway (taxiway) n Subsidized fertilizers, oil palm & cocoa seedlings n Upgrade of Airport main runway to category 2 n Akwa Prime Hatchery -17,000 day old chicks weekly n Only state to own & maintain an airport independently n Free Improved Corn seedlings n n Flood control at Nsikak Eduok n Vegetable Green Houses Completion of Four Points by Sheraton Hotel n n International Worship Centre (on-going) Avenue, Uyo Roads & Oil Palm Processing Plant n n n Eket International Modern Market 21 Storey Intelligent office Agriculture Cassava Processing Mills n Airport Terminal building (under construction) complex...ongoing n Maize Shelling/Drying Mill Other Infrastructure n n Renovation of 85 Flats at n Rice Processing Mills Expansion of Shopping Mall at Ibom Wellington Bassey Army Barracks, n Over 1,200 hectares of rice cultivated Tropicana Entertainment Centre n Ibagwa n N300,000 grant to 250 beneficiaries under the Graduate Unemployment Completion of Governor’s Lodge, Lagos n Private Hangar for State aircraft Youth Scheme n Setting up of Ibom FADAMA Micro Finance Bank n Free medical services for children below 5 years, n Free & compulsory basic education in public schools pregnant women & the aged. -

World Bank Document
ESMP for Nguzu Edda (Afikpo South LGA Headquarters) Gully Erosion site in Ebonyi State Public Disclosure Authorized ENVIRONMENTAL AND SOCIAL MANAGEMENT PLAN (ESMP) (Final Draft Report) For NGUZU EDDA (AFIKPO SOUTH LOCAL GOVERNMENT HEADQUARTERS) GULLY EROSION INTERVENTION SITE, EBONYI STATE Public Disclosure Authorized UNDER Public Disclosure Authorized THE NIGERIA EROSION & WATERSHED MANAGEMENT PROJECT (NEWMAP) WORLD BANK ASSISTED By EBONYI STATE -NIGERIA EROSION & WATERSHED MANAGEMENT PROJECT (EBS-NEWMAP) ABAKALIKI, EBONYI STATE Public Disclosure Authorized Public Disclosure Authorized June, 2014 ESMP for Nguzu Edda (Afikpo South LGA Headquarters) Gully Erosion site in Ebonyi State ESMP for Nguzu Edda (Afikpo South LGA Headquarters) Gully Erosion site in Ebonyi State Table of Contents Content Page Cover Page i Table of Contents ii List of Tables v List of Figures vi List of Maps vi List of Boxes vi List of Abbreviations/ Acronyms vii Definition of Terms ix Executive Summary x CHAPTER 1: GENERAL INTRODUCTION 1 1.1 Background 2 1.2 The proposed Intervention Work 3 1.3 Need for ESMP for the Proposed Intervention Work 4 1.4 Objectives of this Environmental and Social Management Plan 4 1.5 Scope/Terms of Reference of the ESMP and Tasks 4 1.6 Approaches for Preparing the Environmental and Social Management Plan 4 1.6.1 Literature Review 4 1.6.2 Interactive Discussions/Consultations 4 1.6.3 Field Visits 4 1.6.4 Identification of Potential Impacts and Mitigation Measures 4 CHAPTER 2: INSTITUTIONAL AND LEGAL FRAMEWORK FOR ENVIRONMENTAL MANAGEMENT -

Fine Particulate Distribution and Assessment in Nasarawa State – Nigeria
IOSR Journal of Applied Physics (IOSR-JAP) e-ISSN: 2278-4861.Volume 8, Issue 2 Ver. I (Mar. - Apr. 2016), PP 32-38 www.iosrjournals Fine Particulate Distribution and Assessment in Nasarawa State – Nigeria J.U. Ugwuanyi1, A.A. Tyovenda2, T.J. Ayua3 1,2,3 Department Of Physics, University Of Agriculture Makurdi, Benue State - Nigeria Abstract: The purpose of this work is to analyze fine particulate matter (PM10 ) distribution in the ambient air of some major towns in Nasarawa State-North central Nigeria using a high volume respirable dust sampler (APM 460 NL) model, also the meteorological parameters of the State have been correlated with the measured values. Ambient air laden with suspended particulates enter the APM 460 NL system through the inlet pipe, which separates the air into fine and coarse particles. The PM10 concentrations were analyzed to obtain the monthly average PM10 concentration and monthly maximum concentration. The results show that Nasarawa State towns of Karu and Lafia have fine particulates loading in the ambient air more than the recommended standard set by NAAQS and WHO. Variation trends of pollution levels were also identified. The fine particulate matter PM10 average concentrations in the ambient air of Nasarawa State towns had average values increase in the range of 4.0 – 18.0µg/m3 per month. The level of monthly increase of maximum average concentrations also had readings in the range of 8.0 – 20.0 µg/m3 per month. These values were compared with the NAAQS to obtain the toxicity potential for all the study towns in the State. -

2021-2022 Entrance Examination Result.Xlsx
OSUN STATE COLLEGE OF HEALTH TECHNOLOGY, ILESA. 2021/2022 ENTRANCE EXAMINATION RESULT PROFESSIONAL DIPLOMA IN HEALTH INFORMATION MANAGEMENT S/N Reg Nos Name Sex Age State Local Government Courses Total 1 APP3819 OGUNLUMADE TOMILOLA DEBORAH Female 19 Osun Atakunmosa West Professional Diploma in Health Information Mgt.70 2 APP1585 TAIWO GRACE DEBORAH Female 16 Osun Iwo Professional Diploma in Health Information Mgt.70 3 APP0492 ALADOKUN ABOSEDE MARY Female 25 Osun Ifelodun Professional Diploma in Health Information Mgt.67 4 APP3123 AKINYODE OLUWATIMIL?YIN JANET Female 20 Osun Iwo Professional Diploma in Health Information Mgt.65 5 APP3459 MOHAMMED SHIFAU OLAYINKA Female 22 Osun Osogbo Professional Diploma in Health Information Mgt.65 6 APP3736 OLOWOOKERE FERANMI FAITH Female 18 Osun Atakunmosa West Professional Diploma in Health Information Mgt.65 7 APP3621 ADEBUSOYE OMOLARA MAR Y Female 21 Ondo Others Professional Diploma in Health Information Mgt.64 8 APP1319 OLUWOLE CECILIA OPEYEMI Female 21 Osun Odo Otin Professional Diploma in Health Information Mgt.63 9 APP1165 ADEWUYI ESTHER JESUPEMI Female 19 Osun Ilesa West Professional Diploma in Health Information Mgt.62 10 APP2482 AFOLABI ABISOLA RUKAYAT Female 19 Osun Ede South Professional Diploma in Health Information Mgt.62 11 APP3082 AREGBESOLA MOTUNRAYO SOBURAH Female 19 Ondo Others Professional Diploma in Health Information Mgt.62 12 APP1270 OKUNLOLA BLESSING GRACE Female 20 Osun Boripe Professional Diploma in Health Information Mgt.62 13 APP2527 MAKINDE TITILAYO MARY Female 25 Osun Ilesa -

Nigeria's Constitution of 1999
PDF generated: 26 Aug 2021, 16:42 constituteproject.org Nigeria's Constitution of 1999 This complete constitution has been generated from excerpts of texts from the repository of the Comparative Constitutions Project, and distributed on constituteproject.org. constituteproject.org PDF generated: 26 Aug 2021, 16:42 Table of contents Preamble . 5 Chapter I: General Provisions . 5 Part I: Federal Republic of Nigeria . 5 Part II: Powers of the Federal Republic of Nigeria . 6 Chapter II: Fundamental Objectives and Directive Principles of State Policy . 13 Chapter III: Citizenship . 17 Chapter IV: Fundamental Rights . 20 Chapter V: The Legislature . 28 Part I: National Assembly . 28 A. Composition and Staff of National Assembly . 28 B. Procedure for Summoning and Dissolution of National Assembly . 29 C. Qualifications for Membership of National Assembly and Right of Attendance . 32 D. Elections to National Assembly . 35 E. Powers and Control over Public Funds . 36 Part II: House of Assembly of a State . 40 A. Composition and Staff of House of Assembly . 40 B. Procedure for Summoning and Dissolution of House of Assembly . 41 C. Qualification for Membership of House of Assembly and Right of Attendance . 43 D. Elections to a House of Assembly . 45 E. Powers and Control over Public Funds . 47 Chapter VI: The Executive . 50 Part I: Federal Executive . 50 A. The President of the Federation . 50 B. Establishment of Certain Federal Executive Bodies . 58 C. Public Revenue . 61 D. The Public Service of the Federation . 63 Part II: State Executive . 65 A. Governor of a State . 65 B. Establishment of Certain State Executive Bodies . -

Prof. Dr. Kayode AJAYI Dr. Muyiwa ADEYEMI Faculty of Education Olabisi Onabanjo University, Ago-Iwoye, NIGERIA
International Journal on New Trends in Education and Their Implications April, May, June 2011 Volume: 2 Issue: 2 Article: 4 ISSN 1309-6249 UNIVERSAL BASIC EDUCATION (UBE) POLICY IMPLEMENTATION IN FACILITIES PROVISION: Ogun State as a Case Study Prof. Dr. Kayode AJAYI Dr. Muyiwa ADEYEMI Faculty of Education Olabisi Onabanjo University, Ago-Iwoye, NIGERIA ABSTRACT The Universal Basic Education Programme (UBE) which encompasses primary and junior secondary education for all children (covering the first nine years of schooling), nomadic education and literacy and non-formal education in Nigeria have adopted the “collaborative/partnership approach”. In Ogun State, the UBE Act was passed into law in 2005 after that of the Federal government in 2004, hence, the demonstration of the intention to make the UBE free, compulsory and universal. The aspects of the policy which is capital intensive require the government to provide adequately for basic education in the area of organization, funding, staff development, facilities, among others. With the commencement of the scheme in 1999/2000 until-date, Ogun State, especially in the area of facility provision, has joined in the collaborative effort with the Federal government through counter-part funding to provide some facilities to schools in the State, especially at the Primary level. These facilities include textbooks (in core subjects’ areas- Mathematics, English, Social Studies and Primary Science), blocks of classrooms, furniture, laboratories/library, teachers, etc. This study attempts to assess the level of articulation by the Ogun State Government of its UBE policy within the general framework of the scheme in providing facilities to schools at the primary level. -

Enugu State, Nigeria Out-Of-School Children Survey Report
ENUGU STATE, NIGERIA OUT-OF-SCHOOLCHILDREN SURVEY REPORT October, 2014 PREFACE The challenge of school-aged children who for one reason or another did not enrol in school at all or enrolled and later dropped out for whatever reason has been a perennial challenge to education the world over. Nigeria alone is said to house over 10 million out of school children. This is in spite of the universal basic education programme which has been running in the country since 1999. For Enugu State, it is not clear what the state contributes to that national pool of children who are reported to be out of school. Given the effort of the State Government in implementing the universal basic education programme, it is easy to assume that all children in Enugu State are enrolled and are attending school. This kind of assumption might not give us the benefit of knowing the true state of things as they relate to out-of-school children in our State. This is even more so given the State’s development and approval of the Inclusive Education Policy, which has increased the challenge of ensuring that every child of school age, no matter his or her circumstance of birth or residence, has access to quality education; hence, the need to be concerned even for only one child that is out of school. It is, therefore, in a bid to ascertain the prevalence of the incidence of children who are outside the school system, whether public or private, that the Ministry of Education and Enugu State Universal Basic Education Board collaborated with DFID-ESSPIN and other stakeholders to conduct the out of school children’s survey. -

Growing Insecurity in Rivers: Impacts of Re-Run Elections
THE FUND FOR PEACE PARTNERSHIPS INITATIVE IN THE NIGER DELTA NIGER DELTA PARTNERSHIP INITIATIVE Growing Insecurity in Rivers: Impacts of Re-Run Elections Briefing: May 2016 Elections have been a cyclical driver of House of Assembly and Governorship Rivers State, Nigeria conflict risk and violence in Rivers state elections in Rivers. The Independent since 1999. The state was reported to have National Election Commission (INEC) had the highest number of violent incidents headquarters in the state were reportedly during the 2015 general elections in Nigeria. burnt down during the 11 April 2015 In the lead-up and aftermath of the 2016 gubernatorial and state House of Assembly legislative election rerun on 19 March, elections. Heavy gun shots and fatalities Rivers was once again marred by wide- were reported across the state amidst a spread political and cult violence with massive deployment of public security fatalities in the lead-up surpassing any forces. period since 2009. This ongoing cycle of insecurity is not only impacting the citizens There were allegations of widespread voter of the state, but also business. manipulation, intimidation, violence, and hijacking of voting materials. The outcome According to the National Bureau of of the elections was characterised by Statistics, Rivers has the second largest GDP protests and petitions. Eventually, 22 out of after Lagos, but it is also one of the most the 32 State House of Assembly seats and violent states per capita in the Niger Delta. 12 of the 13 Federal House of Representa- This briefing outlines the growing insecurity With increasing insecurity in the state tives, as well as three Senators elected on in Rivers State, Nigeria in the lead up to the surrounding election cycles in 2015 and the platform of the People’s Democratic latest round of the legislative elections in 2016, there are growing concerns that local Party (PDP), were nullified by the elections March 2016. -

AFRREV STECH, Vol. 3(2) May, 2014
AFRREV STECH, Vol. 3(2) May, 2014 AFRREV STECH An International Journal of Science and Technology Bahir Dar, Ethiopia Vol. 3 (2), S/No 7, May, 2014: 51-65 ISSN 2225-8612 (Print) ISSN 2227-5444 (Online) http://dx.doi.org/10.4314/stech.v3i2.4 THE USE OF COMPOSITE WATER POVERTY INDEX IN ASSESSING WATER SCARCITY IN THE RURAL AREAS OF OYO STATE, NIGERIA IFABIYI, IFATOKUN PAUL Department of Geography and Environmental Management, Faculty of Social Sciences University of Ilorin; Ilorin, Kwara State, Nigeria E-mail: 234 8033231626 & OGUNBODE, TIMOTHY OYEBAMIJI Faculty of Law Bowen University, Iwo Osun State, Nigeria Abstract Physical availability of water resources is beneficial to man when it is readily accessible. Oyo State is noted for abundant surface water and appreciable groundwater resources in its pockets of regolith aquifers; as it has about eight months of rainy season and a relatively deep weathered regolith. In spite of this, cases of water associated diseases Copyright© IAARR 2014: www.afrrevjo.net 51 Indexed and Listed in AJOL, ARRONET AFRREV STECH, Vol. 3(2) May, 2014 and deaths have been reported in the rural areas of the state. This study attempts to conduct an investigation into accessibility to potable water in the rural areas of Oyo State, Nigeria via the component approach of water poverty index (WPI). Multistage method of sampling was applied to select 5 rural communities from 25 rural LGAs out of the 33 LGAs in the State. Data were collected through the administration of 1,250 copies of questionnaire across 125 rural communities. Component Index method as developed by Sullivan, et al (2003) was modified and used in this study. -

Farmers Utilization of Insecticide Treated Bed Nets for Malaria
technol ro og g y A Nlerum, Agrotechnology 2016, 5:2 Agrotechnology DOI: 10.4172/2168-9881.1000150 ISSN: 2168-9881 Research Article Open Access Farmers Utilization of Insecticide Treated Bed Nets for Malaria Prevention in Ahoada East Local Government Area, Rivers State, Nigeria Franklin E Nlerum* Department of Agricultural and Applied Economics/Extension, Rivers State University of Science and Technology, Nkpolu-Oroworukwo, Nigeria Abstract The study examined the utilization of insecticide treated bed nets for malaria prevention by rural farmers in Ahoada East Local Government Area of Rivers State, Nigeria. The sample size of the study was 100 respondents who were randomly selected from farmers in the area who benefited from the free distribution of the nets by Rivers State Government. The questionnaire was used in eliciting data from the respondents. Data were analyzed with percentage, mean score and multiple regression. Socio-economic result shows that the respondents on the average were 40 years old, earned monthly net income of N24,184.00 ($121.38) and spent 11 years in schooling. More results indicated that while the ownership of the net was as high as 71.73%, the actual utilization was as low as 28.27%. Result of multiple regression analysis indicated a multiple determination (R2) value of 0.6333. Determinants of the utilization of the net were age, sex, occupation and educational level of the respondents. The two major constraints in the utilization of the net in the area were inadequate information and poor design and inconvenience of hanging. In order to improve the rate of utilization of the net in the area, the study recommends enhanced information which will lead to a better education of the beneficiaries. -
YELLOW FEVER SITUATION REPORT Serial Number: 001 February 2021 Monthly Sitrep Epi Week: Week 1, 2020 – Week 08, 2021 Reporting Month: February 2021
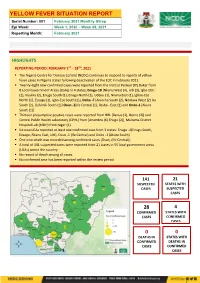
YELLOW FEVER SITUATION REPORT Serial Number: 001 February 2021 Monthly Sitrep Epi Week: Week 1, 2020 – Week 08, 2021 Reporting Month: February 2021 HIGHLIGHTS REPORTING PERIOD: FEBRUARY 1ST – 28TH, 2021 ▪ The Nigeria Centre for Disease Control (NCDC) continues to respond to reports of yellow fever cases in Nigeria states following deactivation of the EOC in February 2021. ▪ Twenty -eight new confirmed cases were reported from the Institut Pasteur (IP) Dakar from 8 Local Government Areas (LGAs) in 4 states; Enugu-18 [Nkanu West (4), Udi (3), Igbo-Etiti (2), Nsukka (2), Enugu South (1), Enugu North (1), Udenu (1), Nkanu East (1), Igboe-Eze North (1), Ezeagu (1), Igbo-Eze South (1)], Delta -7 [Aniocha South (2), Ndokwa West (2) Ika South (2), Oshimili South (1)] Osun -2[Ife Central (1), Ilesha - East (1) and Ondo-1 [Akure South (1)] ▪ Thirteen presumptive positive cases were reported from NRL [Benue (2), Borno (2)] and Central Public Health Laboratory (CPHL) from [Anambra (6) Enugu (2)], Maitama District Hospital Lab (MDH) from Niger (1) ▪ Six new LGAs reported at least one confirmed case from 3 states: Enugu -4(Enugu South, Ezeagu, Nkanu East, Udi), Osun -1 (Ife Central) and Ondo -1 (Akure South) ▪ One new death was recorded among confirmed cases [Osun, (Ife Central)] ▪ A total of 141 suspected cases were reported from 21 states in 55 local government areas (LGAs) across the country ▪ No record of death among all cases. ▪ No confirmed case has been reported within the review period 141 21 SUSPECTED STATES WITH CASES SUSPECTED CASES 28 4