Pathogens and Carcinogenesis: a Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Tasmanian Devils' Transmissible Cancer
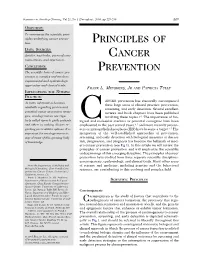
Tasmanian devils’ transmissible cancer: Izarbe Aísa Marín Genetics Bachelor’s Degree What is the future? Final Project | June 2017 Introduction Devil Facial Tumor Disease 1Why is Tasmanian devils’ cancer incidence so high? 2Introduction to transmissible cancers Carcinogenesis is thought to occur via Peto’s Paradox represents the lack of accumulation of mutations and mutation correlation between cancer prevalence rates depend on cell number, which and body size or lifespan and it can be Primary Mode of Lack of Capacity for correlates with body size and lifespan. useful to explore cases that are far tumor’s origin transmission allorecognition infinite growth Then, large and long-lived animals from what is expected. Tasmanian should have more cancers than smaller devils suffer from Devil Facial Tumor and shorter-lived ones, due to increased Disease (DFTD), a lethal transmissible The ancestral type of DTDF is thought to be derived from a Schwann cell (clonal number of cell divisions. cancer that is threatening the species origin) and it is transmitted by biting during mating or feeding interactions. to extinction. (2) (1) y = 0,0815 - 0,0061x [y=%Tumors; x=Log(Mass[x]*LifeSpan[y])] 10x DFTD was first reported in Mount William National Park, northeastern Tasmania, in 1996. In 20 years, the disease has spread to more than 85% Forestier of wild Tasmanian devil Peninsula populations, causing severe declines. Immunology of DFTD 3Why devils immune system do not recognize DFTD? (3) Deficiency of devil Marsupials’ immune system is different immune system from, rather than inferior to mammals’ immune system. Immunological Low genetic Slower immune responses tolerance diversity facilitate early transmission events. -

Ribavirin) Tablets Initial U.S
HIGHLIGHTS OF PRESCRIBING INFORMATION ------------------------------ CONTRAINDICATIONS ----------------------------- These highlights do not include all the information needed to use • Pregnant women and men whose female partners are pregnant (4, 5.1, COPEGUS safely and effectively. See full prescribing information for 8.1) COPEGUS. • Hemoglobinopathies (4) • Coadministration with didanosine (4, 7.1) ® COPEGUS (ribavirin) Tablets Initial U.S. Approval: 2002 COPEGUS in combination with PEGASYS is contraindicated in patients with: WARNING: RISK OF SERIOUS DISORDERS AND RIBAVIRIN • Autoimmune hepatitis (4) ASSOCIATED EFFECTS • Hepatic decompensation in cirrhotic patients (4, 5.3) See full prescribing information for complete boxed warning. • Ribavirin monotherapy, including COPEGUS, is not effective for ----------------------- WARNINGS AND PRECAUTIONS ---------------------- the treatment of chronic hepatitis C virus infection (Boxed • Birth defects and fetal death with ribavirin: Do not use in pregnancy and Warning). for 6 months after treatment. Patients must have a negative pregnancy • The hemolytic anemia associated with ribavirin therapy may result test prior to therapy, use at least 2 forms of contraception and undergo in worsening of cardiac disease and lead to fatal and nonfatal monthly pregnancy tests (4, 5.1, 8.1) myocardial infarctions. Patients with a history of significant or unstable cardiac disease should not be treated with COPEGUS (2.3, PEGASYS/COPEGUS: Patients exhibiting the following conditions should be 5.2, 6.1). closely monitored and may require dose reduction or discontinuation of • Significant teratogenic and embryocidal effects have been therapy: demonstrated in all animal species exposed to ribavirin. Therefore, • Hemolytic anemia may occur with a significant initial drop in COPEGUS is contraindicated in women who are pregnant and in hemoglobin. -

Combination Therapy for Chronic Hepatitis B: Current Indications
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by PubMed Central Curr Hepatitis Rep (2011) 10:98–105 DOI 10.1007/s11901-011-0095-1 Combination Therapy for Chronic Hepatitis B: Current Indications Navin Paul & Steven-Huy Han Published online: 19 February 2011 # The Author(s) 2011. This article is published with open access at Springerlink.com Abstract Hepatitis B infection remains a major public infected adults in the United States alone and an annual health problem globally and in the United States, with financial burden of $1.3 billion [1, 2•]. Currently available significant use of healthcare resources. Several therapeu- therapeutic options include both parenteral and oral agents, tic agents active against viral and host targets are which act on various host and viral targets. These include currently available for its treatment. The success of medications such as standard interferon and pegylated combination therapy in HIV infection, which has simi- interferon (peg-interferon), which target receptors on the larities to hepatitis B in both therapeutic targets and host cell membranes, and nucleotide and nucleoside treatment options, stimulated studies on the efficacy and analogues, which inhibit HBV RNA-dependent DNA safety of various combinations of available drugs in the polymerase (lamivudine, telbivudine, entecavir, adefovir treatment of hepatitis B infection. In this review, we dipivoxil, and tenofovir disoproxil fumarate) [3]. analyze the current role of combination therapy in The availability of agents acting on different targets chronic hepatitis B infection. makes the option of combination therapy to achieve better therapeutic results particularly attractive. -

Journal of Carcinogenesis Biomed Central
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by PubMed Central Journal of Carcinogenesis BioMed Central Editorial Open Access New paradigms, new Hopes: the need for socially responsible research on carcinogenesis Gopala Kovvali* Address: Gopala Kovvali Ph.D. Editor-in-Chief, Journal of Carcinogenesis, Founder President, Carcinogenesis Foundation, 22 Heritage Drive, Edison, NJ 08820, USA Email: Gopala Kovvali* - [email protected] * Corresponding author Published: 21 November 2005 Received: 15 November 2005 Accepted: 21 November 2005 Journal of Carcinogenesis 2005, 4:22 doi:10.1186/1477-3163-4-22 This article is available from: http://www.carcinogenesis.com/content/4/1/22 © 2005 Kovvali; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. It has been three years since the publication of the first The formation of the Carcinogenesis Foundation is a his- article in the Journal of Carcinogenesis; it was the editorial toric opportunity. While its goal is to promote and that espoused the need for the launch of the journal. Hav- advance research in the field of carcinogenesis, it has a ing seen three springs and three falls, it is time to ask specialized mission of understanding the phenomenon of where we are as a journal and where we want to be in the increased cancer incidence among individuals who years to come. migrate to the western countries. -
Principles of Cancer Prevention and Will Emphasize the Scientific Underpinnings of This Emerging Discipline
Seminars in Oncology Nursing, Vol 21, No 4 (November), 2005: pp 229-235 229 OBJECTIVE: To summarize the scientific prin- ciples underlying cancer preven- tion. PRINCIPLES OF DATA SOURCES: Articles, text books, personal com- CANCER munications, and experience. CONCLUSION: PREVENTION The scientific basis of cancer pre- vention is complex and involves experimental and epidemiologic approaches and clinical trials. FRANK L. MEYSKENS,JR AND PATRICIA TULLY IMPLICATIONS FOR NURSING PRACTICE: ANCER prevention has classically encompassed As more information becomes three large areas of clinical practice: prevention, available regarding proven and screening, and early detection. Several excellent potential cancer-prevention strate- reviews and book chapters have been published gies, oncology nurses are regu- involving these topics.1-3 The importance of bio- larly called upon to guide patients Clogical and molecular markers as potential surrogates have been and others in making choices re- emphasized in the past several years,4,5 and more recently precan- garding preventative options. It is cers or intraepithelial neoplasia (IEN) have become a target.6,7 The important for oncology nurses to integration of the well-established approaches of prevention, stay abreast of this growing body screening, and early detection with biological measures of disease of knowledge. risk, progression, and prognosis has become the hallmark of mod- ern cancer prevention (see Fig 1). In this article we will review the principles of cancer prevention and will emphasize the scientific underpinnings of this emerging discipline. The principles of cancer prevention have evolved from three separate scientific disciplines: carcinogenesis, epidemiology, and clinical trials. Many other areas From the Department of Medicine and of science and medicine, including genetics and the behavioral Biological Chemistry, Chao Family Com- sciences, are contributing to this evolving and complex field. -

Pegintron.Com
HIGHLIGHTS OF PRESCRIBING INFORMATION Hypothyroidism, hyperthyroidism, hyperglycemia, diabetes mellitus These highlights do not include all the information needed to use that cannot be effectively treated by medication. (5.4) PEGINTRON safely and effectively. See full prescribing New or worsening ophthalmologic disorders. (5.5) information for PEGINTRON. Ischemic and hemorrhagic cerebrovascular events. (5.6) ® Severe decreases in neutrophil or platelet counts. (5.7) PEGINTRON (peginterferon alfa-2b) injection, for subcutaneous History of autoimmune disorders. (5.8) use Pancreatitis and ulcerative or hemorrhagic/ischemic colitis and Initial U.S. Approval: 2001 pancreatitis. (5.9, 5.10) Pulmonary infiltrates or pulmonary function impairment. (5.11) WARNING: RISK OF SERIOUS DISORDERS Child-Pugh score greater than 6 (class B and C). (4, 5.12) See full prescribing information for complete boxed warning. Increased creatinine levels in patients with renal insufficiency. May cause or aggravate fatal or life-threatening (5.13) neuropsychiatric, autoimmune, ischemic, and infectious Serious, acute hypersensitivity reactions and cutaneous eruptions. disorders. Monitor closely and withdraw therapy with (5.14) persistently severe or worsening signs or symptoms of the Dental/periodontal disorders reported with combination therapy. above disorders. (5) (5.16) Hypertriglyceridemia may result in pancreatitis (e.g., triglycerides ----------------------------INDICATIONS AND USAGE---------------------------- greater than 1000 mg/dL). (5.17) PEGINTRON is an antiviral indicated for treatment of Chronic Hepatitis Weight loss and growth inhibition reported during combination C (CHC) in patients with compensated liver disease. (1.1) therapy in pediatric patients. Long-term growth inhibition (height) reported in some patients. (5.18) ----------------------- DOSAGE AND ADMINISTRATION ----------------------- Peripheral neuropathy when used in combination with telbivudine. -

Carcinogenesis
Chapter 3 Chapter 3 Carcinogenesis CONTENTS Oral Carcinoma and Smokeless Tobacco Use: A Clinical Profile W. Frederick McGuirt and Anna Wray .................................................. 91 Introduction .................................................................................... 91 Patients ............................................................................................ 91 Field Cancerization ......................................................................... 92 Discussion........................................................................................ 93 References ........................................................................................ 95 Chemical Composition of Smokeless Tobacco Products Klaus D. Brunnemann and Dietrich Hoffmann ..................................... 96 Introduction .................................................................................... 96 Chemical Composition ................................................................... 97 Carcinogenic Agents in ST .............................................................. 97 Carcinogenic N-Nitrosamines ....................................................... 100 TSNA .............................................................................................. 101 Control of Carcinogens in ST ....................................................... 104 References ...................................................................................... 106 Carcinogenesis of Smokeless Tobacco Dietrich Hoffmann, Abraham -

Telbivudine Decreases Proportion of Peripheral Blood CD4+CD25+Cd127low T Cells in Parallel with Inhibiting Hepatitis B Virus DNA
2024 MOLECULAR MEDICINE REPORTS 9: 2024-2030, 2014 Telbivudine decreases proportion of peripheral blood CD4+CD25+CD127low T cells in parallel with inhibiting hepatitis B virus DNA ZEHUI YAN1, JIJUN ZHOU1, MENGJUN ZHANG2, XIAOLAN FU2, YUZHANG WU2 and YUMING WANG1 1Institute of Infectious Diseases, Southwest Hospital, Third Military Medical University; 2Institute of Immunology, Third Military Medical University, Chongqing 400038, P.R. China Received July 11, 2013; Accepted February 25, 2014 DOI: 10.3892/mmr.2014.2042 Abstract. Regulatory T cells (Treg) have significant roles in the Introduction immunopathology of patients with chronic hepatitis B (CHB) and exhibit an evident correlation with antiviral immunity Hepatitis B virus (HBV) infection is a serious public health when antiviral therapy is applied. In order to investigate how problem affecting more than 400 million individuals world- circulating Tregs are affected by telbivudine treatment and wide (1). During HBV infection, the host immune responses, its significance in patients with CHB, peripheral blood mono- particularly the cellular immune response, mediate clearance nuclear cells (PBMCs) were isolated and the proportions of of HBV infection and the pathogenesis of liver injury is circulating cluster of differentiation (CD)4+CD25+CD127low and dependent on the balance between HBV replication and the CD8+CD25+ T cells of CHB patients prior to and during the viral‑specific cytotoxic T‑lymphocyte (CTL) response (2). In three or six months of treatment were assessed and detected by patients with an acute self-limiting HBV infection, the CD4+ flow cytometric analysis. The levels of orkheadf /winged helix and CD8+ T-cell response with T helper 1 type cytokine transcription factor (Foxp3) mRNA were also quantified using profile is crucial for the control of the infection (3,4). -

Sebivo® (Telbivudine)
Sebivo® (telbivudine) SINGLE TECHNOLOGY APPRAISAL (STA) MANUFACTURER SUBMISSION OF EVIDENCE 1 List of Abbreviations A&E Accident and emergency AASLD American Association for the Study of Liver Diseases AE Adverse events ALT Alanine aminotransferase APASL Asia Pacific Association for the Study of Liver AST Aspartate aminotransferase BSC Best standard care CC Compensated cirrhosis CDC Centres for Disease Control CHB Chronic hepatitis B CI Confidence interval CK Creatine kinase DCC Decompensated cirrhosis DNA Deoxyribonucleic acid EASL European Association for the Study of the Liver EMEA European Medicines Evaluation Agency ER Emergency room ESRD End stage renal disease ETV Entecavir HBcAg Hepatitis B core antigen HBeAg Hepatitis B e antigen HBIG Hepatitis B immunoglobulin HBsAg Hepatitis B surface antigen HBV Hepatitis B virus HCC Hepatocellular carcinoma ICER Incremental cost effectiveness ratio IFN Interferon alfa ITT Intention to treat population LAM Lamivudine LDT Telbivudine Mg Milligram NRTIs Nucleoside Analogue Reverse Transcriptase Inhibitors ns Not significant OR Odds ratio PCR Polymerase chain reaction PEG IFN Pegylated Interferon 2 PI Product information QALY Quality adjusted life year RNA Ribonucleic acid RR Relative risk SD Standard deviation SmPC Summary of Product Characteristics TGA Therapeutic Goods Administration ULN Upper limit of normal 3 Appendices Provided Separately from Main Submission The appendices below are provided electronically on CD-Rom (separate from the main submission) to assist the Evidence Review Group -

TYZEKA™ (Telbivudine) Tablets
NDA 22-011 TYZEKA™ (telbivudine) Tablets Rx only Prescribing Information WARNINGS Lactic acidosis and severe hepatomegaly with steatosis, including fatal cases, have been reported with the use of nucleoside analogues alone or in combination with antiretrovirals. Severe acute exacerbations of hepatitis B have been reported in patients who have discontinued anti-hepatitis B therapy, including TYZEKA™ (telbivudine). Hepatic function should be monitored closely with both clinical and laboratory follow-up for at least several months in patients who discontinue anti-hepatitis B therapy. If appropriate, resumption of anti-hepatitis B therapy may be warranted. (See WARNINGS.) DESCRIPTION TYZEKA™ is the trade name for telbivudine, a synthetic thymidine nucleoside analogue with activity against hepatitis B virus (HBV). The chemical name for telbivudine is 1- ((2S,4R,5S)-4-hydroxy-5-hydroxymethyltetrahydrofuran-2-y1)-5-methyl-1H-pyrimidine- 2,4-dione, or 1-(2-deoxy-β-L-ribofuranosyl)-5-methyluracil. Telbivudine is the unmodified β-L enantiomer of the naturally occurring nucleoside, thymidine. Its molecular formula is C10H14N2O5, which corresponds to a molecular weight of 242.23. Telbivudine has the following structural formula: O CH3 HN O N OH O OH Telbivudine is a white to slightly yellowish powder. Telbivudine is sparingly soluble in water (>20 mg/mL), and very slightly soluble in absolute ethanol (0.7 mg/mL) and n- octanol (0.1 mg/mL). Page 8 of 17 TYZEKA™ (telbivudine) film-coated tablets are available for oral administration in 600 mg strength. TYZEKA 600 mg film-coated tablets contain the following inactive ingredients: colloidal silicon dioxide, magnesium stearate, microcrystalline cellulose, povidone, and sodium starch glycolate. -

Mitochondrial Metabolism in Carcinogenesis and Cancer Therapy
cancers Review Mitochondrial Metabolism in Carcinogenesis and Cancer Therapy Hadia Moindjie 1,2, Sylvie Rodrigues-Ferreira 1,2,3 and Clara Nahmias 1,2,* 1 Inserm, Institut Gustave Roussy, UMR981 Biomarqueurs Prédictifs et Nouvelles Stratégies Thérapeutiques en Oncologie, 94800 Villejuif, France; [email protected] (H.M.); [email protected] (S.R.-F.) 2 LabEx LERMIT, Université Paris-Saclay, 92296 Châtenay-Malabry, France 3 Inovarion SAS, 75005 Paris, France * Correspondence: [email protected]; Tel.: +33-142-113-885 Simple Summary: Reprogramming metabolism is a hallmark of cancer. Warburg’s effect, defined as increased aerobic glycolysis at the expense of mitochondrial respiration in cancer cells, opened new avenues of research in the field of cancer. Later findings, however, have revealed that mitochondria remain functional and that they actively contribute to metabolic plasticity of cancer cells. Understand- ing the mechanisms by which mitochondrial metabolism controls tumor initiation and progression is necessary to better characterize the onset of carcinogenesis. These studies may ultimately lead to the design of novel anti-cancer strategies targeting mitochondrial functions. Abstract: Carcinogenesis is a multi-step process that refers to transformation of a normal cell into a tumoral neoplastic cell. The mechanisms that promote tumor initiation, promotion and progression are varied, complex and remain to be understood. Studies have highlighted the involvement of onco- genic mutations, genomic instability and epigenetic alterations as well as metabolic reprogramming, Citation: Moindjie, H.; in different processes of oncogenesis. However, the underlying mechanisms still have to be clarified. Rodrigues-Ferreira, S.; Nahmias, C. Mitochondria are central organelles at the crossroad of various energetic metabolisms. -

Cancer Biology Introduction Proto-Oncogenes Tumor
Introduction • Tissue homeostasis depends on the regulated cell division and self-elimination (programmed cell Cancer Biology death) of each of its constituent members except its stem cells • A tumor arises as a result of uncontrolled cell division and failure for self-elimination Chapter 18 • Alterations in three groups of genes are responsible Eric J. Hall., Amato Giaccia, for the deregulated control mechanisms that are the hallmarks of cancer cells: proto-oncogenes, tumor- Radiobiology for the Radiologist supressor genes, and DNA stability genes Proto-oncogenes Tumor-suppressor genes • Proto-oncogenes are components of signaling • Tumor-suppressor genes are also components of networks that act as positive growth the same signaling networks as proto-oncogenes, except that they act as negative growth regulators regulators in response to mitogens, cytokines, • They modulate proliferation and survival by and cell-to-cell contact antagonizing the biochemical functions of proto- • A gain-of-function mutation in only one copy oncogenes or responding to unchecked growth signals of a protooncogene results in a dominantly • In contrast to oncogenes, inactivation of both acting oncogene that often fails to respond to copies of tumor-suppressor genes is required for extracellular signals loss of function in most cases DNA stability genes Mechanisms of carcinogenesis • DNA stability genes form a class of genes • A single genetic alteration that leads to the involved in both monitoring and activation of an oncogene or loss of a tumor maintaining