Examination of Independent Prognostic Power of Gene Expressions and Histopathological Imaging Features in Cancer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Noelia Díaz Blanco
Effects of environmental factors on the gonadal transcriptome of European sea bass (Dicentrarchus labrax), juvenile growth and sex ratios Noelia Díaz Blanco Ph.D. thesis 2014 Submitted in partial fulfillment of the requirements for the Ph.D. degree from the Universitat Pompeu Fabra (UPF). This work has been carried out at the Group of Biology of Reproduction (GBR), at the Department of Renewable Marine Resources of the Institute of Marine Sciences (ICM-CSIC). Thesis supervisor: Dr. Francesc Piferrer Professor d’Investigació Institut de Ciències del Mar (ICM-CSIC) i ii A mis padres A Xavi iii iv Acknowledgements This thesis has been made possible by the support of many people who in one way or another, many times unknowingly, gave me the strength to overcome this "long and winding road". First of all, I would like to thank my supervisor, Dr. Francesc Piferrer, for his patience, guidance and wise advice throughout all this Ph.D. experience. But above all, for the trust he placed on me almost seven years ago when he offered me the opportunity to be part of his team. Thanks also for teaching me how to question always everything, for sharing with me your enthusiasm for science and for giving me the opportunity of learning from you by participating in many projects, collaborations and scientific meetings. I am also thankful to my colleagues (former and present Group of Biology of Reproduction members) for your support and encouragement throughout this journey. To the “exGBRs”, thanks for helping me with my first steps into this world. Working as an undergrad with you Dr. -

RNA Editing at Baseline and Following Endoplasmic Reticulum Stress
RNA Editing at Baseline and Following Endoplasmic Reticulum Stress By Allison Leigh Richards A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy (Human Genetics) in The University of Michigan 2015 Doctoral Committee: Professor Vivian G. Cheung, Chair Assistant Professor Santhi K. Ganesh Professor David Ginsburg Professor Daniel J. Klionsky Dedication To my father, mother, and Matt without whom I would never have made it ii Acknowledgements Thank you first and foremost to my dissertation mentor, Dr. Vivian Cheung. I have learned so much from you over the past several years including presentation skills such as never sighing and never saying “as you can see…” You have taught me how to think outside the box and how to create and explain my story to others. I would not be where I am today without your help and guidance. Thank you to the members of my dissertation committee (Drs. Santhi Ganesh, David Ginsburg and Daniel Klionsky) for all of your advice and support. I would also like to thank the entire Human Genetics Program, and especially JoAnn Sekiguchi and Karen Grahl, for welcoming me to the University of Michigan and making my transition so much easier. Thank you to Michael Boehnke and the Genome Science Training Program for supporting my work. A very special thank you to all of the members of the Cheung lab, past and present. Thank you to Xiaorong Wang for all of your help from the bench to advice on my career. Thank you to Zhengwei Zhu who has helped me immensely throughout my thesis even through my panic. -

The Genomics of Oral Poliovirus Vaccine
THE GENOMICS OF ORAL POLIOVIRUS VACCINE RESPONSE IN BANGLADESHI INFANTS by Genevieve L. Wojcik, MHS A dissertation submitted to the Johns Hopkins University in conformity with the requirements for the degree of Doctor of Philosophy Baltimore, Maryland, USA October 2013 © Genevieve L. Wojcik All Rights Reserved Abstract The success of Oral Poliovirus Vaccine (OPV) in eradicating poliovirus has set an example for the immense potential of oral vaccines in preventing enteric infections. It is widely considered the standard for oral vaccines aiming to elicit a mucosal immune response. Despite being validated in diverse populations worldwide, there still remain some individuals that fail to mount an adequate response to vaccination with OPV. It has been hypothesized that this may be due to host genetics, as the heritability is estimated to be high (60%) and there have been ethnic differences in response. To address this question we conducted a genome-wide association study (GWAS) in 357 Bangladeshi children comparing individuals that fail to mount an immune response to high responders of OPV. Four different approaches were conducted to elucidate genetic risk loci: (1) a traditional GWAS analysis, (2) a correlation of the GWAS results with signatures of positive selection, (3) an application of gene-level methods to the GWAS results, and (4) an application of pathway-level methods to the GWAS results. Because there is no consensus as to the best gene- and pathway-level methods, a simulation experiment was conducted to systematically evaluate their relative performance. The traditional GWAS assessed the association of 6.6 million single nucleotide polymorphisms (SNPs) across the human genome, adjusted for stunting (height-for-age Z-score (HAZ) < -2). -

Original Article a Database and Functional Annotation of NF-Κb Target Genes
Int J Clin Exp Med 2016;9(5):7986-7995 www.ijcem.com /ISSN:1940-5901/IJCEM0019172 Original Article A database and functional annotation of NF-κB target genes Yang Yang, Jian Wu, Jinke Wang The State Key Laboratory of Bioelectronics, Southeast University, Nanjing 210096, People’s Republic of China Received November 4, 2015; Accepted February 10, 2016; Epub May 15, 2016; Published May 30, 2016 Abstract: Backgrounds: The previous studies show that the transcription factor NF-κB always be induced by many inducers, and can regulate the expressions of many genes. The aim of the present study is to explore the database and functional annotation of NF-κB target genes. Methods: In this study, we manually collected the most complete listing of all NF-κB target genes identified to date, including the NF-κB microRNA target genes and built the database of NF-κB target genes with the detailed information of each target gene and annotated it by DAVID tools. Results: The NF-κB target genes database was established (http://tfdb.seu.edu.cn/nfkb/). The collected data confirmed that NF-κB maintains multitudinous biological functions and possesses the considerable complexity and diversity in regulation the expression of corresponding target genes set. The data showed that the NF-κB was a central regula- tor of the stress response, immune response and cellular metabolic processes. NF-κB involved in bone disease, immunological disease and cardiovascular disease, various cancers and nervous disease. NF-κB can modulate the expression activity of other transcriptional factors. Inhibition of IKK and IκBα phosphorylation, the decrease of nuclear translocation of p65 and the reduction of intracellular glutathione level determined the up-regulation or down-regulation of expression of NF-κB target genes. -

Promoterless Transposon Mutagenesis Drives Solid Cancers Via Tumor Suppressor Inactivation
bioRxiv preprint doi: https://doi.org/10.1101/2020.08.17.254565; this version posted August 17, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 1 Promoterless Transposon Mutagenesis Drives Solid Cancers via Tumor Suppressor Inactivation 2 Aziz Aiderus1, Ana M. Contreras-Sandoval1, Amanda L. Meshey1, Justin Y. Newberg1,2, Jerrold M. Ward3, 3 Deborah Swing4, Neal G. Copeland2,3,4, Nancy A. Jenkins2,3,4, Karen M. Mann1,2,3,4,5,6,7, and Michael B. 4 Mann1,2,3,4,6,7,8,9 5 1Department of Molecular Oncology, Moffitt Cancer Center & Research Institute, Tampa, FL, USA 6 2Cancer Research Program, Houston Methodist Research Institute, Houston, Texas, USA 7 3Institute of Molecular and Cell Biology, Agency for Science, Technology and Research (A*STAR), 8 Singapore, Republic of Singapore 9 4Mouse Cancer Genetics Program, Center for Cancer Research, National Cancer Institute, Frederick, 10 Maryland, USA 11 5Departments of Gastrointestinal Oncology & Malignant Hematology, Moffitt Cancer Center & Research 12 Institute, Tampa, FL, USA 13 6Cancer Biology and Evolution Program, Moffitt Cancer Center & Research Institute, Tampa, FL, USA 14 7Department of Oncologic Sciences, Morsani College of Medicine, University of South Florida, Tampa, FL, 15 USA. 16 8Donald A. Adam Melanoma and Skin Cancer Research Center of Excellence, Moffitt Cancer Center, Tampa, 17 FL, USA 18 9Department of Cutaneous Oncology, Moffitt Cancer Center & Research Institute, Tampa, FL, USA 19 These authors contributed equally: Aziz Aiderus, Ana M. -
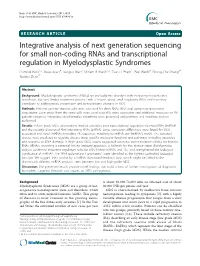
Integrative Analysis of Next Generation Sequencing for Small Non-Coding
Beck et al. BMC Medical Genomics 2011, 4:19 http://www.biomedcentral.com/1755-8794/4/19 RESEARCHARTICLE Open Access Integrative analysis of next generation sequencing for small non-coding RNAs and transcriptional regulation in Myelodysplastic Syndromes Dominik Beck1,2, Steve Ayers4, Jianguo Wen3, Miriam B Brandl1,2, Tuan D Pham1, Paul Webb4, Chung-Che Chang3*, Xiaobo Zhou1* Abstract Background: Myelodysplastic Syndromes (MDSS) are pre-leukemic disorders with increasing incident rates worldwide, but very limited treatment options. Little is known about small regulatory RNAs and how they contribute to pathogenesis, progression and transcriptome changes in MDS. Methods: Patients’ primary marrow cells were screened for short RNAs (RNA-seq) using next generation sequencing. Exon arrays from the same cells were used to profile gene expression and additional measures on 98 patients obtained. Integrative bioinformatics algorithms were proposed, and pathway and ontology analysis performed. Results: In low-grade MDS, observations implied extensive post-transcriptional regulation via microRNAs (miRNA) and the recently discovered Piwi interacting RNAs (piRNA). Large expression differences were found for MDS- associated and novel miRNAs, including 48 sequences matching to miRNA star (miRNA*) motifs. The detected species were predicted to regulate disease stage specific molecular functions and pathways, including apoptosis and response to DNA damage. In high-grade MDS, results suggested extensive post-translation editing via transfer RNAs (tRNAs), providing a potential link for reduced apoptosis, a hallmark for this disease stage. Bioinformatics analysis confirmed important regulatory roles for MDS linked miRNAs and TFs, and strengthened the biological significance of miRNA*. The “RNA polymerase II promoters” were identified as the tightest controlled biological function. -

SUPPORTING INFORMATION for Regulation of Gene Expression By
SUPPORTING INFORMATION for Regulation of gene expression by the BLM helicase correlates with the presence of G4 motifs Giang Huong Nguyen1,2, Weiliang Tang3, Ana I. Robles1, Richard P. Beyer4, Lucas T. Gray5, Judith A. Welsh1, Aaron J. Schetter1, Kensuke Kumamoto1,6, Xin Wei Wang1, Ian D. Hickson2,7, Nancy Maizels5, 3,8 1 Raymond J. Monnat, Jr. and Curtis C. Harris 1Laboratory of Human Carcinogenesis, National Cancer Institute, National Institutes of Health, Bethesda, Maryland, U.S.A; 2Department of Medical Oncology, Weatherall Institute of Molecular Medicine, John Radcliffe Hospital, University of Oxford, Oxford, U.K.; 3Department of Pathology, University of Washington, Seattle, WA U.S.A.; 4 Center for Ecogenetics and Environmental Health, University of Washington, Seattle, WA U.S.A.; 5Department of Immunology and Department of Biochemistry, University of Washington, Seattle, WA U.S.A.; 6Department of Organ Regulatory Surgery, Fukushima Medical University, Fukushima, Japan; 7Cellular and Molecular Medicine, Nordea Center for Healthy Aging, University of Copenhagen, Denmark; 8Department of Genome Sciences, University of WA, Seattle, WA U.S.A. SI Index: Supporting Information for this manuscript includes the following 19 items. A more detailed Materials and Methods section is followed by 18 Tables and Figures in order of their appearance in the manuscript text: 1) SI Materials and Methods 2) Figure S1. Study design and experimental workflow. 3) Figure S2. Immunoblot verification of BLM depletion from human fibroblasts. 4) Figure S3. PCA of mRNA and miRNA expression in BLM-depleted human fibroblasts. 5) Figure S4. qPCR confirmation of mRNA array data. 6) Table S1. BS patient and control detail. -
Prion Characterization Using Cell Based Approaches
University of Kentucky UKnowledge Theses and Dissertations--Microbiology, Microbiology, Immunology, and Molecular Immunology, and Molecular Genetics Genetics 2012 PRION CHARACTERIZATION USING CELL BASED APPROACHES Vadim Khaychuk University of Kentucky, [email protected] Right click to open a feedback form in a new tab to let us know how this document benefits ou.y Recommended Citation Khaychuk, Vadim, "PRION CHARACTERIZATION USING CELL BASED APPROACHES" (2012). Theses and Dissertations--Microbiology, Immunology, and Molecular Genetics. 2. https://uknowledge.uky.edu/microbio_etds/2 This Doctoral Dissertation is brought to you for free and open access by the Microbiology, Immunology, and Molecular Genetics at UKnowledge. It has been accepted for inclusion in Theses and Dissertations--Microbiology, Immunology, and Molecular Genetics by an authorized administrator of UKnowledge. For more information, please contact [email protected]. STUDENT AGREEMENT: I represent that my thesis or dissertation and abstract are my original work. Proper attribution has been given to all outside sources. I understand that I am solely responsible for obtaining any needed copyright permissions. I have obtained and attached hereto needed written permission statements(s) from the owner(s) of each third-party copyrighted matter to be included in my work, allowing electronic distribution (if such use is not permitted by the fair use doctrine). I hereby grant to The University of Kentucky and its agents the non-exclusive license to archive and make accessible my work in whole or in part in all forms of media, now or hereafter known. I agree that the document mentioned above may be made available immediately for worldwide access unless a preapproved embargo applies. -
Revealing New Candidate Genes for Reproductive Traits in Pigs: Combining Bayesian GWAS and Functional Pathways Lucas L
Verardo et al. Genet Sel Evol (2016) 48:9 Genetics DOI 10.1186/s12711-016-0189-x Selection Evolution RESEARCH ARTICLE Open Access Revealing new candidate genes for reproductive traits in pigs: combining Bayesian GWAS and functional pathways Lucas L. Verardo1,2*, Fabyano F. Silva1, Marcos S. Lopes2,3, Ole Madsen2, John W. M. Bastiaansen2, Egbert F. Knol3, Mathew Kelly4, Luis Varona5, Paulo S. Lopes1 and Simone E. F. Guimarães1 Abstract Background: Reproductive traits such as number of stillborn piglets (SB) and number of teats (NT) have been evalu- ated in many genome-wide association studies (GWAS). Most of these GWAS were performed under the assumption that these traits were normally distributed. However, both SB and NT are discrete (e.g. count) variables. Therefore, it is necessary to test for better fit of other appropriate statistical models based on discrete distributions. In addition, although many GWAS have been performed, the biological meaning of the identified candidate genes, as well as their functional relationships still need to be better understood. Here, we performed and tested a Bayesian treatment of a GWAS model assuming a Poisson distribution for SB and NT in a commercial pig line. To explore the biological role of the genes that underlie SB and NT and identify the most likely candidate genes, we used the most significant single nucleotide polymorphisms (SNPs), to collect related genes and generated gene-transcription factor (TF) networks. Results: Comparisons of the Poisson and Gaussian distributions showed that the Poisson model was appropriate for SB, while the Gaussian was appropriate for NT. The fitted GWAS models indicated 18 and 65 significant SNPs with one and nine quantitative trait locus (QTL) regions within which 18 and 57 related genes were identified for SB and NT, respectively. -

Promoterless Transposon Mutagenesis Drives Solid Cancers Via Tumor Suppressor Inactivation
cancers Article Promoterless Transposon Mutagenesis Drives Solid Cancers via Tumor Suppressor Inactivation Aziz Aiderus 1,† , Ana M. Contreras-Sandoval 1,† , Amanda L. Meshey 1,†, Justin Y. Newberg 1,2,‡, Jerrold M. Ward 3,§, Deborah A. Swing 4, Neal G. Copeland 2,3,4,k, Nancy A. Jenkins 2,3,4,k, Karen M. Mann 1,2,3,4,5,6,7,* and Michael B. Mann 1,2,3,4,6,7,8,9,* 1 Department of Molecular Oncology, Moffitt Cancer Center & Research Institute, Tampa, FL 33612, USA; Aziz.Aiderus@moffitt.org (A.A.); Ana.ContrerasSandoval@moffitt.org (A.M.C.-S.); Amanda.Meshey@moffitt.org (A.L.M.); [email protected] (J.Y.N.) 2 Cancer Research Program, Houston Methodist Research Institute, Houston, TX 77030, USA; [email protected] (N.G.C.); [email protected] (N.A.J.) 3 Institute of Molecular and Cell Biology, Agency for Science, Technology and Research (A*STAR), Singapore 138673, Singapore; [email protected] 4 Mouse Cancer Genetics Program, Center for Cancer Research, National Cancer Institute, Frederick, MD 21702, USA; [email protected] 5 Departments of Gastrointestinal Oncology & Malignant Hematology, Moffitt Cancer Center & Research Institute, Tampa, FL 33612, USA 6 Cancer Biology and Evolution Program, Moffitt Cancer Center & Research Institute, Tampa, FL 33612, USA 7 Department of Oncologic Sciences, Morsani College of Medicine, University of South Florida, Tampa, FL 33612, USA 8 Donald A. Adam Melanoma and Skin Cancer Research Center of Excellence, Moffitt Cancer Center, Tampa, FL 33612, USA 9 Department of Cutaneous Oncology, Moffitt Cancer Center & Research Institute, Tampa, FL 33612, USA * Correspondence: Karen.Mann@moffitt.org (K.M.M.); Michael.Mann@moffitt.org (M.B.M.) † These authors contributed equally. -

Genomic and Molecular Screenings Identify Different Mechanisms For
Published OnlineFirst April 10, 2017; DOI: 10.1158/1535-7163.MCT-17-0104 Cancer Biology and Signal Transduction Molecular Cancer Therapeutics Genomic and Molecular Screenings Identify Different Mechanisms for Acquired Resistance to MET Inhibitors in Lung Cancer Cells Pol Gimenez-Xavier1, Eva Pros1, Ester Bonastre1, Sebastian Moran2, Ana Aza1, Osvaldo Grana~ 3, Gonzalo Gomez-Lopez3, Sophia Derdak4,5, Marc Dabad4,5, Anna Esteve-Codina4,5, Jose R. Hernandez Mora2, Diana Salinas-Chaparro1, Manel Esteller2,6, David Pisano3, and Montse Sanchez-Cespedes1 Abstract The development of resistance to tyrosine kinase inhibitors groups of resistant cells. In one of these, the cells have acquired (TKI) limits the long-term efficacy of cancer treatments involving sensitivity to erlotinib, concomitantly with mutations of the them. We aimed to understand the mechanisms that underlie KIRREL, HDAC11, HIATL1, and MAPK1IP1L genes, among acquired resistance (AR) to MET inhibitors in lung cancer. EBC1 others. In the other group, some cells have acquired inactivation cells, which have MET amplification and are sensitive to TKIs of neurofibromatosis type 2 (NF2) concomitantly with strong against MET, were used to generate multiple clones with AR to a overexpression of NRG1 and a mutational profile that includes MET-TKI. Whole-exome sequencing, RNA sequencing, and global changes in LMLN and TOMM34. Multiple independent and DNA methylation analysis were used to scrutinize the genetic and simultaneous strategies lead to AR to the MET-TKIs in lung cancer molecular characteristics of the resistant cells. AR to the MET-TKI cells. The acquired sensitivity to erlotinib supports the known involved changes common to all resistant cells, that is, phenotypic crosstalk between MET and the HER family of receptors. -

Aberrant Downstream Mechanisms Following Depletion of KMT2C and KMT2D in Pancreatic Ductal Adenocarcinoma
Aberrant downstream mechanisms following depletion of KMT2C and KMT2D in Pancreatic Ductal Adenocarcinoma Joshua Benjamin Newton Dawkins Thesis submitted in partial fulfilment of the requirements of the degree of Doctor of Philosophy (PhD) at Barts and the London School of Medicine and Dentistry, Queen Mary University of London Barts Cancer Institute, Queen Mary University of London, Charterhouse Square, London EC1M 6BQ UK 2016 1 Statement of Originality I, Joshua Benjamin Newton Dawkins, confirm that the research included within this thesis is my own work or that where it has been carried out in collaboration with, or supported by others, that this is duly acknowledged below and my contribution indicated. Previously published material is also acknowledged below. I attest that I have exercised reasonable care to ensure that the work is original, and does not to the best of my knowledge break any UK law, infringe any third party’s copyright or other Intellectual Property Right, or contain any confidential material. I accept that the College has the right to use plagiarism detection software to check the electronic version of the thesis. I confirm that this thesis has not been previously submitted for the award of a degree by this, or any other, university. The copyright of this thesis rests with the author and no quotation from it or information derived from it may be published without the prior written consent of the author. Signature: Date: Details of collaboration and publications: - RNA sequencing and was carried out by Source Bioscience, William James House, Cowley Road, Cambridge UK. - Bioinformatic analysis of the clinically annotated patient gene expression datasets, and the RNA sequencing data were carried out by Dr Jun Wang at the Barts Cancer Institute, Queen Mary University of London, London UK.