First Report of AIDS
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Poland and the Peace Movement
Trinity College Trinity College Digital Repository Resist Newsletters Resist Collection 6-30-1981 Resist Newsletter, May-June 1981 Resist Follow this and additional works at: https://digitalrepository.trincoll.edu/resistnewsletter Recommended Citation Resist, "Resist Newsletter, May-June 1981" (1981). Resist Newsletters. 96. https://digitalrepository.trincoll.edu/resistnewsletter/96 --------RESIST----- May-June 1981 - 38 Union Square, Somerville, Mass. 02143 - Newsletter #140 a call to resist illegitimate authority POLAND AND THE WOMEN IN PEACE MOVEMENT EL ·SALVADOR FRANK BRODHEAD AMANDA CLAIBORNE What are the US government's goals in Poland? The lives of women are distinctly different from the Does it want a reformed version of the present govern lives of men, and this is no less true in developing coun ment? Or would it rather have a more Western-looking tries than in the US. Any general socio-economic por or neutralist government, even if this meant risking mili trait conceals this fact, as differences in employment, tary intervention by the Soviet Union? Or would the US health, education and other areas are made invisible by in fact welcome an invasion, an event which would be "sex-blind" research. likely to result in a drawn out war, as in Afghanistan, In all countries women suffer from hardships addi and would certainly drive many neutral nations into the tional to those of men. Some of these result from sexism US camp? Certainly any Soviet move in Poland would or ''machismo,'' or whatever name it goes under; and provide a large increase in popular support for Reagan's so one is not surprised to discover legal and "cultural" aggressive foreign policy: what military responses would discrimination against women in the countries of Latin the US make to Soviet intervention? These and other America where, after all, the word "machismo" was questions make it important to think about the Polish coined. -

Federal Agencies Updating Base Year of Indexes to 1977
Technical Note Federal agencies updating Exhibit 1 . Schedule of dates for converting base year of indexes to 1977 BLS statistical series to a base year of 1977 =100 Scheduled Along with other Federal agencies, the Bureau of Labor Statistical series completion Statistics is changing the base year used in its statistical date indexes from 1967 to 1977. The rebasing of most BLS data: establishment series will be completed by December 1981, the target Employment Aggregate weekly hour indexes . July 1981 date for conversion of all Federal index numbers Aggregate weekly payroll indexes . July 1981 adopted by the Office of Federal Statistical Policy and Average weekly earnings indexes . July 1981 Standards. The BLS Producer, Consumer, and import Federal Government hours and and export price indexes and price-related indexes (such earnings indexes . July 1981 Gross and spendable earnings as the Spendable Earnings Series) will be rebased to indexes . February 1982 1977 with the release of data for January 1982. Price data Periodic revision Consumer Price Indexes . February 1982 The base period of Federal statistical indexes is re- Import and export price indexes . February 1982 Producer Price Indexes . February 1982 vised approximately every 10 years. In announcing the latest revision, the Office of Statistical Policy and Stan- Productivity data dards noted that reference periods are changed to "fa- Compensation per hour indexes . January 1981 cilitate the visual comprehension of rates of change Output per hour indexes . January 1981 from a base period that is not too distant in time." Prices indexes . January 1981 The Office of Statistical Policy chose the year 1977 Unit labor cost indexes . -

Polar Research Board Antarctic-Related Activities, June
Services, support, other SCAR, held in New Zealand 13-24 October 1980. Scientific Polar Research Board problems related to impending exploitation of living resources antarctic-related activities, and possible exploration of mineral resources of Antarctica June 1980-June 1981 were the central theme of the meeting. The structure, role, and future of SCAR were reviewed, and the constitution was mod- ified to allow each member nation a second (nonvoting) rep- resentative as an alternate delegate. New Groups of Specialists STAFF, POLAR RESEARCH BOARD on the Environmental Implications of Possible Mineral Explo- ration and Exploitation and on Antarctic Climate Research Polar Research Board were created (the latter to plan the antarctic component of the National Academy of Sciences National Research Council World Climate Research Program), and the specialist group on Washington, D.C. 20418 late Cenozoic studies was disbanded. A symposium on research in the Ross Sea region, 1957-1980, was held in con- The Polar Research Board (PRB), was established in 1958 to junction with the meeting; U.S. scientists presented 4 of 13 serve as a national advisory group on research in the polar papers, highlighting achievements and identifying directions regions. It adheres to the International Council of Scientific for future research. U.S. scientists head 2 of the 10 SCAR Work- Unions (icsu) Scientific Committee on Antarctic Research ing Groups and convene 2 of the 4 SCAR Groups of Specialists. The international program, Biological Investigations of (SCAR) on behalf of the National Academy of Sciences (NAs). The Boards regional orientation and multidisciplinary char- Marine Antarctic Systems and Stocks (BIOMASS), endorsed by acter involve it in a wide range of studies in the physical and the Antarctic Treaty nations and the Intergovernmental Ocean- life sciences, as well as in environmental matters. -

General Agreement on Tariffs and Trade
RESTRICTED ADP/W/42/Add.l GENERAL AGREEMENT ON 25 October 1982 TARIFFS AND TRADE Special Distribution *• See bound volume for :.:.^ Committee on Anti-Dumping Practices for mÉàÊÙkat+d to this document. BACKGROUND INFORMATION FOR ANNUAL REVIEW OF THE OPERATION OF THE AGREEMENT Note by the Secretariat Addendum Attached' is the Summary of Anti-Dumping Actions taken within the period 1 July 1980-30 June 1981 and 1 July 1981-30 June 1982. The late submission of several semi-annual reports and the lack of more detailed information made impossible more comprehensive analysis of the developments in this field. However some preliminary conclusions can be drawn. 1. There has been some increase in the number of anti-dumping actions in 1981/1982 as compared with 1980/1981: (a) Initiations: 1980/1981 - 71 (7)1 1981/1982 - 156 (19) (b) Provisional measures: 1980/1981 - 39 (2) 1981/1982 - 41 (8) (c) Definite duties: 1980/1981 - 24 (-) 1981/1982 - 60 (6) (d) Price undertakings: 1980/1981 - 11 (1) 1981/1982 - 18 (1) 2. Actions J:aken by the three most active Parties (Canada, EEC and the United States ) in the anti-dumping field affect (at least in the quantitative sense) mainly other developed Parties. It does not seem that this conclusion would be modified if the analysis was completed by inclusion of cases which were dismissed or terminated by a negative finding in the course of an investigation. Number in brackets indicate actions affecting developing countries. 2 Australia has not been included in this analysis because insufficient information was available. ANNEX Summary of Anti-Dumping Actions Reporting Reporting Initiation Provisional measures Definite duties P-loe undertaking Outstanding* •o > country period No. -

Robert B. Arnold V. US - 22 July, 1982
Appeal No. 2280 - Robert B. Arnold v. US - 22 July, 1982. ___________________________________________________ UNITED STATES OF AMERICA UNITED STATES COAST GUARD vs. MERCHANT MARINER'S DOCUMENT NO. Z redacted Issued to: Robert B. Arnold DECISION OF THE COMMANDANT ON APPEAL UNITED STATES COAST GUARD 2280 Robert B. Arnold This appeal has been taken in accordance with Title 46 U.S.C. 239(g) and 46 CFR 5.30-1. By order dated 18 September 1981, an Administrative Law Judge of the United States Coast Guard at Long Beach, California, revoked Appellant's seaman's documents upon finding him guilty of misconduct and physical incompetence. The specifications found proved alleged that Appellant while serving as crew messman aboard the SS AUSTRAL LIGHTING, under authority of the captioned document, (1) did on or about 6 June 1981 fail to perform his assigned duties, by not serving breakfast; (2) did on or about 10 June 1981 while the vessel was in Sydney, Australia, fail to perform his duties, by not serving supper; (3) did on or about 10 June 1981 while the vessel was in Sydney, Australia fail to join for the continued voyage to Melbourne, Australia; (4) did on or about 20 June 1981, fail to perform his duties for reasons of intoxication; (5) did on or about 21 June 1981, fail to perform his duties for reasons of intoxication; (6) did on or about 22 June 1981 while vessel was in Brisbane, Australia, fail to join for the continued voyage to San Francisco, California; (7) was on or about 21 June 1981 while the vessel was in port at Brisbane, Australia, and at the time of the hearing was, physically incompetent to perform the file:////hqsms-lawdb/users/KnowledgeManagementD...20&%20R%202280%20-%202579/2280%20-%20ARNOLD.htm (1 of 7) [02/10/2011 8:20:14 AM] Appeal No. -

The New York Patent Law Association
THE NEW YORK PATENT LAW ASSOCIATION VOLUME 20 MAY-JUNE,1981 NUMBER 8 New York Patent Law Association NYPLA Golf and Dinner Outing Continuing Legal Education a Success Weekend Seminar In The Catskills Our Association held its Annual Golf and Dinner Outing on Friday, May 8, 1981, at the Westchester Coun Concord Resort Hotel try Club. Nov. 13,14 and 15,1981 Thirty "golfers" tead off Wlder perfectly blue skies and The Association is planning to hold a Continuing Legal beautiful weather conditions, and nearly one hWldred at Education Weekend Seminar in the Catskills at the Con tended the dinner during which prizes were awarded to the cord Resort Hotel on Friday, Saturday and SWlday, winners. November 13, 14 and 15, 1981. Bob Pollock won the low gross with a score of 82 fol The program will include seminars on the implementa lowed by Albert Robin with 83. tion of the new Patent Office Rules, and on Recent The winner of the net score was David Just with a score of I?evelopments in Patent and Trademark Law and Litiga 94 for a net of 63. tion. Several lovely ladies were among the golfers and each Since accommodations will be limited, all those in was awarded a prize. terested in attending should tear off and return the en Everyone had a most enjoyable day. closed registration form with the registration fee as soon as possible. Yearbook Address Changes All members are urged to check their addresses in the Inventor Of The Year - 1981 1980-81 NYPLA Yearbook and if a correction or change is The Inventor of the Year - 1981 award is to be pre in order, notify Richard G. -

Country Term # of Terms Total Years on the Council Presidencies # Of
Country Term # of Total Presidencies # of terms years on Presidencies the Council Elected Members Algeria 3 6 4 2004 - 2005 December 2004 1 1988 - 1989 May 1988, August 1989 2 1968 - 1969 July 1968 1 Angola 2 4 2 2015 – 2016 March 2016 1 2003 - 2004 November 2003 1 Argentina 9 18 15 2013 - 2014 August 2013, October 2014 2 2005 - 2006 January 2005, March 2006 2 1999 - 2000 February 2000 1 1994 - 1995 January 1995 1 1987 - 1988 March 1987, June 1988 2 1971 - 1972 March 1971, July 1972 2 1966 - 1967 January 1967 1 1959 - 1960 May 1959, April 1960 2 1948 - 1949 November 1948, November 1949 2 Australia 5 10 10 2013 - 2014 September 2013, November 2014 2 1985 - 1986 November 1985 1 1973 - 1974 October 1973, December 1974 2 1956 - 1957 June 1956, June 1957 2 1946 - 1947 February 1946, January 1947, December 1947 3 Austria 3 6 4 2009 - 2010 November 2009 1 1991 - 1992 March 1991, May 1992 2 1973 - 1974 November 1973 1 Azerbaijan 1 2 2 2012 - 2013 May 2012, October 2013 2 Bahrain 1 2 1 1998 - 1999 December 1998 1 Bangladesh 2 4 3 2000 - 2001 March 2000, June 2001 2 Country Term # of Total Presidencies # of terms years on Presidencies the Council 1979 - 1980 October 1979 1 Belarus1 1 2 1 1974 - 1975 January 1975 1 Belgium 5 10 11 2007 - 2008 June 2007, August 2008 2 1991 - 1992 April 1991, June 1992 2 1971 - 1972 April 1971, August 1972 2 1955 - 1956 July 1955, July 1956 2 1947 - 1948 February 1947, January 1948, December 1948 3 Benin 2 4 3 2004 - 2005 February 2005 1 1976 - 1977 March 1976, May 1977 2 Bolivia 3 6 7 2017 - 2018 June 2017, October -

ECONOMIC COMMISSION-FOR LATIN AMERICA Office for the Caribbean
ECONOMIC COMMISSION-FOR LATIN AMERICA Office for the Caribbean Work-Programme 1979-1981 1 July 1979 - 31 July 1981 Work Programme 1979-1981 1 July 1979 - 31 July 1981 Divisions Economic co-operation and integration Priority Areass 1. Removal of language barriers 2. Caribbean Documentation Centre 1» Name of Pro.ject; Removal of language barriers Objective; Facilitate intercourse and closer relations among all countries in sub-region Durations 1/7/79 - 30/6/81 Resources; a) Professional staff m/m Hamid Mohammed 4 b) Consultancy (UNESCO) US$ Co-ordinations - UNESCO Output; Regional workshop on modern approaches to the teaching of foreign languages» National workshops on teaching foreign languages. 2. Name of Projects Establishment of Caribbean Documentation Centre - Caribbean information system in selected sectors viz., agriculture, economic and social planning, and science and technology. Objectives The establishment of regional information networks and the strengthening of national information systems will support the programmes of economic and social development in the sub-region and avoid costly duplication of efforts. Durations 1/7/79 - 30/6/81 Resources s m/m a) Professional staff Hamid Mohammed b) Librarian Assistants 48 c) Travel US$3,000 d) Consultancy (iDRC) US$90,000 - 2 - Co-ordinations - CEPAL, Santiago UNESCO IDRC CARICOM OutputI Establishment of regional information systems. CEPAL Office for the Caribbean Work Programme 1979-1981 1 July 1979 - 51 July 1981 Division; Agriculture Priority Areas; 1) Balance sheets of selected agricultural products 2) Sub-regional co-operation in agriculture lo Name of Pro.ject; Publication of agricultural statistics of Caribbean countries Objective; Provide analytical data to assist countries in the sub-region to consider possibilities for expanding supply of foodstuffs and of agricultural, fishing, and forestry raw materials. -

June 02, 1981 Letter by the President of the Socialist International, Brandt
Digital Archive digitalarchive.wilsoncenter.org International History Declassified June 02, 1981 Letter by the President of the Socialist International, Brandt, to the Chairman of the Committee of the SI for Defence of the Revolution in Nicaragua, González Citation: “Letter by the President of the Socialist International, Brandt, to the Chairman of the Committee of the SI for Defence of the Revolution in Nicaragua, González,” June 02, 1981, History and Public Policy Program Digital Archive, Friedrich Ebert Foundation, Archives of Social Democracy, Willy Brandt Archive, A 11.15, 21. Published in: Berliner Ausgabe, vol. 8. English translation: Dwight E. Langston. Included in CWIHP e-Dossier #22. http://digitalarchive.wilsoncenter.org/document/112717 Summary: Willy Brandt's letter is about the establishment of the Nicaragua solidarity committee, which took place in Madrid in 1981. Brandt states the importance of the new rule of law in Nicaragua and concerns on Socialist International's involvement in the country. Original Language: German Contents: English Translation Scan of Original Document No. 8 Letter by the President of the SI, Brandt, to the Chairman of the “Committee of the SI for Defence of the Revolution in Nicaragua”, González 2 June 1981 AdsD, WBA, A 11.15, 21. Published in: Berliner Ausgabe, vol. 8 English translation: Dwight E. Langston Dear Felipe, With the establishment of the Nicaragua solidarity committee, which took place in Madrid, the Socialist International has obligated itself, within the scope of the capabilities of our association, to defend developments in Nicaragua from external infringements and influences.1 We have tried to express clearly our hopes, but also some misgivings, on the occasion of the first meeting of this committee in early December 1980 in Washington.2 Today we are faced with the question of whether much of what we wanted in Madrid, and reaffirmed in Washington, is still shared to the same degree by our friends in Nicaragua. -
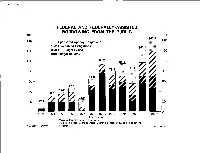
BORROWING from the PUBLIC $Bil
FEDERAL AND FEDERALLY-ASSISTED BORROWING FROM THE PUBLIC $Bil. $Bil. 40.5 140 140 IS11 Sponsored Agency Obligations V//A Guaranteed Obligations^ 124.4 120 Y//A Off-Budget Deficit 120 WM Budget Deficit1 100 100 80 80 60 60 47.5 40.0 40 40 33.5 24.5 20 17.9 20 0 0 1970 1971 1972 1973 1974 1975 1976 1977 1978 1979 1980 1981e Fiscal Years ±1 Adjusted for other means of financing. 2/ Adjusted for federal and sponsored agency purchases of guaranteed obligations. Ofiice of the Secretary of the Treasury Office of Government Financing e estimate April 28, 1981 16 TREASURY FINANCING REQUIREMENTS January - March 1981 $Bil. $Bil. Uses Sources 60 57Va 60 Redemptions of Special Issues ^1% t| l_| 13/4 Gov't Account Sales 50 Coupon 50 Coupon Maturities | Refundings Savings Bonds 40 40 Va Other Nonmarketables 30 30 Net Market ^ 20 4 Cash Deficit Borrowing " 20 10 10 Decrease in Cash Balance 1V2fr 0 0 u Includes maturing marketable securities of $1/2 billion. Office of the Secretary of the Treasury April 28, 1981-18 Office of Government Financing TREASURY FINANCING REQUIREMENTS April - June 1981 $Bil. $Bil. USES SOURCES 313/4 30 30 Government Account ^Special Issues Investment 20 20 Coupon ±\ a Coupon Maturities t • Refunding 10 Savings 10 Bonds 3/4^1 Net Cash |^11/4 Other Non- T marketables Paydown|^| Cash Surplus^ 4 Increase in Cash Balance^ 0' 0 -V Assumes $15 billion June 30, 1981 cash balance. Office of the Secretary of the Treasury Office of Government Financing April 28,1981-21 NET MARKET BORROWING April - June 1981 Total -2 Cash Management Bills: April Issues 6 April Retirements -16 June Maturities -4 Net Borrowing -14 Other Net Borrowing: 12 Done^ 20 year - 1 month bond 13/4 7 year note 3 2 year note 172 Regular bills Va Total 6Y2 To Be Done SV2 JV Issued or announced through April 24, 1981. -

Appeal No. 2251 - Hassen M
Appeal No. 2251 - Hassen M. Fadl v. US - 10 June, 1981. ________________________________________________ UNITED STATES OF AMERICA UNITED STATES COAST GUARD vs. MERCHANT MARINER'S DOCUMENT Issued to: Hassen M. Fadl Z-1192982 DECISION OF THE COMMANDANT ON APPEAL UNITED STATES COAST GUARD 2251 Hassen M. Fadl This appeal has been taken in accordance with Title 46 U.S.C. 239(g) and 46 CFR 5.30-1. By order dated 31 July 1980, an Administrative Law Judge of the United States Coast Guard at New York, New York, revoked Appellant's seaman's document upon finding him guilty of the charge of "conviction for a narcotic drug law violation." The one specification found proved alleges that while holder of the document above captioned, on or about 5 August 1970, Appellant was convicted by the Criminal Court of the City of New York, County of New York, a court of record, for violation of Section 220.05 of the Penal Law of the State of New York, for criminal possession of a dangerous drug, to wit; Hashish. The hearing was held at New York, New York, on 25 July 1980. Appellant did not appear and was not represented at the hearing, which was held in absentia. The Investigating Officer introduced in evidence two documents. Subsequent to the hearing, the Administrative Law Judge file:////hqsms-lawdb/users/KnowledgeManagementD...S%20&%20R%201980%20-%202279/2251%20-%20FADL.htm (1 of 3) [02/10/2011 9:59:23 AM] Appeal No. 2251 - Hassen M. Fadl v. US - 10 June, 1981. entered a written decision in which he concluded that the charge and the specification had been proved. -

Pan American Health Organization World Health
directing council regional committee PAN AMERICAN WORLD HEALTH HEALTH ORGANIZATION ORGANIZATION XXVIII Meeting XXXIII Meeting Washington, D.C. September-October 1981 INDEXED' I - - - I - II __ I - Provisional Agenda Item 19 CD28/23 (Eng.) 27 July 1981 ORIGINAL: ENGLISH REPORT ON THE COLLECTION OF QUOTA CONTRIBUTIONS The Director has the honor to present, in Schedule A (Annex I) a report on the status of quota contributions as of 4 June 1981, as submitted to the 86th Meeting of the Executive Committee. In the Interim Financial Report of the Director for the Year 1980 (Official Document 175 and 175-A) there is presented a table showing the status of quota contributions as of 31 December 1980. In 1979 the XXVI Meeting of the Directing Council, by Resolution XXVIII, approved a supplementary budget for the financing of the Pan American Foot-and-Mouth Disease Center and the Pan American Zoonoses Center. The status as of 4 June 1981 of the quota contributions for the supplementary budget is presented as Schedule B (Annex II). To provide the Council with the latest information, an updated status report will be issued on 11 September. The Executive Committee at its 86th Meeting considered the status of quota contributions and approved Resolution VI, which reads as follows: THE EXECUTIVE COMMITTEE, Having considered the report of the Director on the collection of quota contributions (Document CE86/27 and ADD. I); Noting that, of the three countries with approved payment plans for liquidating their arrears, one had made a payment by the time of the Executive Committee Meeting; Considering the importance of prompt and full payment of quota contributions to assure the financing of the authorized program and budget and to maintain the Organization in a sound financial position; and CD28/23 (Eng.) Page 2 Bearing in mind the provisions of Article 6.B of the Constitution of PAHO relating to the suspension of voting privileges of Governments failing to meet their financial obligations, RESOLVES: 1.