Endoscopic Sinus Surgery: Role of the Radiologist
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gross Anatomy Assignment Name: Olorunfemi Peace Toluwalase Matric No: 17/Mhs01/257 Dept: Mbbs Course: Gross Anatomy of Head and Neck
GROSS ANATOMY ASSIGNMENT NAME: OLORUNFEMI PEACE TOLUWALASE MATRIC NO: 17/MHS01/257 DEPT: MBBS COURSE: GROSS ANATOMY OF HEAD AND NECK QUESTION 1 Write an essay on the carvernous sinus. The cavernous sinuses are one of several drainage pathways for the brain that sits in the middle. In addition to receiving venous drainage from the brain, it also receives tributaries from parts of the face. STRUCTURE ➢ The cavernous sinuses are 1 cm wide cavities that extend a distance of 2 cm from the most posterior aspect of the orbit to the petrous part of the temporal bone. ➢ They are bilaterally paired collections of venous plexuses that sit on either side of the sphenoid bone. ➢ Although they are not truly trabeculated cavities like the corpora cavernosa of the penis, the numerous plexuses, however, give the cavities their characteristic sponge-like appearance. ➢ The cavernous sinus is roofed by an inner layer of dura matter that continues with the diaphragma sellae that covers the superior part of the pituitary gland. The roof of the sinus also has several other attachments. ➢ Anteriorly, it attaches to the anterior and middle clinoid processes, posteriorly it attaches to the tentorium (at its attachment to the posterior clinoid process). Part of the periosteum of the greater wing of the sphenoid bone forms the floor of the sinus. ➢ The body of the sphenoid acts as the medial wall of the sinus while the lateral wall is formed from the visceral part of the dura mater. CONTENTS The cavernous sinus contains the internal carotid artery and several cranial nerves. Abducens nerve (CN VI) traverses the sinus lateral to the internal carotid artery. -

Maxillary Sinus (Antrum of Higmore)
Maxillary Sinus (Antrum of Higmore) The maxillary sinus is a pneumatic space. It is the largest bilateral air sinus located in the body of the maxilla and opens in the middle nasal meatus of the nasal cavity with single or multiple openings. Development: The maxillary sinuses are the only sizable sinuses present at birth. At birth they have the size of a small lima bean measuring about 8X4 mm, and are situated with their longer dimension directed anteriorly and posteriorly. They develop at the third month of intrauterine life, in the place existing between the oral cavity and the floor of the orbit. They develop as evagination of the mucous membrane of the lateral wall of the nasal cavity at the level of the middle nasal meatus forming a minute space that expands primarily in an inferior direction into the primordium of the maxilla. The maxillary sinus enlarges variably and greatly by pneumatization until it reaches the adult size by the eruption of the permanent teeth. Enlargement of the maxillary sinus is consequent to facial growth. Growth of the sinus slows down with decline of facial growth during puberty but continues throughout life. Anatomy: The maxillary sinus varies greatly in size, shape and position not only in different individuals but also in different sides of the same individual. It is pyramidal in shape having a base, an apex and four walls: The base: lateral wall of the nasal cavity. The apex: directed laterally towards the zygomatic process of the maxilla. The four walls: Anterior wall: facial surface of the maxilla. -

Normal and Abnormal Findings in Rhinoscopy
3/18/2016 Normal and Abnormal Findings in Rhinoscopy Brian C. Spector, MD Ear, Nose Throat and Plastic Surgery Associates Assistant Professor FSU College of Medicine Assistant Professor UCF College of Medicine Sixth Annual ENT for the PA-C | March 30 – April 3, 2016| Orlando, FL No Disclosures Sixth Annual ENT for the PA-C | March 30 – April 3, 2016| Orlando, FL Learning Objectives • Maximize diagnostic yield by understanding best technique for Rhinoscopy • Identify normal anatomy and variants of normal anatomy visualized in Rhinoscopy • Identify abnormal findings visualized in Rhinoscopy Sixth Annual ENT for the PA-C | March 30 – April 3, 2016| Orlando, FL 1 3/18/2016 Sixth Annual ENT for the PA-C | March 30 – April 3, 2016| Orlando, FL Nasal Septum Lateral Nasal Wall Sixth Annual ENT for the PA-C | March 30 – April 3, 2016| Orlando, FL 2 3/18/2016 Nasopharynx Mucosa Intact Sixth Annual ENT for the PA-C | March 30 – April 3, 2016| Orlando, FL Ehab Zayyan MD, PhD Anterior Rhinoscopy Non Dominant Hand. Index Finger on Nasal Tip. Keep open until fully removed to avoid pulling hairs. Headlight Illumination Nasal Septum: deviation, perforation, stigmata of recent or active bleeding Inferior Turbinates: color of mucosa, congestion, secretions Internal Nasal Valve ‐ Septum, floor, caudal border of upper lateral cartilage, anterior head of inferior turbinate. Narrowest part of nasal airway Middle Turbinates Mucosa Sixth Annual ENT for the PA-C | March 30 – April 3, 2016| Orlando, FL 3 3/18/2016 Nasal Endoscopy Flexible Nasal Endoscopy: Technique -

Surgical Anatamic of Paranasal Sinuses
SURGICAL ANATAMIC OF PARANASAL SINUSES DR. SEEMA MONGA ASSOCIATE PROFESSOR DEPARTMENT OF ENT-HNS HIMSR MIDDLE TURBINATE 1. Anterior attachment : vertically oriented, sup to the lateral border of cribriform plate. 2. Second attachment :Obliquely oriented- basal lamella/ ground lamella, Attached to the lamina papyracea ( medial wall of orbit anterior, posterior air cells, sphenopala‐ tine foramen 3. Posterior attachment :medial wall of maxillary sinus, horizontally oriented. , supreme turbinate 3. Occasionally 4. fourth turbinate, 5. supreme meatus, if present 6. drains posterior ethmoid drains inferior, middle, superior turbinates and, occasionally, the supreme turbinate, the fourth turbinate. e. Lateral to these turbinates are the corresponding meatuses divided per their drainage systems ANATOMICAL VARIATIONS OF THE TURBINATES 1. Concha bullosa, 24–55%, often bilateral, 2. Interlamellar cell of grunwald: pneumatization is limited to the vertical part of middle turbinate, usually not causing narrowing of the ostiomeatal unit 3. Paradoxic middle turbinate: 26%,. Occasionally, it can affect the patency of the ostiomeatal unit 4. Pneumatized basal lamella, falsely considered, posterior ethmoid air cell Missed basal lamella – attaches to lateral maxillary sinus wall Ostiomeatal unit Anterior ostiomeatal unit, maxillary, anterior ethmoid, frontal sinuses, (1) ethmoid infundibulum, (2) middle meatus, (3) hiatus semilunaris, (4) maxillaryOstium, (5) ethmoid bulla, (6) frontal recess, (7) uncinate process. , sphenoethmoidal recess Other draining osteomeatal unit, posterior in the nasal cavity, posterior ethmoid sinus, lateral to the superior turbinate, . sphenoid Sinus medial to the superior turbinate Uncinate Process Crescent‐shaped, thin individual bone inferiorly- ethmoidal process of inferior turbinate, anterior, lacrimal bone, posteriorly- hiatus Semilunaris, medial -ethmoid infundibulum, laterally, middle meatus superior attachment- variability, direct effect on frontal sinus drainage pathway. -

Download PDF (Inglês)
Braz J Otorhinolaryngol. 2015;81(1 Supl. 1):S1-S49 Brazilian Journal of OTORHINOLARYNGOLOGY www.bjorl.org CONSENSUS Rhinosinusitis: evidence and experience October 18 and 19, 2013 - São Paulo Coordination Although VAS has only been validated for CRS in adults, Wilma T. Anselmo-Lima e Eulalia Sakano the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) 20121 also recommends its use in ARS. There are sev- Participants eral specific questionnaires for rhinosinusitis, but in practice, 2-4 André Alencar, Atílio Fernandes, Edwin Tamashiro, most have limited application, particularly in acute cases. Elizabeth Araújo, Érica Ortiz, Fabiana Cardoso Pereira Valera, Fábio Pinna, Fabrizio Romano, Francini Padua, João Mello Jr., Acute rhinosinusitis João Teles Jr., José E. L. Dolci, Leonardo Balsalobre, Macoto Kosugi, Marcelo H. Sampaio, Márcio Nakanishi, Definition Marco César, Nilvano Andrade, Olavo Mion, Otávio Piltcher, Reginaldo Fujita, Renato Roithmann, Richard Voegels, ARS is an inflammatory process of the nasal mucosa of sud- Roberto E. Guimarães, Roberto Meireles, Shirley Pignatari, Victor Nakajima den onset, lasting up to 12 weeks. It may occur one or more times in a given period of time, but always with complete For the purpose of citation remission of signs and symptoms between episodes. Wilma Terezinha Anselmo Lima, Eulalia Sakano, Edwin Tamashiro, Elizabeth Araújo, Érica Ortiz, Fábio Pinna, Fabrizio Romano, Francini Padua, João Mello Jr., João Teles Jr., José E. L. Dolci, Classification Leonardo Balsalobre, Macoto Kosugi, Marcelo H. Sampaio, Márcio Nakanishi, Marco César, Nilvano Andrade, Olavo Mion, There are several classifications for RS. One of the most Otávio Piltcher, Reginaldo Fujita, Renato Roithmann, often used is the etiological classification, which is based Richard Voegels, Roberto E. -

Macroscopic Anatomy of the Nasal Cavity and Paranasal Sinuses of the Domestic Pig (Sus Scrofa Domestica) Daniel John Hillmann Iowa State University
Iowa State University Capstones, Theses and Retrospective Theses and Dissertations Dissertations 1971 Macroscopic anatomy of the nasal cavity and paranasal sinuses of the domestic pig (Sus scrofa domestica) Daniel John Hillmann Iowa State University Follow this and additional works at: https://lib.dr.iastate.edu/rtd Part of the Animal Structures Commons, and the Veterinary Anatomy Commons Recommended Citation Hillmann, Daniel John, "Macroscopic anatomy of the nasal cavity and paranasal sinuses of the domestic pig (Sus scrofa domestica)" (1971). Retrospective Theses and Dissertations. 4460. https://lib.dr.iastate.edu/rtd/4460 This Dissertation is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Retrospective Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected]. 72-5208 HILLMANN, Daniel John, 1938- MACROSCOPIC ANATOMY OF THE NASAL CAVITY AND PARANASAL SINUSES OF THE DOMESTIC PIG (SUS SCROFA DOMESTICA). Iowa State University, Ph.D., 1971 Anatomy I University Microfilms, A XEROX Company, Ann Arbor. Michigan I , THIS DISSERTATION HAS BEEN MICROFILMED EXACTLY AS RECEIVED Macroscopic anatomy of the nasal cavity and paranasal sinuses of the domestic pig (Sus scrofa domestica) by Daniel John Hillmann A Dissertation Submitted to the Graduate Faculty in Partial Fulfillment of The Requirements for the Degree of DOCTOR OF PHILOSOPHY Major Subject: Veterinary Anatomy Approved: Signature was redacted for privacy. h Charge of -^lajoï^ Wor Signature was redacted for privacy. For/the Major Department For the Graduate College Iowa State University Ames/ Iowa 19 71 PLEASE NOTE: Some Pages have indistinct print. -

CT of Perineural Tumor Extension: Pterygopalatine Fossa
731 CT of Perineural Tumor Extension: Pterygopalatine Fossa Hugh D. Curtin1.2 Tumors of the oral cavity and paranasal sinuses can spread along nerves to areas Richard Williams 1 apparently removed from the primary tumor. In tumors of the palate, sinuses, and face, Jonas Johnson3 this "perineural" spread usually involves the maxillary division of the trigeminal nerve. The pterygopalatine fossa is a pathway of the maxillary nerve and becomes a key landmark in the detection of neural metastasis by computed tomogaphy (CT). Oblitera tion of the fat in the fossa suggests pathology. Case material illustrating neural extension is presented and the CT findings are described. Perineural extension is possibly the most insidious form of tumor spread of head and neck malignancy. After invading a nerve, tumor follows the sheath to reach the deeper connections of the nerve, escaping the area of a planned resection. Thus, detection of this form of extension is important in treatment planning and estimation of prognosis. The pterygopalatine fossa (PPF) is a key crossroad in extension along cranial nerve V. The second branch of the trigeminal nerve passes from the gasserian ganglion through the foramen rotundum into the PPF. Here the nerve branches send communications to the palate, sinus, nasal cavity, and face. Tumor can follow any of these routes proximally into the PPF and eventually to the gasserian ganglion in the middle cranial fossa. The PPF contains enough fat to be an ideal subject for computed tomographic (CT) evaluation. Obliteration of this fat is an important indicator of pathology, including perineural tumor spread. Other signs of perineural extension include enlargement of foramina, increased enhancement in the region of Meckel cave (gasserian ganglion), and atrophy of the muscles innervated by the trigeminal nerve. -

MBB: Head & Neck Anatomy
MBB: Head & Neck Anatomy Skull Osteology • This is a comprehensive guide of all the skull features you must know by the practical exam. • Many of these structures will be presented multiple times during upcoming labs. • This PowerPoint Handout is the resource you will use during lab when you have access to skulls. Mind, Brain & Behavior 2021 Osteology of the Skull Slide Title Slide Number Slide Title Slide Number Ethmoid Slide 3 Paranasal Sinuses Slide 19 Vomer, Nasal Bone, and Inferior Turbinate (Concha) Slide4 Paranasal Sinus Imaging Slide 20 Lacrimal and Palatine Bones Slide 5 Paranasal Sinus Imaging (Sagittal Section) Slide 21 Zygomatic Bone Slide 6 Skull Sutures Slide 22 Frontal Bone Slide 7 Foramen RevieW Slide 23 Mandible Slide 8 Skull Subdivisions Slide 24 Maxilla Slide 9 Sphenoid Bone Slide 10 Skull Subdivisions: Viscerocranium Slide 25 Temporal Bone Slide 11 Skull Subdivisions: Neurocranium Slide 26 Temporal Bone (Continued) Slide 12 Cranial Base: Cranial Fossae Slide 27 Temporal Bone (Middle Ear Cavity and Facial Canal) Slide 13 Skull Development: Intramembranous vs Endochondral Slide 28 Occipital Bone Slide 14 Ossification Structures/Spaces Formed by More Than One Bone Slide 15 Intramembranous Ossification: Fontanelles Slide 29 Structures/Apertures Formed by More Than One Bone Slide 16 Intramembranous Ossification: Craniosynostosis Slide 30 Nasal Septum Slide 17 Endochondral Ossification Slide 31 Infratemporal Fossa & Pterygopalatine Fossa Slide 18 Achondroplasia and Skull Growth Slide 32 Ethmoid • Cribriform plate/foramina -

Anatomic Variations of Paranasal Sinus on Multidetector Computed Tomography Examinations for Functional Endoscopic Sinus Surgery
MÜSBED 2013;3(2):102-106 DOI: 10.5455/musbed.20130410100848 Derleme / Review Anatomic Variations of Paranasal Sinus on Multidetector Computed Tomography Examinations for Functional Endoscopic Sinus Surgery Filiz Namdar Pekiner Department of Oral Diagnosis and Radiology, Faculty of Dentistry, Marmara University, Istanbul - Turkey Ya zış ma Ad re si / Add ress rep rint re qu ests to: Filiz Namdar Pekiner, Marmara University, Faculty of Dentistry, Department of Oral Diagnosis and Radiology, Nisantasi, Istanbul - Turkey Elekt ro nik pos ta ad re si / E-ma il add ress: [email protected] Ka bul ta ri hi / Da te of ac cep tan ce: 10 Nisan 2013 / April 10, 2013 ÖZET ABS TRACT Fonksiyonel endoskopik sinüs cerrahisinde mul- Anatomic variations of paranasal sinus tidetektör bilgisayarlı tomografide paranasal on multidetector computed tomography sinüslerin anatomik varyasyonları examinations for functional endoscopic sinus surgery Bilgisayarlı tomografi paranasal sinüslerin hastalıklarının ve fonksiyo- nel endoskopik sinüs cerrahisi ile tedavilerinin değerlendirilmesinde Computed tomography is excellent means of providing anatomical anatomik olarak sağladığı bilgi oldukça önemlidir. Paranasal sinüs- information of paranasal sinuses, assessing disease and guiding lerde izlenen anatomik varyasyonlar nadir değildir. Bu makalenin treatment with functional endoscopic sinus surgery (FESS). Common amacı paranasal sinüslerde izlenebilen bazı anatomik varyasyonları anatomical variations are not rare in the paranasal sinuses. The aim of sunmaktır. this article was presented radiological characteristics of some anatomic Anahtar sözcükler: Paranasal sinüsler, anatomik varyasyonlar, bilgi- variation in paranasal sinuses. sayarlı tomografi, fonksiyonel endoskopik sinüs cerrahisi Key words: Paranasal sinus, anatomical variation, computed tomography, functional endoscopic sinus surgery INTRODUCTION anatomy as shown on CT are of potential significance, it may predispose to certain pathologic conditions and Functional endoscopic sinus surgery (FESS) has been diseases (5). -

Dissertation on an OBSERVATIONAL STUDY COMPARING the EFFECT of SPHENOPALATINE ARTERY BLOCK on BLEEDING in ENDOSCOPIC SINUS SURGE
Dissertation On AN OBSERVATIONAL STUDY COMPARING THE EFFECT OF SPHENOPALATINE ARTERY BLOCK ON BLEEDING IN ENDOSCOPIC SINUS SURGERY Dissertation submitted to TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI For M.S.BRANCH IV (OTORHINOLARYNGOLOGY) Under the guidance of DR. F ANTHONY IRUDHAYARAJAN, M.S., D.L.O Professor & HOD, Department of ENT & Head and Neck Surgery, Govt. Stanley Medical College, Chennai. GOVERNMENT STANLEY MEDICAL COLLEGE THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY, CHENNAI-32, TAMILNADU APRIL 2017 CERTIFICATE This is to certify that this dissertation titled AN OBSERVATIONAL STUDY COMPARING THE EFFECT OF SPHENOPALATINE ARTERY BLOCK ON BLEEDING IN ENDOSCOPIC SINUS SURGERY is the original and bonafide work done by Dr. NIGIL SREEDHARAN under the guidance of Prof Dr F ANTHONY IRUDHAYARAJAN, M.S., DLO Professor & HOD, Department of ENT & Head and Neck Surgery at the Government Stanley Medical College & Hospital, Chennai – 600 001, during the tenure of his course in M.S. ENT from July-2014 to April- 2017 held under the regulation of the Tamilnadu Dr. M.G.R Medical University, Guindy, Chennai – 600 032. Prof Dr F Anthony Irudhayarajan, M.S., DLO Place : Chennai Professor & HOD, Date : .10.2016 Department of ENT & Head and Neck Surgery Government Stanley Medical College & Hospital, Chennai – 600 001. Dr. Isaac Christian Moses M.D, FICP, FACP Place: Chennai Dean, Date : .10.2016 Govt.Stanley Medical College, Chennai – 600 001. CERTIFICATE BY THE GUIDE This is to certify that this dissertation titled “AN OBSERVATIONAL STUDY COMPARING THE EFFECT OF SPHENOPALATINE ARTERY BLOCK ON BLEEDING IN ENDOSCOPIC SINUS SURGERY” is the original and bonafide work done by Dr NIGIL SREEDHARAN under my guidance and supervision at the Government Stanley Medical College & Hospital, Chennai – 600001, during the tenure of his course in M.S. -
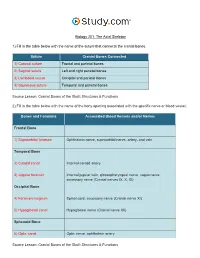
The Axial Skeleton Visual Worksheet
Biology 201: The Axial Skeleton 1) Fill in the table below with the name of the suture that connects the cranial bones. Suture Cranial Bones Connected 1) Coronal suture Frontal and parietal bones 2) Sagittal suture Left and right parietal bones 3) Lambdoid suture Occipital and parietal bones 4) Squamous suture Temporal and parietal bones Source Lesson: Cranial Bones of the Skull: Structures & Functions 2) Fill in the table below with the name of the bony opening associated with the specific nerve or blood vessel. Bones and Foramina Associated Blood Vessels and/or Nerves Frontal Bone 1) Supraorbital foramen Ophthalmic nerve, supraorbital nerve, artery, and vein Temporal Bone 2) Carotid canal Internal carotid artery 3) Jugular foramen Internal jugular vein, glossopharyngeal nerve, vagus nerve, accessory nerve (Cranial nerves IX, X, XI) Occipital Bone 4) Foramen magnum Spinal cord, accessory nerve (Cranial nerve XI) 5) Hypoglossal canal Hypoglossal nerve (Cranial nerve XII) Sphenoid Bone 6) Optic canal Optic nerve, ophthalmic artery Source Lesson: Cranial Bones of the Skull: Structures & Functions 3) Label the anterior view of the skull below with its correct feature. Frontal bone Palatine bone Ethmoid bone Nasal septum: Perpendicular plate of ethmoid bone Sphenoid bone Inferior orbital fissure Inferior nasal concha Maxilla Orbit Vomer bone Supraorbital margin Alveolar process of maxilla Middle nasal concha Inferior nasal concha Coronal suture Mandible Glabella Mental foramen Nasal bone Parietal bone Supraorbital foramen Orbital canal Temporal bone Lacrimal bone Orbit Alveolar process of mandible Superior orbital fissure Zygomatic bone Infraorbital foramen Source Lesson: Facial Bones of the Skull: Structures & Functions 4) Label the right lateral view of the skull below with its correct feature. -
![NASAL CAVITY and PARANASAL SINUSES, PTERYGOPALATINE FOSSA, and ORAL CAVITY (Grant's Dissector [16Th Ed.] Pp](https://docslib.b-cdn.net/cover/6054/nasal-cavity-and-paranasal-sinuses-pterygopalatine-fossa-and-oral-cavity-grants-dissector-16th-ed-pp-1806054.webp)
NASAL CAVITY and PARANASAL SINUSES, PTERYGOPALATINE FOSSA, and ORAL CAVITY (Grant's Dissector [16Th Ed.] Pp
NASAL CAVITY AND PARANASAL SINUSES, PTERYGOPALATINE FOSSA, AND ORAL CAVITY (Grant's Dissector [16th Ed.] pp. 290-294, 300-303) TODAY’S GOALS (Nasal Cavity and Paranasal Sinuses): 1. Identify the boundaries of the nasal cavity 2. Identify the 3 principal structural components of the nasal septum 3. Identify the conchae, meatuses, and openings of the paranasal sinuses and nasolacrimal duct 4. Identify the openings of the auditory tube and sphenopalatine foramen and the nerve and blood supply to the nasal cavity, palatine tonsil, and soft palate 5. Identify the pterygopalatine fossa, the location of the pterygopalatine ganglion, and understand the distribution of terminal branches of the maxillary artery and nerve to their target areas DISSECTION NOTES: General comments: The nasal cavity is divided into right and left cavities by the nasal septum. The nostril or naris is the entrance to each nasal cavity and each nasal cavity communicates posteriorly with the nasopharynx through a choana or posterior nasal aperture. The roof of the nasal cavity is narrow and is represented by the nasal bone, cribriform plate of the ethmoid, and a portion of the sphenoid. The floor is the hard palate (consisting of the palatine processes of the maxilla and the horizontal portion of the palatine bone). The medial wall is represented by the nasal septum (Dissector p. 292, Fig. 7.69) and the lateral wall consists of the maxilla, lacrimal bone, portions of the ethmoid bone, the inferior nasal concha, and the perpendicular plate of the palatine bone (Dissector p. 291, Fig. 7.67). The conchae, or turbinates, are recognized as “scroll-like” extensions from the lateral wall and increase the surface area over which air travels through the nasal cavity (Dissector p.