Changes in Bengal's Western Frontier
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Magmatic Underplating Beneath the Rajmahal Traps: Gravity Signature and Derived 3-D Configuration
Magmatic underplating beneath the Rajmahal Traps: Gravity signature and derived 3-D configuration A P Singh∗, Niraj Kumar and Bijendra Singh National Geophysical Research Institute, Uppal Road, Hyderabad 500 007, India ∗ e-mail: apsingh−[email protected] [email protected] The early Cretaceous thermal perturbation beneath the eastern continental margin of the Indian shield resulted in the eruption of the Rajmahal Traps. To understand the impact of the magmatic process that originated in the deep mantle on the lower crustal level of the eastern Indian shield and adjoining Bengal basin the conspicuous gravity anomalies observed over the region have been modelled integrating with available geophysical information. The 3-D gravity modelling has delin- 3 eated 10–15 km thick high-density (ρ =3.02 g/cm ) accreted igneous layer at the base of the crust beneath the Rajmahal Traps. Thickness of this layer varies from 16 km to the west of the Rajmahal towards north to about 12 km near Kharagpur towards south and about 18 km to the east of the Raniganj in the central part of the region. The greater thickness of the magmatic body beneath the central part of the region presents itself as the locus of the potential feeder channel for the Rajmahal Traps. It is suggested that the crustal accretion is the imprint of the mantle thermal perturbation, over which the eastern margin of the eastern Indian shield opened around 117 Ma ago. The nosing of the crustal accretion in the down south suggests the possible imprint of the subsequent magmatic intrusion along the plume path. -

Pakur District, Jharkhand State
भूजल सूचना पुस्तिका पाकु र स्जला, झारखंड Ground Water Information Booklet Pakur District, Jharkhand State के न्द्रीय भमू िजल बोड ड Central Ground water Board Ministry of Water Resources जल संसाधन िंत्रालय (Govt. of India) (भारि सरकार) State Unit Office,Ranchi रा煍य एकक कायाडलय, रााँची Mid-Eastern Region िध्य-पूर्वी क्षेत्र Patna पटना मसिंबर 2013 September 2013 1 भूजल सूचना पुस्तिका पाकु र स्जला, झारखंड Ground Water Information Booklet Pakur District, Jharkhand State Prepared By सुनिल टोꥍपो (वैज्ञानिक ख ) Sunil Toppo (Scientist B) रा煍य एकक कायाडलय, रााँची िध्य-पूर्वी क्षेत्र,पटना State Unit Office, Ranchi Mid Eastern Region, Patna 2 GROUND WATER INFORMATION BOOKLET PAKUR DISTRICT, JHARKHAND STATE CONTENTS Chapter Page No. 1.0 Introduction 1 1.1 Administration 1 1.2 River System 1 1.3 Irrigation practices 2 1.4 Studies/ Activities carried out by CGWB 2 2.0 Rainfall & Climate 2 2.1 Rainfall 2 2.2 Climate 2 3.0 Geomorphology & Soil 3 3.1 Geomorphology 3 3.2 Soils 3 4.0 Ground Water Scenario 4 4.1 Hydrogeology 4 4.1.1 Exploratory wells 4 4.1.2 Depth to water level 5 4.1.3 Seasonal Fluctuation 6 4.1.4 Long term water level trend (2002 – 2011) 6 4.2 Ground Water Resources 6 4.3 Ground Water Quality 7 4.4 Status of Ground Water Development 7 5.0 Ground Water Management Strategy 8 5.1 Ground Water Development 8 5.2 Water Conservation & Artificial Recharge 8 6.0 Ground Water related issues and problems 9 7.0 Awareness & Training Activity 9 7.1 Mass Awareness Programme 9 8.0 Area Notified by CGWA/ SGWA 9 9.0 Recommendations 10 3 List of Tables: Table 1 : Administrative division and population of Pakur district. -

JHARKHAND - NOTIFIED PROTECTION OFFICERS (W.E.F
JHARKHAND - NOTIFIED PROTECTION OFFICERS (w.e.f. 11.06.2007) 1. Ms. Hema Choudhary, CDPO, Integrated Child Development Services, Lapung, P.O. Lapung, Ranchi - 835244, Jharkhand. Ph. 9934172154 2. Smt. Abha Choudhary, CDPO, Integrated Child Development Services, Ranchi Sadar, Kanke Road, Apar Shivpuri, Ranchi - 834008, Jhharkhand. Ph. 9431578415 3. Ms. Pushpa Tigga, CDPO, Integrated Child Development Services, Angara, P.O. Angara, Ranchi – 835103, Jharkhand. Ph. 9431118906 4. Ms. Renu Ravi, CDPO, Integrated Child Development Services, Chanho, P.O. Chanho, Ranchi - 835239, Jharkhand. Ph. 9431701597 5. Ms. Jyoti Kumari Prasad CDPO, Integrated Child Development Services Mandar, P.O. Mandar, Ranchi - 835214. Jharkhand Ph. 9130147188 6. Ms. Neeta Kumari Chouhan, ICDPO, Integrated Child Development Services, Khijari, P.O. Namkum, Ranchi – 834010, Jharkhand. Ph. 9431465643 7. Ms. Sudha Sinha, CDPO, Integrated Child Development Services, Bero, P.O. Berro, Ranchi – 835202, Jharkhand. Ph. 9431386449 8. Ms. Nirupama Shankar, CDPO, Integrated Child Development Services, Ratu, P.O. Ratu, Ranchi - 835222, Jharkhand. 9. CDPO, Integrated Child Development Services, Bundu, P.O. Bundu, Ranchi - 835204, Jhharkhand. 10. Ms. Uma Sinha, CDPO, Integrated Child Development Services, Tamar, P.O. Tamar, Ranchi – 835225, Jhharkhand. Ph. 9431312338 11. Ms. Surbhi Singh, CDPO, Integrated Child Development Services, Ormanjhi, P.O. Ormanjhi, Ranchi - 835219, Jharkhand. Ph. 9431165293 12. CDPO, Integrated Child Development Services, Budmu, P.O. Budmu, Ranchi – 835214, Jharkhand. 13. Ms. Pooja Kumari, CDPO, Integrated Child Development Services, Kanke, P.O. Kanke, Ranchi - 834006. Jharkhand Ph. 9431772461 14. Ms. Kanak Kumari Tirki, CDPO, Integrated Child Development Services, Silli, P.O. Silli, Ranchi - 835103, Jharkhand. Ph. 9431325767 15. Ms. Lilavati Singh, CDPO, Integrated Child Development Services, Sonahatu, Post – Sonahatu, Ranchi - 835243, Jharkhand. -

Sahebganj Districts, Jharkhand
कᴂद्रीय भूमि जल बो셍ड जल संसाधन, नदी विकास और गंगा संरक्षण विभाग, जल शक्ति मंत्रालय भारत सरकार Central Ground Water Board Department of Water Resources, River Development and Ganga Rejuvenation, Ministry of Jal Shakti Government of India AQUIFER MAPPING AND MANAGEMENT OF GROUND WATER RESOURCES SAHEBGANJ DISTRICTS, JHARKHAND राज्य एकक कायाालय, रांची State Unit Office, Ranchi भारत सरकार Government of India जऱ स車साधन, नदी विकास एि車 ग車गा स車रक्षण म車त्राऱय Ministry of Water Resources, River Development & Ganga Rejuvenation केन्द्रीय भमू म-जऱ र्बो셍ा Central Ground Water Board PART – I/ भाग -१ Aquifer Maps and Ground Water Management Plan of Sahebganj district, Jharkhand जऱभतृ न啍शे तथा भूजऱ प्रबंधन योजना साहिबगंज जजऱा, झारख赍ड State Unit Office, Ranchi Mid-Eastern Region, Patna March 2019 रा煍य एकक कायााऱय रा車ची मध्य-ऩर्बू ी क्षेत्र ऩटना माचा २०१९ Aquifer Maps and Ground Water Management Plan of Sahebganj district, Jharkhand जऱभतृ न啍शे तथा भूजऱ प्रबंधन योजना साहिबगंज जजऱा, झारख赍ड State Unit Office, Ranchi Mid-Eastern Region, Patna March 2019 रा煍य एकक कायााऱय रा車ची मध्य-ऩर्बू ी क्षेत्र ऩटना माचा २०१९ REPORT ON AQUIFER MAPPING AND MANAGEMENT PLAN (PART – I) OF SAHEBGANJ DISTRICT, JHARKHAND 2017 – 18 CONTRIBUTORS’ Principal Authors Sunil Toppo : Junior Hydrogeologist (Scientist-B) Supervision & Guidance A.K.Agrawal : Regional Director G. K. Roy : Officer-In- Charge T.B.N. Singh : Scientist-D Dr Sudhanshu Shekhar : Scientist-D Hydrogeology, GIS maps and Management Plan Sunil Toppo : Junior Hydrogeologist Dr Anukaran Kujur : Assistant Hydrogeologist Atul Beck : Assistant Hydrogeologist Hydrogeological Data Acquisition and Groundwater Exploration Sunil Toppo : Junior Hydrogeologist Dr Anukaran Kujur : Assistant Hydrogeologist Atul Beck : Assistant Hydrogeologist Geophysics : B. -
![Ftyk Fuokzpu Dk;Kzy;] Lkgscxat](https://docslib.b-cdn.net/cover/2720/ftyk-fuokzpu-dk-kzy-lkgscxat-1372720.webp)
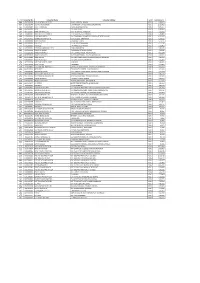
Ftyk Fuokzpu Dk;Kzy;] Lkgscxat
ftyk fuokZpu dk;kZy;] lkgscxat ch0,y0vks0 dh lwph 01& jktegy fo/kku lHkk fuokZpu {ks= AC- Booth Booth Name Name of BLO Mobile No Address NO Number Middle School Hajipur Diyara 1-Vill- Hajipur Diyara, Dist- 1 1 Savita Devi 9939967486 (New Building) Sahibganj Middle School Hajipur Diyara, 2-Vill- Hajipur Diyara, Dist- 1 2 Sangita Devi 9955137519 (Old Building) Sahibganj Middle School Hajipur Diyara, 3-Vill- Hajipur Diyara, Dist- 1 3 Sulekha Devi 7739650069 (Old Building) Sahibganj 4-Vill- Hajipur Bhitta, Dist- 1 4 Up. Middle School, Rajgaown Ramakanta Devi 8936016787 Sahibganj 5-Vill- Hajipur Bhitta, Dist- 1 5 Up. Middle School, Rajgaown Babita Devi 9973195910 Sahibganj 1 6 Panchayat Building, Dihari Manju Kumari 9973195910 6-Vill- Dihari, Dist- Sahibganj 1 7 Up.High School,, Dihari Ajay Kumar Yadav 7766017485 7-Vill- Dihari, Dist- Sahibganj Up. Middle School, Patwar 8-Vill- Patwar Tola, Dist- 1 8 Rita Devi 9801340228 Tola Sahibganj Up. Middle School, Patwar 1 9 Usha Devi 9661205005 9-Vill- Dihari, Dist- Sahibganj Tola Up. Middle School Badi 10-Vill-Bholiya Tola, Dist- 1 10 Shavya Devi 8409462362 Kodarjanna Sahibganj Middle School Badi 11-Vill-Bari Kojarjanna South, 1 11 Renu Devi 9006958107 Kodarjanna (South Part) Dist- Sahibganj Middle School Badi 12-Vill-Mahaldar Tola, Dist- 1 12 Shrimani Devi 8271720579 Kodarjanna (North Part) Sahibganj Middle School Badi 13-Vill- Naya Tola, Dist- 1 13 Kiran Devi 9771823375 Kodarjanna (North Part) Sahibganj Urdu Middle School 14-Vill- Makhmalpur South, 1 14 Akhtari Begam 9801430040 Makhmalpur Dist- Sahibganj Panchayat Building 15-Vill-Rahamat Tola, Dist- 1 15 Anjuman Aara 7295915866 Makhmalpur ( South Part) Sahibganj Panchayat Building 16-Vill- Sarpanch Tola, Dist- 1 16 Alimuddin Jang 9798190712 Makhmalpur ( South Part) Sahibganj Up. -

Obtaining Environmental Clearance
OBTAINING ENVIRONMENTAL CLEARANCE CATEGORY FOR TETRIYA STONE DEPOSIT (MINOR MINERAL), IN TETRIYA MOUZA OF SAHIBGANJ B2 DISTRICT, JHARKHAND STATE {AREA COVER 9.87 ACRES (3.995 HA)} PROJECT FORM-IM I. BASIC INFORMATION :- Sl. Item Details No. I. Name of the Mining Lease site Tetriya Stone Deposit II. Location/site Location: (GPS Co-ordinates) Mouza – Tetriya, P.S. – Taljhari, Dist – Sahibganj, Jharkhand. Boundary Location (Co – ordinates) Pillar No. Latitude Longitude A N25°02'38.00" E87°42'07.36" B N25°02'42.36" E87°42'04.40" C N25°02'49.92" E87°42'12.29" D N25°02'43.81" E87°42'14.78" III. Size of the Mining Lease (Hectare) 9.87 Acres / 3.995 Ha J.B. No 1 2 7 8 Plot No. 19(P) 34(P), 36(P) 17(P) 18 IV. Capacity of the mine Lease (TPA) 2,80,956 Tonnes / Annum 937 Tonnes / Day V. Period of Mining Lease Fresh Area. Applied on 17.01.2018 VI. Expected Cost of the project 44 Lakhs VII. Contact Information M/s Dadi Maa Stone Works Partners: Sri Sanjay Kumar Bhuwaniya and Md. Shamim At–Makhani, P.O. - Taljhari, P.S. – Rajmahal, Sub-Division – Rajmahal, Dist – Sahibganj, Jharkhand, Pin -816129 Phone No. – +91-9973848050/9955948836 Email ID: [email protected] PROJECT PROPONENT PAGE 1 M/S DADI MAA STONE WORKS OBTAINING ENVIRONMENTAL CLEARANCE CATEGORY FOR TETRIYA STONE DEPOSIT (MINOR MINERAL), IN TETRIYA MOUZA OF SAHIBGANJ B2 DISTRICT, JHARKHAND STATE {AREA COVER 9.87 ACRES (3.995 HA)} PROJECT II. ENVIRONMENTAL SENSITIVITY :- Sl. Areas Distance in Kilometer / Details No. -
List of Consumers of Sahibganj
SL. NO Consumer No. Consumer Name Consumer Address Tarrif Total Amount 298 GVCS000006 THE I/C MEDICAL OFFICER RANGA HOSPITAL, RANGA NDS-3 11,58,453 397 GVCS000046 DISTRICT HOMEGAURD COMMANDENT OFFICE, BANSKOLA,SAKRIGALI NDS-3 10,96,411 396 GVCS000029 B.D.O. , RAJMAHAL , NAYA BAZAR,RAJMAHAL NDS-3 10,90,657 395 GVCS000030 B D O , TALJHARI BLOCK NDS-3 10,88,846 297 MJPCS00557 BHARTI INFRATEL LTD PROP- A DWIVEDI, MIRZAPUR NDS-3 7,91,505 392 TPCS000005 DIVN.ELEC.EXEC.ENGINEER , E.RLY,MALDA,AT-TEENPAHAR NDS-3 6,98,808 198 LHDCS00001 SUNIL KR BHARTIYA S/o LT MURARILAL BHARTIYA, LOHANDA,AT-PETROL PUMP NDS-3 6,81,282 296 BHCS002471 ADIWASI KALYAN HOSTEL B S K COLLEGE, BARHARWA NDS-3 6,14,929 386 GVCS000002 SUPDT OF POLICE , RAJMAHAL THANA NDS-3 6,11,735 385 GVCS000033 CIVIL S.D.O. , S.D.O. COURT,RAJMAHAL NDS-3 6,11,126 295 GVCS000015 THE B.D.O. , PATHNA BLOCK,PATHNA NDS-3 5,93,452 294 GVCS000014 THE PRAKHAND BIKASH OFFI. , BARHARWA BLOCK NDS-3 5,90,543 380 GVCS000004 THANA INCHARGE , RADHANAGAR THANA,UDHWA NDS-3 5,14,026 191 MZCCS00783 BRANCH MANAGER STATE BANK OF INDIA, MIRZA CHAUKI NDS-3 4,79,984 190 MDSCS00045 BRANCH MANAGER STATE BANK OF INDIA, CHHOTA MADANSAHI NDS-3 4,63,921 188 BROCS00546 HEAD MASTER STR GIRLS HIGH SCHOOL, BANDARKOLA,BORIO,SAHIBGAN NDS-3 4,56,278 377 GVCS000007 MEDICAL OFFICER , REFERAL HOSPITAL,RAJMAHAL NDS-3 4,32,801 179 GVCS000009 DIST EMPLOYMENT OFFICE , LOHANDA NDS-3 3,98,842 373 GVCS000001 SUPDT OF JAIL , RAJMAHAL NDS-3 3,75,802 369 RJLCS01800 ATC TOWER OF INDIA (P) LT C/o MD ZIAUDDIN AHMED, GUDRAGHAT,RAJMAHAL NDS-3 -
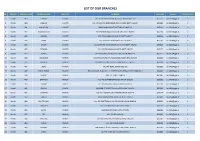
List of Our Branches
LIST OF OUR BRANCHES SR REGION BRANCH CODE BRANCH NAME DISTRICT ADDRESS PIN CODE E-MAIL CONTACT NO 1 Ranchi 419 DORMA KHUNTI VILL+PO-DORMA,VIA-KHUNTI,DISTT-KHUNTI-835 227 835227 [email protected] 0 2 Ranchi 420 JAMHAR KHUNTI VILL-JAMHAR,PO-GOBINDPUR RD,VIA-KARRA DISTT-KHUNTI. 835209 [email protected] 0 3 Ranchi 421 KHUNTI (R) KHUNTI MAIN ROAD,KHUNTI,DISTT-KHUNTI-835 210 835210 [email protected] 0 4 Ranchi 422 MARANGHADA KHUNTI VILL+PO-MARANGHADA,VIA-KHUNTI,DISTT-KHUNTI 835210 [email protected] 0 5 Ranchi 423 MURHU KHUNTI VILL+PO-MURHU,VIA-KHUNTI, DISTT-KHUNTI 835216 [email protected] 0 6 Ranchi 424 SAIKO KHUNTI VILL+PO-SAIKO,VIA-KHUNTI,DISTT-KHUNTI 835210 [email protected] 0 7 Ranchi 425 SINDRI KHUNTI VILL-SINDRI,PO-KOCHASINDRI,VIA-TAMAR,DISTT-KHUNTI 835225 [email protected] 0 8 Ranchi 426 TAPKARA KHUNTI VILL+PO-TAPKARA,VIA-KHUNTI, DISTT-KHUNTI 835227 [email protected] 0 9 Ranchi 427 TORPA KHUNTI VILL+PO-TORPA,VIA-KHUNTI, DISTT-KHUNTI-835 227 835227 [email protected] 0 10 Ranchi 444 BALALONG RANCHI VILL+PO-DAHUTOLI PO-BALALONG,VIA-DHURWA RANCHI 834004 [email protected] 0 11 Ranchi 445 BARIATU RANCHI HOUSING COLONY, BARIATU, RANCHI P.O. - R.M.C.H., 834009 [email protected] 0 12 Ranchi 446 BERO RANCHI VILL+PO-BERO, RANCHI-825 202 825202 [email protected] 0 13 Ranchi 447 BIRSA CHOWK RANCHI HAWAI NAGAR, ROAD NO. - 1, KHUNTI ROAD, BIRSA CHOWK, RANCHI - 3 834003 [email protected] 0 14 Ranchi 448 BOREYA RANCHI BOREYA, KANKE, RANCHI 834006 [email protected] 0 15 Ranchi 449 BRAMBEY RANCHI VILL+PO-BRAMBEY(MANDER),RANCHI-835205 835205 [email protected] 0 16 Ranchi 450 BUNDU -

Directory Establishment
DIRECTORY ESTABLISHMENT SECTOR :RURAL STATE : JHARKHAND DISTRICT : Bokaro Year of start of Employment Sl No Name of Establishment Address / Telephone / Fax / E-mail Operation Class (1) (2) (3) (4) (5) NIC 2004 : 1010-Mining and agglomeration of hard coal 1 PROJECT OFFICE POST OFFICE DISTRICT BOKARO, JHARKHAND , PIN CODE: 829144, STD CODE: NA , TEL NO: NA , FAX 1975 51 - 100 MAKOLI NO: NA, E-MAIL : N.A. 2 CENTRAL COAL FIELD LIMITED AMLO BERMO BOKARO , PIN CODE: 829104, STD CODE: NA , TEL NO: NA , FAX NO: NA, 1972 101 - 500 E-MAIL : N.A. 3 PROJECT OFFICER KHASMAHAL PROJECT VILL. KURPANIA POST SUNDAY BAZAR DISTRICT BOKARO PIN 1972 101 - 500 CODE: 829127, STD CODE: NA , TEL NO: NA , FAX NO: NA, E-MAIL : N.A. 4 SRI I. D. PANDEY A T KARGAL POST . BERMO DISTRICT BOKARO STATE JHARKHAND , PIN CODE: NA , STD CODE: 06549, TEL NO: 1960 > 500 221580, FAX NO: NA, E-MAIL : N.A. 5 SRI S K. BALTHARE AT TARMI DAH DISTRICT BOKARO STATE - JHARKHAND , PIN CODE: NA , STD CODE: NA , TEL NO: NA 1973 > 500 P.O.BHANDARI , FAX NO: NA, E-MAIL : N.A. 6 PROJECT OFFICER CCL MAKOLI POST CE MAKOLI DISTRICT BOKARO STATE JAHARKHAND PIN CODE: 829144, STD CODE: NA , TEL 1975 > 500 OFFFI NO: NA , FAX NO: NA, E-MAIL : N.A. NIC 2004 : 1410-Quarrying of stone, sand and clay 7 SANJAY SINGH VILL KHUTR PO ANTR PS JARIDIH DIST BOKARO JHARKHANDI PIN CODE: 829138, STD CODE: 1989 10 - 50 NA , TEL NO: NA , FAX NO: NA, E-MAIL : N.A. -

Urma Paharitola Coal Block Summary
URMA PAHARITOLA COAL BLOCK SUMMARY PART A Sr. Features Details No. 1. Location Coal Block Urma Paharitola Latitude 24029’48”N- 24032’21”N (PROVISIONAL) Longitude 87029’55”E- 87031’36”E (PROVISIONAL) Topo Sheet No. 72P/10 Coalfield Rajmahal Group of Coalfields District Dumka and Pakur State Jharkhand 2. Connectivity with Block Nearest Rail Head The nearest railhead is Muraroi, which is about 37 km from Amrapara. This area is approachable from Amrapara by Amrapara-Alubera metalled road as well as from Durgapur along Durgapur Silingi forest road. Both Road Amrapara and Durgapur are connected by motorable Dumka-Pakur metalled road and are about 46 and 51km respectively from Dumka. 3. Area Geological Block Area 9.76 sq.km. (As per shape file. Refer Note) Forest Area Approx. 15 % (As per FSI map) Non-Forest Area Approx. 85 %(As per FSI map) 4. Climate and Topography Average Annual Rainfall 1000 mm Local Surface The terrain depicts, in general, a gently undulating topography with few Drainage Channels isolated hillocks in the southern and northern part. The main coal bearing area with subdued topography is skirted on the northern, eastern and southern sides by hills of basic volcanic rocks. The general elevation of the low ground straddles between 80 m and 105 m, while the hill in the southern part attains a maximum altitude of 135 m above the mean sea level. Bansloi, the main surface run-off flowing from west to east drains the central part of the area. A few ephemeral streamlets originating from the northern and southern uplands and fed by the rain water, criss-cross the tract and eventually meet the Bansloi river, which together constitute the drainage system of the area. -

1.0 Brief on 4000 MW Deoghar Ultra Mega Power Project to Be Set up in Pipra Village, Mohanpur Anchal, District Deoghar, Jharkhand
1.0 Brief on 4000 MW Deoghar Ultra Mega Power Project to be set up in Pipra village, Mohanpur Anchal, District Deoghar, Jharkhand 1.1 Ministry of Power, Govt. of India has taken the initiative to develop coal based Ultra Mega Power Projects (UMPPs) of 4000 MW capacity (using Supercritical Technology) in different parts of the country. Power Finance Corporation Limited (PFC) is the nodal agency and Central Electricity Authority (CEA) is providing technical support for development of these UMPPs. 1.2 A 4000 MW UMPP is proposed to be set up Mohanpur Anchal in Deoghar district of Jharkhand. In this regard, Deoghar Mega Power Limited (DMPL), a wholly owned subsidiary of PFC Ltd. has been incorporated as a Special Purpose Vehicle to carry out technical studies, obtain all linkages, clearances and approvals and to select a developer for the Project through International Competitive Bidding process as per the Guidelines and Standard Bidding Documents issued by Ministry of Power, Govt of India. 1.3 Jharkhand is one of the power- starved states in the country with high potential for development. The 4000 MW UMPP will play a key role in providing the much needed power to overcome the short fall as well as in spurring all round economic development in the State. It will also supply power to other states as per the allocation given below: Sl. No. Procurer Power Allocated (MW) 1 Jharkhand 1500 2 Gujarat 1000 3 Tamil Nadu 600 4 Karnataka 300 5 Haryana 200 6 Kerala 200 7 Goa 200 Total 4000 1.4 Location The site is located under the block office of Mohanpur of Deoghar District at about 16 kilometers North of the Deoghar district town. -

PAKUR (Jharkhand)
A BASELINE SURVEY OF MINORITY CONCENTRATION DISTRICTS OF INDIA PAKUR (Jharkhand) Sponsored by Ministry of Minority Affairs Government of India and Indian Council of Social Science Research INSTITUTE FOR HUMAN DEVELOPMENT NIDM Building, 3rd Floor, IIPA Campus I.P. Estate, Mahatma Gandhi Marg, New Delhi - 110 002 Phones – 2335 8166, 2332 1610 / Fax: 2376 5410 Email: [email protected], website: www.ihdindia.org 2008 A BASELINE SURVEY OF MINORITY CONCENTRATION DISTRICTS OF INDIA PAKUR (Jharkhand) Sponsored by Ministry of Minority Affairs Government of India and Indian Council of Social Science Research INSTITUTE FOR HUMAN DEVELOPMENT NIDM Building, 3rd Floor, IIPA Campus I.P. Estate, Mahatma Gandhi Marg, New Delhi - 110 002 Phones – 2335 8166, 2332 1610 / Fax: 2376 5410 Email: [email protected], website: www.ihdindia.org RESEARCH TEAM Principal Researchers Alakh N. Sharma Ashok K. Pankaj Data Processing and Tabulation Balwant Singh Mehta Sunil Kumar Mishra Abhay Kumar Research Associates/Field Supervisors Ramashray Singh Ashwani Kumar Subodh Kumar M. Poornima Research Assistant P.K. Mishra Secretarial Assistance Shri Prakash Sharma Nidhi Sharma Sindhu Joshi PAKUR Principal Author of the Report HARISHWAR DAYAL Regional Director, Institute for Human Development Ranchi CONTENTS Executive Summary................................................................................................i-iv CHAPTER I: INTRODUCTION ...............................................................................1-9 Methodology...............................................................................................................