Vol.6 No. 3 in This Issue
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Developmental Pattern of Human Milk Teeth
Int J Oral-Med Sci 9(2):75-87,2010 Original Article Developmental Pattern of Human Milk Teeth Kazuya Ohzeki,Rumi Ota-Yokota,and Hayato Ohshima Departments ofOral Diagnostics,and Histology,Cytology and Developmental Anatomy,Nihon University School of Dentistry at Matsudo,Matsudo,Chiba 271-8587,Japan Divisions of Anatomy and Cell Biology of the Hard Tissue,Niigata University Graduate School of Medical and Dental Sciences,Niigata,Niigata 951-8510,Japan Correspondence to: Kazuya Ohzeki The development of mammalian tooth cusps or ridges has been ex- E-mail: ohzeki.kazuya@ nihon-u.ac. plained by phylogenetic homology,such as the‘Tritubercular theory’ jp (Gregory 1934).However,descriptions of the incisor and canine are lacking, and many questions remain unanswered. In this paper, the authors examine crown development in human teeth in embryos and skulls of young children by micro computed tomography(μ-CT),and discuss these problems.The results were as follows: 1)In milk incisors and canines,the first swelling developed into the central marginal ridge,and new swellings became mesial and distal sites and also buccal and mesial sites. Mesial and distal promi- nences developed into mesial and distal mamelons,but labial and lingual swellings formed cingulums. 2)In upper first milk molars,the first swelling developed into a buccal cusp and new swellings around it became buccal and lingual,and also mesial and distal sites symmetrically.The lingual prominence formed a lingual cusp,and the mesial and distal prominences for- med mesial and distal cones or marginal ridges,but only the labial prominences developed into a mesio-buccal ridge. -

Biomechanics of Temporo-Mandibular Joint. Articilator. Movements of Mandible Protrusion Retrusion Lateral Excursion Opening-Closing
Biomechanics of temporo-mandibular joint. Articilator. Movements of mandible Protrusion Retrusion Lateral excursion Opening-Closing Opening-Closing Translatory movement of the mandibular condyle along the posterior wall of the articular eminence. Protrusion A protrusive movement occurs when the mandible moves forward. Retrusion Retraction of the mandible from any position Lateral excurcion When the mandible moves into a left lateral excurcion the right condyle moves forward and inward (Bennett angle), while the left condyle will shift slightly in a lateroposterior direction(Bennett movement). In this example, the left side is working side and the right side is nonworking side. When the mandible moves into a right lateral excurcion the left condyle moves forward and inward (Bennett angle), while the right condyle will shift slightly in a lateroposterior direction(Bennett movement). In this example, the right side is working side and the left side is nonworking side. Border movements of the mandible The most extreme positions to which the jaw is able to move. Laterally: max 10 mm Opening: 50-60 mm Protrusion: 9mm Retrusion:1 mm Described from sagittal, frontal and horizontal planes. Usually not affected by head or body posture. Mandibular movements Most mandibular movements occur around three dimensions. They include, the transverse(horizontal), vertical(frontal) and sagittal axes. Mandibular movements can be classified as border and intraborder movements. Border movements occuring in all three planes and intraborder movements are all possible movements of the mandible occur within the border envelope. Extreme movements in the sagittal plane The patient is instructed to move the mandible from centric relation(CR) to centric occlusion(CO), then edge to edge relationship(ER), then the maximum protrusive (MP) and then arc downward to the maximum opening position. -

Learning Curve 8% Offer Campuses
Learning Curve 8% Cash Back offer for student licence purchases made using Virgin Money Spot - Available for the following campuses: Name Address AAA School of Advertising 1st Floor, Bond Street Centre, Cnr Bram Fischer Drive & Bond Street, Kensington B, Randburg, 2194 BHC School of Design 72 Salt River Road, Woodstock, Cape Town, 7925 Boston City Campus & Business College 247 Louis Botha Avenue, Orchards, Orange Grove, Johannesburg 2192 Boston Media House 137, 11th Street,Parkmore, Johannesburg 2196 Cape Town College of Fashion Design 7 Delaney Road, Plumstead, Cape Town, 7801 Cape Town Creative Academy The Old Biscuit Mill, 375 Albert Road, Woodstock, Cape Town, 7915 Capricorn TVET College Die Meer Street,Polokwane 0699 Centurion Akademie - Rustenberg 39 Heystek Street, Rustenburg Centurion Academy 1023 Bank Avenue Centurion City Varsity Cape Town Coastal KZN FET College 1 Jameson Crescent, Congella, 4013, Durban Concept Interactive COMMUNITYWest Block, Tannery ARTS CENTRE, Park, 23 LEONARD Belmont AUALA Road, Rondebosch,STREET, WINDHOEK, Cape Town, NAMIBIA 7700 College of The Arts (Reseller: PC Centre) CTU Training Solutions Unit 26, Garsfontein Office Park, 645 Jacqueline Drive, Pretoria, 1788 Design Academy of Fashion 208 Albert Road, Woodstock, Cape Town, 7925 East London Management Institute 231 Oxford Street, East London, 5201 Elizabeth Galloway Fashions Techno Road, 26 Techno Avenue, Stellenbosch, 7600 Faculty Training Institute CT Faculty Training Institute Joburg Fedisa 81 Church Street, Cape Town, 8001 Friends of Design Business -

Saieg Directory Final
SAIEG Directory 2014 DIRECTORY OF SAIEG MEMBERS Regions and areas of expertise CONTENTS Section A List of members according to regions (province / country) Section B Member contact details in alphabetical order with principle work disciplines (in italics) followed by primary and secondary areas of expertise. Information herein was correct at the time of compilation. The website www.saieg.co.za, is constantly being updated with information as it comes to hand. Page 1 SAIEG Directory 2014 SECTION A MEMBERS AND REGIONS Eastern Cape Province Mulville, Dudley Hingston, Egerton Naidoo, Salona Isherwood, Casper De Jager, Frederick Ndlovu,Siyamazi Zamagatsheni James, Garth Fyvie, Richard Nell, Johann Jermy, Colin Proudfoot, Marinus Louis Netterberg, Dr Frank Kriek, Johan Ngubelanga, Sifiso Lynn, Bruce Gauteng Province Ntengnou, Ndamkou Gerard Mahabeer, Prashant A'Bear, Tony Oliver, Denzil Maud, Rodney Antrobus, Bryan Ralph Oosthuizen, Tharina Naidoo, Deven Arkert, Jan Paige-Green, Prof Philip Ndlela, Gugu Renolda Aucamp, Paul Pidgeon, John Terry Nxumalo, Ayanda Francis Barker, Oliver Pillay, Ohveshlan Pather, Sundras Barnard, Hendrik (Ian) Puchner, Richard Pillay, Sue-Anya Bester, Anton Michael Purnell, Dave Price, Dr Gordon Vivian Bloem, Jaco Rabodiba, Godwill Richter, Mark Vincent Bredenkamp, Brendon Reddy, Kogalin Shriram, Rahul Breytenbach, Izak Richer, Lindi Singh, Riona Brink, George Robson, John Wessels, Colin Buttrick, Dr David Belton Roussel, Julien Wilson-Jones, Brett Canahai, Cecilia Roux, Pierre Lategan Chiliza, Sibonakaliso Goodman -
Anatomical Landmarks in Order to Study an Individual Tooth Intelligently, We Must Be Able to Recognize All Landmarks of Importance by Name
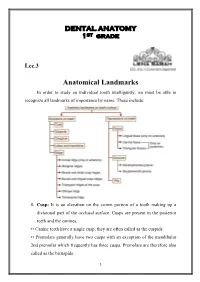
DENTAL ANATOMY 1ST grade Lec.3 Anatomical Landmarks In order to study an individual tooth intelligently, we must be able to recognize all landmarks of importance by name. These include: 1. Cusp: It is an elevation on the crown portion of a tooth making up a divisional part of the occlusal surface. Cusps are present in the posterior teeth and the canines. •• Canine teeth have a single cusp; they are often called as the cuspids. •• Premolars generally have two cusps with an exception of the mandibular 2nd premolar which frequently has three cusps. Premolars are therefore also called as the bicuspids. 1 •• Maxillary and mandibular 1st molars have five cusps, while other molars generally have four cusps. Each cusp is a gothic pyramid with four sides formed by four ridges that run down from the cusp tip: •• Mesial and distal cusp ridges (cusp slopes) •• Buccal/lingual cusp ridge •• Triangular ridge of the cusp. There are two cusp slopes on either side of the triangular ridge. In case of canines, there is a labial ridge analogous to the buccal ridge posterior teeth; there is a lingual ridge analogous to triangular ridge of posterior teeth. In the Table below the Number of cusps in different types of teeth: Tooth type Maxillary arch Mandibular arch Incisors 0 0 Canines 1 1 Premolars 2 2 in 1st premolar 3 or 2 in 2nd premolar Molars 1st molar 4 +1 accessory cusp 5 (cusp of Carabelli) 2nd molar 4 4 3rd molar 4 or 3 4 or 5 A cusp is named according to its location on the tooth. -

Dental Assisting Science I
ADED 110C: Dental Assisting Science I Hours: Lecture - 3, Lab - 0, Credits - 3 Prerequisite: none Term & Dates: Fall 2020 Faculty: Kelly O’Brien, CDA, RDH, MEd Faculty Accessibility: available via discussion board and email, virtual conferences by appointment Email: [email protected] DRAFT Course Outline – official syllabus will be available in August Course Description A study of the anatomy of the head, emphasizing the osteological landmarks and the structures of the oral cavity. Both the permanent and primary dentitions are studied, including embryonic development and eruption patterns. In addition, an introduction to the structure and function of the human body systems in health and disease will be presented. Return to Top Learning Outcomes Educated Person Statement of Philosophy Upon completion of this course, students will be able to: Pronounce, spell, and define key terminology required to function within the profession. Identify any tooth on the oral cavity by name, number, location, function and shorthand terms. Discuss the development of the head and neck from conception through adulthood with a focus on the oral cavity. Describe the major systems of the body, their functions, and relationship to oral health. Acquired Knowledge and Skills: List the classifications and function of each of the teeth. Identify the different tissues of the teeth and oral cavity. Identify the arrangement of the dentitions by arch, quadrant, and sextant. Label the surfaces of any tooth, and the divisions into thirds of the root and the crown. 1 Describe the dentitions using eruption and shedding dates. Provide the shorthand identification of each tooth using Palmer, FDI, and Universal. -

City Suburb Postalcode Zone ALBERTON MEYERSDAL 1447
City Suburb PostalCode Zone ALBERTON MEYERSDAL 1447 Local ALBERTON ALBERTSDAL 1448 Local ALBERTON ALBERTSDAL EXT 17 1448 Local ALBERTON ALBERTSDAL EXT 18 1448 Local ALBERTON ALBERTSDAL EXT 6 1448 Local ALBERTON BRACKEN DOWNS 1448 Local ALBERTON BRACKEN DOWNS EXT 1 1448 Local ALBERTON BRACKEN DOWNS EXT 2 1448 Local ALBERTON BRACKEN DOWNS EXT 3 1448 Local ALBERTON BRACKEN DOWNS EXT 4 1448 Local ALBERTON BRACKEN DOWNS EXT 5 1448 Local ALBERTON BRACKENHURST 1448 Local ALBERTON BRACKENHURST EXT 1 1448 Local ALBERTON BRACKENHURST EXT 2 1448 Local ALBERTON MABALIA 1448 Local ALBERTON MAYBERRY PARK 1448 Local ALBERTON MAYBERRY PARK EXT 1 1448 Local ALBERTON MEYERSDAL 1448 Local ALBERTON ALBERANTE 1449 Local ALBERTON ALBERANTE EXT 1 1449 Local ALBERTON ALBERTON 1449 Local ALBERTON ALBERTON EXT 28 1449 Local ALBERTON ALBERTON NORTH 1449 Local ALBERTON ALBERTON-NOORD 1449 Local ALBERTON ELANDSHAVEN 1449 Local ALBERTON FLORENTIA 1449 Local ALBERTON GENERAAL ALBERTSPARK 1449 Local ALBERTON NEW REDRUTH 1449 Local ALBERTON NEWMARKET 1449 Local ALBERTON NEWMARKET PARK 1449 Local ALBERTON NEWMARKET PARK EXT 1 1449 Local ALBERTON RACEVIEW 1449 Local ALBERTON RANDHART 1449 Local ALBERTON RANDHART EXT 1449 Local ALBERTON RANDHART EXT 1 1449 Local ALBERTON RANDHART EXT 2 1449 Local ALBERTON RANDHART EXT 4 1449 Local ALBERTON SOUTH CREST 1449 Local ALBERTON VERWOERDPARK 1449 Local ALBERTON ALRODE 1451 Local ALBERTON ALRODE SOUTH EXT 1451 Local ALBERTON BRACKEN GARDENS 1452 Local ALBERTON VERWOERDPARK 1453 Local ALBERTON EDEN PARK 1455 Local ALBERTON ALBERTON -

Provincial Gazette Provinsiale Koerant
THE PROVINCE OF DIE PROVINSIE VAN UNITY DIVERSITY GAUTENG IN GAUTENG Provincial Gazette Provinsiale Koerant Selling price • Verkoopprys: R2.50 Other countries • Buitelands: R3.25 PRETORIA Vol. 22 1 JUNE 2016 No. 190 1 JUNIE 2016 PART 1 OF 2 We oil Irawm he power to pment kiIDc AIDS HElPl1NE 0800 012 322 DEPARTMENT OF HEALTH Prevention is the cure ISSN 1682-4525 N.B. The Government Printing Works will 00190 not be held responsible for the quality of “Hard Copies” or “Electronic Files” submitted for publication purposes 9 771682 452005 2 No. 190 PROVINCIAL GAZETTE, 1 JUNE 2016 Government Printing Works NWUNo+ot iiceice sSUbI'nsa0baubmi siSSsiionon deid&akae a ddll iineisnes Government Printing Works has over the last few months implemented rules for completing and submitting the electronic Adobe Forms when you, the customer, submit your notice request. In line with these business rules, GPW has revised the notice submission deadlines for all gazettes. Please refer to the GPW website www.gpwonline.co.za to familiarise yourself with the new deadlines. cancellations Cancellation of notice submissions are accepted by GPW according to the deadlines stated in the table above. Non-compliance to these deadlines will result in your request being failed. Please pay special attention to the different deadlines for each gazette. Please note that any notices cancelled after the cancellation deadline will be published and charged at full cost. Requests for cancellation must be sent by the original sender of the notice and must accompanied by the relevant notice reference number (N-) in the email body. Amendments to notices With effect from 01 October, GPW will not longer accept amendments to notices. -

Noritake Super Porcelain EX-3
Porcelain for metal ceramic dental restorations Noritake Super Porcelain EX-3 Technical Instructions Contraindications: If the patient is hypersensitive to potassium-aluminosilicate glass or any other components, this product must not be used. Caution: 1. If the patient or the dental professional demonstrates a hypersensitivity reaction, such as rash, dermatitis, etc., discontinue use of the product and seek medical attention immediately. 2. When mixing materials or grinding a restoration being fabricated, use an approved dust mask and vacuum with air filter to protect your lungs from inhaling the dust. 3. When mixing materials or grinding a restoration being fabricated, use safety glasses to prevent the dust from getting into your eyes. If the dust gets into your eyes, immediately rinse with copious amounts of water and consult a physician. 4. Do not use for any purposes except for fabricating dental restorations. This product is for dental application only. 5. Do not touch the items heated by the furnace with your bare hands. 6. Paste Opaque, Paste Opaque Modifier, PASTE OPAQUE LIQUID, IS LIQUID, ES LIQUID and UP LIQUID are flammable. Do not use them near fire or high-temperature objects. 7. IS LIQUID is a stimulant liquid. When using it, have good ventilation and if necessary wear an approved dust mask, safety glasses and gloves. 8. Stain and plaque can accumulate on a restoration, once it has been put in position in the patient’s oral cavity, depending on the patient's eating habits or food choices. Instruct patients about the importance of cleaning their restorations. Precautions in use: 2 1. -

Participating Engen Garages
Participating Engen garages Branch name Street address Area Province The Bridge Service Station 14 CJ Langenhoven Drive Greenacres Eastern Cape Kimjer Motors 37 Piet Retief Street Burgersdorp Eastern Cape Beachway Auto Centre Cnr Humewood & Perrott Road, Humewood Port Elizabeth Eastern Cape Mount Pleasant Motors 14 Buffelsfontein Road Mount Pleasant Eastern Cape Mdantsane Retail Centre 9692 Zone Mdantsane East London Eastern Cape Peddie Motors N2 Main Road Peddie Eastern Cape Leo Motors 34 Main Street Kirkwood Eastern Cape PZ Motors 322 Main Road, Flagstaff Transkei Eastern Cape Mount Ayliff Service Station 1 Nolangeni Street Mount Ayliff Eastern Cape Algoa Park Motors St Leonards Road, Algoa Park Port Elizabeth Eastern Cape Tsolo Motors 88 Thurston Street Tsolo Eastern Cape A&J Motors 3 Umtata Street Butterworth Eastern Cape Ubuntu Motors Cnr Phalo Crescent & Komga Road Bisho Eastern Cape Smith and Wiggill 24 Griffith Street Queenstown Eastern Cape Queens Convenience Centre 19A Cathcart Road Queenstown Eastern Cape Greenacres Auto Centre 10 Ring Road, Greenacres Port Elizabeth Eastern Cape Airport Motors Retail Centre 9 Breezyvale Road, Orange Grove East London Eastern Cape Progress Service Station / 35 Thompson Avenue Bizana Eastern Cape De Boer’s Fuel CC Bergview 1 Stop Boschetto Avenue Harrismith Free State Etienne Convenience Centre 102 Toronto Road Welkom Free State Auto Land Convenience Centre Cnr Tempest & Volks Road, Jim Fouchepark Welkom Free State Vyfster Motors Cnr De La Rey & Curie Avenue Bloemfontein Free State Captains Retail -
Netflorist Designated Area List.Pdf
Subrub ID Suburb Name City Name Zone Name IsExtendedHourSuburb 27924 carswald kyalami Johannesburg Johannesburg (North) True 30721 montgomery park Johannesburg Johannesburg (North) True 28704 oaklands Johannesburg Johannesburg (North) True 28982 sunninghill Johannesburg Johannesburg (North) True 29534 • bramley Johannesburg Johannesburg (North) True 8736 Abbotsford Johannesburg Johannesburg (North) True 28048 Abbotts ford Johannesburg Johannesburg (North) True 29972 Albertskroon Johannesburg Johannesburg (North) True 897 Albertskroon Randburg Johannesburg (North) True 29231 Albertsville Johannesburg Johannesburg (North) True 898 Albertville Randburg Johannesburg (North) True 28324 Albertville Johannesburg Johannesburg (North) True 29828 Allandale Johannesburg Johannesburg (North) True 30099 Allandale park Johannesburg Johannesburg (North) True 28364 Allandale park / midrand Johannesburg Johannesburg (North) True 9053 Allen Grove Johannesburg Johannesburg (North) True 8613 Allen Grove Johannesburg Johannesburg (North) True 974 Allen Grove Kempton Park Johannesburg (North) True 30227 Allen neck Johannesburg Johannesburg (North) True 31191 Allen’s nek, 1709 Johannesburg Johannesburg (North) True 31224 Allens neck Johannesburg Johannesburg (North) True 27934 Allens nek Johannesburg Johannesburg (North) True 27935 Allen's nek Johannesburg Johannesburg (North) True 975 Allen's Nek Roodepoort Johannesburg (North) True 29435 Allens nek, rooderport Johannesburg Johannesburg (North) True 30051 Allensnek, Johannesburg Johannesburg (North) True 28638 -
Surfaces and Ridges
Surfaces and ridges • The crowns of incisors and canines have four surfaces and ridge, while the crowns of premolars and molars have five surfaces The surfaces are: 1. Labial surface: is the surface which is toward the lip in incisors and canines (in anterior teeth). 2. Buccal surface: is the surface which is toward the cheek in premolars and molars (posterior teeth). The labial and buccal surfaces could be termed as the "facial surfaces". 3. Lingual surface: is the surface which is facing the tongue (all teeth). 4. Occlusal surface: is the surface of the posterior teeth coming in contact with the teeth in the opposite jaw during closing the mouth. In anterior teeth, this surface is called "incisal ridge". 5. Proximal surface: is the surface of the tooth facing toward adjacent teeth in the same dental arch. a. Mesial surface: is the surface which is facing toward the median line. b. Distal surface: is the surface which is facing away from the median line. All teeth have their mesial surfaces touching the distal surfaces of the adjacent tooth except the maxillary and mandibular central incisor (both permanent and deciduous).The area of the mesial and distal surface that touch its neighbor in the arch is called the "contact area". Division of the crown into thirds • For description, the crown and the root are divided into thirds according to the position of the surface. • Line angle: it is formed by the junction of two surfaces and gets its name from these surfaces. Example: mesio-labial line angle. • Point angle: it is formed by junction of three surfaces and get its name from these surfaces.