Renal Clearance
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
ANS: 600 Ml/Min This Is the Renal Plasma Flow, Which Is Given As the Clearance of PAH
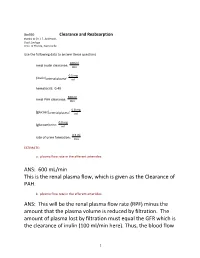
Bio390 Clearance and Reabsorption thanks to Dr. J.F. Anderson, Dept Zoology Univ. of Florida, Gainesville Use the following data to answer these questions. 100 ml renal inulin clearance: min 0.5 mg [inulin]arterial plasma: ml hematocrit: 0.40 600 ml renal PAH clearance: min 0.8 mg [glucose]arterial plasma: ml 0.0 mg [glucose]urine: ml 0.5 ml rate of urine formation: min ESTIMATE: a. plasma flow rate in the afferent arterioles: ANS: 600 mL/min This is the renal plasma flow, which is given as the Clearance of PAH. b. plasma flow rate in the efferent arterioles: ANS: This will be the renal plasma flow rate (RPF) minus the amount that the plasma volume is reduced by filtration. The amount of plasma lost by filtration must equal the GFR which is the clearance of inulin (100 ml/min here). Thus, the blood flow 1 in the efferent arteriole is 600 - 100 ml/min = 500 ml/min in this problem c. plasma flow rate in the renal veins: ANS: by the time that blood enters the veins, nearly all of the water lost during filtration has made its way back to the blood (especially if the subject is dehydrated!). If urine is being formed at a rate of 0.5 mL/min, then that represents (essentially) the volume of water lost per min. So, the renal venous plasma flow rate = RPF- urine loss = 600 - 0.5 = 599.5 ml/min d. renal blood flow rate in renal artery in ml/min ANS: 833 mL/min the hct = 40% (0.4). -

Renal Effects of Atrial Natriuretic Peptide Infusion in Young and Adult ~Ats'
003 1-3998/88/2403-0333$02.00/0 PEDIATRIC RESEARCH Vol. 24, No. 3, 1988 Copyright O 1988 International Pediatric Research Foundation, Inc. Printed in U.S.A. Renal Effects of Atrial Natriuretic Peptide Infusion in Young and Adult ~ats' ROBERT L. CHEVALIER, R. ARIEL GOMEZ, ROBERT M. CAREY, MICHAEL J. PEACH, AND JOEL M. LINDEN WITH THE TECHNICAL ASSISTANCE OF CATHERINE E. JONES, NANCY V. RAGSDALE, AND BARBARA THORNHILL Departments of Pediatrics [R.L.C., A.R.G., C.E.J., B. T.], Internal Medicine [R.M.C., J.M. L., N. V.R.], Pharmacology [M.J.P.], and Physiology [J.M.L.], University of Virginia, School of Medicine, Charlottesville, Virginia 22908 ABSTRAm. The immature kidney appears to be less GFR, glomerular filtration rate responsive to atrial natriuretic peptide (ANP) than the MAP, mean arterial pressure mature kidney. It has been proposed that this difference UeC~pV,urinary cGMP excretion accounts for the limited ability of the young animal to UN,V, urinary sodium excretion excrete a sodium load. To delineate the effects of age on the renal response to exogenous ANP, Sprague-Dawley rats were anesthetized for study at 31-32 days of age, 35- 41 days of age, and adulthod. Synthetic rat A* was infused intravenously for 20 min at increasing doses rang- By comparison to the adult kidney, the immature kidney ing from 0.1 to 0.8 pg/kg/min, and mean arterial pressure, responds to volume expansion with a more limited diuresis and glomerular filtration rate, plasma ANP concentration, natriuresis (I). A number of factors have been implicated to urine flow rate, and urine sodium excretion were measured explain this phenomenon in the neonatal kidney, including a at each dose. -

Impaired Tubular Secretion of Organic Solutes in Acute Kidney Injury
Original Investigation Impaired Tubular Secretion of Organic Solutes in Acute Kidney Injury Frank J. O’Brien,1 Robert D. Mair,2,3 Natalie S. Plummer,2,3 Timothy W. Meyer,2,3 Scott M. Sutherland,4 and Tammy L. Sirich2,3 Abstract Background Impairment of kidney function is routinely assessed by measuring the accumulation of creatinine, an organic solute cleared largely by glomerular filtration. We tested whether the clearance of solutes that undergo tubular secretion is reduced in proportion to the clearance of creatinine in humans with AKI. Methods Four endogenously produced organic solutes (phenylacetylglutamine [PAG], hippurate [HIPP], indoxyl sulfate [IS], and p-cresol sulfate [PCS]) were measured in spot urine and plasma samples from ten patients with AKI and 17 controls. Fractional clearance relative to creatinine was calculated to assess tubular secretion. Fractional clearance values were calculated in terms of the free, unbound levels of HIPP, IS, and PCS that bind to plasma proteins. Results Fractional clearance values for PAG, HIPP, IS, and PCS were .1.0 in patients with AKI as well as controls, indicating that these solutes were still secreted by the tubules of the injured kidneys. Fractional clearance values were, however, significantly lower in patients with AKI than controls, indicating that kidney injury reduced tubular secretion more than glomerular filtration (AKI versus control: PAG, 2.160.7 versus 4.661.4, P,0.001; HIPP, 1065 versus 1567, P50.02; IS, 1066 versus 2867, P,0.001; PCS, 3.361.8 versus 1063, P,0.001). Free plasma levels rose out of proportion to total plasma levels for each of the bound solutes in AKI, so that calculating their fractional clearance in terms of their total plasma levels failed to reveal their impaired secretion. -

Urate-2- C Transport in the Rat Nephron
Urate-2-14C transport in the rat nephron Ronald A. Kramp, … , William E. Lassiter, Carl W. Gottschalk J Clin Invest. 1971;50(1):35-48. https://doi.org/10.1172/JCI106482. Research Article Intrarenal transport of urate-2-14C was studied in anesthetized rats using the microinjection technic. During saline diuresis, small volumes of urate-2-14C (0.24-0.48 mM) and inulin-3H were injected into surface proximal and distal convoluted tubules, and ureteral urine was collected serially. Total (74-96%) and direct (57-84%) urate recovery increased significantly the more distal the puncture site. Delayed recovery (±20%) remained approximately the same regardless of localization of the microinjection. After proximal injections, total and direct recoveries of urate-2-14C were significantly higher in rats treated with probenecid, pyrazinoate, or PAH than during saline diuresis alone, while the excretion rates were comparable after distal injection. Delayed recovery was not altered by drug administration. The decreased proximal reabsorption of urate is presumably due to an effect of the drugs on the luminal membrane of the nephron. For perfusion at high urate concentrations, nonradioactive urate was added to the injectate (0.89-1.78 mM). Urate-2-14C recovery was almost complete and there was no delayed excretion, demonstrating saturation kinetics. These findings are compatible with a carrier-mediated mechanism for urate transport probably located at the luminal border of the proximal tubular epithelium. No definitive evidence for urate secretion was found in these studies. Find the latest version: https://jci.me/106482/pdf Urate-2-14C Transport in the Rat Nephron RONALD A. -

Production of Hypertonic Urine in the Absence of Pituitary Antidiuretic Hormone
Production of Hypertonic Urine in the Absence of Pituitary Antidiuretic Hormone Robert W. Berliner, Douglas G. Davidson J Clin Invest. 1957;36(10):1416-1427. https://doi.org/10.1172/JCI103541. Research Article Find the latest version: https://jci.me/103541/pdf PRODUCTION OF HYPERTONIC URINE IN THE ABSENCE OF PITUITARY ANTIDIURETIC HORMONE 1 BY ROBERT W. BERLINER AND DOUGLAS G. DAVIDSON 2 (From the Laboratory of Kidney and Electrolyte Metabolism, National Heart Institute, National Institutes of Health, Public Health Sertice, Department of Health, Education, and Welfare, Bethesda, Md.) (Submitted for publication May 1, 1957; accepted May 23, 1957) The mechanism by which pituitary antidiuretic permeability of the tubule membrane to water. hormone (ADH) produces its renal effect has The change to hypertonicity cannot be so readily not been clearly established. Under ordinary con- attributed to an effect on water permeability with- ditions, in the absence of ADH, urine of a con- out some assumptions as to the mechanism by centration considerably below that of plasma is which the hypertonicity is produced. However, produced in large volume. With increasing it is a reasonable hypothesis that the mechanism amounts of ADH, administered or secreted, the for the production of hypertonicity is not depen- osmotic pressure of the urine rises to and above dent upon ADH but that its effects are unmasked, that of plasma. With respect to total water bal- in the presence of ADH, by 1) changes in the vol- ance, the quantitatively more important contri- ume and concentration of urine delivered to it and, bution to water economy is the change between possibly, 2) changes in the permeability of the maximally dilute and isotonic urine, since this, in membranes separating the concentrating mecha- normal man, may involve a change in water ex- nism from the urine in the tubule lumen. -

A Compendium of Research
NASA TECHNICAL NASA TM X-3308 MEMORANDUM CO CO I X c PHYSIOLOGIC RESPONSES TO WATER IMMERSION IN MAN: A COMPENDIUM OF RESEARCH James Kollias, Dena Van Derveer, Karen J. Dorchak, and John E. Greenleaf Ames Research Center Moffett Field, Calif. 94035 ^ *" /V NATIONAL AERONAUTICS AND SPACE ADMINISTRATION • WASHINGTON, D. C. • FEBRUARY 1976 1. Report No. 2. Government Accession No. 3. Recipient's Catalog No. NASA TM X-3308 4. Title and Subtitle 5. Report Date February 1976 PHYSIOLOGIC RESPONSES TO WATER IMMERSION IN MAN: 6. Performing Organization Code A COMPENDIUM OF RESEARCH 7. Author(s) 8. Performing Organization Report No. A-6038 James Kollias, Dena Van Derveer, Karen J. Dorchak, and John E. Greenleaf 10. Work Unit No. 9. Performing Organization Name and Address 970-21-14-05 NASA Ames Research Center 11. Contract or Grant No. Moffett Field, Calif. 94035 13. Type of Report and Period Covered 12. Sponsoring Agency Name and Address Technical Memorandum National Aeronautics and Space Administration 14. Sponsoring Agency Code Washington, D. C. 20546 15. Supplementary Notes 16. Abstract Since the advent of space flight programs, scientists have been searching for ways to reproduce the zero-gravity effects of weightlessness. Brief periods of weightlessness up to 1 minute were feasible using Keplerian trajectory, but comprehen- sive study of the prolonged effects of the weightless state necessitated the development of other methods. Thus far the two approaches most widely used have been complete bedrest and fluid immersion. Surprisingly, these simulated environments have produced essentially all of the symptoms found in astronauts. This compendium contains reports appearing in the literature through December 1973. -

Renal Function in Mice: Effects of Volume Expansion and Angiotensin II
J Am Soc Nephrol 10: 2631–2636, 1999 Renal Function in Mice: Effects of Volume Expansion and Angiotensin II LUDEK CERVENKA,* KENNETH D. MITCHELL,† and L. GABRIEL NAVAR† *Department of Experimental Medicine, Institute for Clinical and Experimental Medicine, Prague, Czech Republic; and †Department of Physiology, Tulane University School of Medicine, New Orleans, Louisiana. Abstract. The present study was performed to validate a simple (83 6 2 mmHg), but led to significantly greater values in both means for assessing renal function in anesthetized mice and to GFR and RPF (1.35 6 0.14 versus 1.01 6 0.1 ml/min z g and characterize the renal hemodynamic responses to acute volume 11.26 6 1.39 versus 6.29 6 0.5 ml/min z g, respectively). expansion and how these responses are altered by concurrent Infusion of AngII during volume expansion led to significant angiotensin II (AngII) infusions. Inulin and para-aminohippu- elevations of MAP (100 6 3 mmHg, P , 0.05) and prevented rate clearances were used to assess GFR and renal plasma flow the increases in GFR and RPF elicited by volume expansion (RPF) in three groups of male C57Bl/6 mice anesthetized with (0.77 6 0.08 and 5.35 6 0.48 ml/min z g, respectively). inactin (100 mg/kg, intraperitoneally) and ketamine (10 mg/ Volume expansion also elicited marked increases in absolute kg). To avoid the hypotension associated with repeated blood and fractional sodium excretion (6.1 6 1.0 versus 0.62 6 0.2 sampling, a single blood sample was taken after three timed mEq/min z g and 3.1 6 0.7 versus 0.4 6 0.1%, respectively). -

Atrial Natriuretic Peptide and Blood Volume During Red Cell Transfusion
Archives ofDisease in Childhood 1991; 66: 395-397 395 Atrial natriuretic peptide and blood volume during Arch Dis Child: first published as 10.1136/adc.66.4_Spec_No.395 on 1 April 1991. Downloaded from red cell transfusion in preterm infants W Rascher, N Lingens, M Bald, 0 Linderkamp Abstract 1710 g (range 650-2660). All infants were in Because raised plasma concentrations of good clinical condition. Four were mechanically atrial natriuretic peptide indicate volume ventilated through an intratracheal tube. None expansion, we studied the effect of red cell had renal disease, shock, sepsis or were being transfusion on plasma atrial natriuretic pep- treated with diuretics. The volume of trans- tide concentration, packed cell volume, and fused red cells was calculated to raise the packed intravascular volume in eight preterm infants. cell volume to 0-45 (haemoglobin to 155 g/l). Red cell transfusion increased red cell mass, The transfusion rate averaged 0-05 (0 01) packed cell volume and erythrocyte count, ml/min/kg. but decreased plasma volume. Total blood Before and one hour after red cell transfusion volume, plasma atrial natriuretic peptide con- blood was drawn in EDTA coated tubes (1 5-2 centration, urine flow rate, and urinary ml) for determination of plasma atrial natriur- sodium excretion did not change. etic peptide and haemoglobin concentrations We conclude that a slow transfusion of packed cell volume, haemoglobin F concentra- less than 10 ml red cells/kg body weight does tion, and plasma osmolality. In addition 0 5 ml not cause volume expansion with subsequent blood was drawn in plastic tubes for measure- atrial natriuretic peptide release thereby ment of serum sodium, potassium and creati- affecting the cardiovascular system. -

Hypernatremia Due to Urea-Induced Osmotic Diuresis: Physiology at The
Educational Forum Hypernatremia due to Urea-Induced Osmotic Diuresis: Physiology at the Bedside Sonali Vadi, Kenneth Yim1 Private Practitioner, Mumbai, Maharashtra, India, 1Director of Inpatient Hemodialysis‑Davita Dialysis, University of Maryland Midtown Campus, Maryland, USA Abstract Hypernatremia secondary to urea‑induced solute diuresis is due to the renal excretion of electrolyte‑free water. This concept is explained here step‑wise physiologically with the help of a clinical vignette. Keywords: Electrolyte‑free water clearance, hypernatremia, hypertonicity, osmotic diuresis, urea BACKGROUND Her initial laboratory data are presented in Table 1 and electrolyte trends during the hospital stay are summarized in Equation between solutes and water determines serum sodium Table 2. levels. Increased urinary solute load in the form of urea nitrogen leads to urea‑induced osmotic diuresis with increased Acute issues at hand free water loss and ensued hypernatremia. Diagnostic 1. What is the cause of her renal dysfunction? CLINICAL VIGNETTE 2. Why is she hypernatremic? A 70‑year‑old woman was found unconscious at home. As Treatment per her family members, she complained of abdominal pain 1. Should she be urgently dialyzed? and diarrhea for 1 week’s duration. Her baseline mental 2. How should her hypernatremia be managed? status was noted to be alert and oriented three days prior to presentation. Her medical history was significant for DISCUSSION hypertension and osteoarthritis. There was no prior history of renal dysfunction. She has been a heavy alcohol drinker. This complex pathological situation has been de‑coded Her medications included ibuprofen and cyclobenzaprine step‑wise in a question format, with answers to each in two for osteoarthritis; lisinopril and felodipine for hypertension; parts. -

The Use of Selected Urine Chemistries in the Diagnosis of Kidney Disorders
CJASN ePress. Published on January 9, 2019 as doi: 10.2215/CJN.10330818 The Use of Selected Urine Chemistries in the Diagnosis of Kidney Disorders Biff F. Palmer1 and Deborah Joy Clegg2 Abstract Urinary chemistries vary widely in both health and disease and are affected by diet, volume status, medications, and disease states. When properly examined, these tests provide important insight into the mechanism and therapy of 1Division of various clinical disorders that are first detected by abnormalities in plasma chemistries. These tests cannot be Nephrology, interpreted in isolation, but instead require knowledge of key clinical information, such as medications, physical Department of examination, and plasma chemistries, to include kidney function. When used appropriately and with knowledge of Medicine, University of Texas Southwestern limitations, urine chemistries can provide important insight into the pathophysiology and treatment of a wide Medical Center, variety of disorders. Dallas, Texas; and Clin J Am Soc Nephrol 14: ccc–ccc, 2019. doi: https://doi.org/10.2215/CJN.10330818 2Department of Internal Medicine, University of California, Los Introduction values ,15 mEq/L. On the other hand, volume Angeles School of Urine chemistries can provide valuable insight into a expansion suppresses effector mechanisms and stimu- Medicine, Los wide range of clinical conditions. These tests are often lates release of atrial natriuretic peptide, leading to a Angeles, California underutilized because of the difficulty many physi- reduction in sodium reabsorption, causing urinary so- Correspondence: cians find in their interpretation. Whereas a basic dium concentration to be high. Thus, the urine sodium fi Dr. Biff F. Palmer, metabolic pro le obtained from a blood sample has concentrationisanindirectmeasureofvolumestatusand Department of Internal well defined normal values, there are no such values reflects the integrity of the kidney to regulate that status. -

A Didactic Approach to Renal Clearance
A Didactic Approach to Renal Clearance Vander Baptista, PhD Department of Physiological Sciences, Centre of Biological Sciences, Federal University of Santa Catarina, 88040-970 Florianópolis, SC – Brazil [email protected] Abstract Renal clearance encompasses a somewhat abstract concept, which makes it a hard-to-visualize phenomenon. It is a confusing topic for students and a difficult task for the instructor to teach. In order to improve or facilitate the teaching-learning process of renal clearance, an alternative strategy is presented here. To properly characterize the components of renal clearance, this didactic model splits renal clearance into two distinct portions of flow rates. The information is organized in a sequential structure, from the simplest ideas to the most complex concepts, assisting both teacher and student in addressing renal clearance. https://doi.org/10.21692/haps.2020.022 Key words: renal clearance, didactic model, cumulative sequence, renal physiology, kidney Introduction The clearance methods are a useful way to quantify the The renal excretion rate of a substance S (ERS) is the amount glomerular filtration rate, tubular reabsorption, and tubular of S removed from the body by the kidneys per unit of time secretion (Hall and Guyton 2011). In a broader vision, as (mg/min). By using the same reasoning, it can be written pointed out by Dr. Donald W. Seldin: “The clearance concept ERS = x US, where is the urinary excretion rate (urinary is central to three critical areas of nephrology”; it was a key volume per unit of time) and US is the concentration of S in feature for understanding the nature of urine formation, for the urine. -

Atrial Natriuretic Peptide and Furosemide Effects on Hydraulic Pressure in the Renal Papilla
Kidney International, Vol. 34 (1988), pp. 36—42 Atrial natriuretic peptide and furosemide effects on hydraulic pressure in the renal papilla RAMON E. MENDEZ, B. RENTZ DUNN, JULIA L. TROY, and BARRY M. BRENNER The Harvard Center for the Study of Kidney Diseases, Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts, USA Atrial natriuretic peptide and furosemide effects on hydraulic pressure pre-renal arterial clamping prior to, or during, ANP administra- in the renal papilla. Atrial peptides (ANP) have been shown to prefer- tion has been shown to markedly blunt or abolish the natriuresis entially increase blood flow tojuxtamedullary nephrons and to augment vasa recta blood flow. To determine the effect of this alteration in[1,9,4]. Since clamping also prevented an ANP-induced rise in intrarenal blood flow distribution on pressure relationships in innerGFR, the enhancement of GFR by ANP was felt to be a primary medullary structures and their significance as a determinant of ANP- factor responsible for its natriuretic effect [11. However, several induced natriuresis, we measured hydraulic pressures in vascular and studies have demonstrated increases in renal sodium excretion tubule elements of the renal papilla exposed in Munich-Wistar rats in in the absence of discernable changes in whole kidney hemo- vivo during an euvolemic baseline period and again during an experi- mental period. Rats in Group 1 received intravenous infusion of rANP dynamics [6, 7, 10]. On the other hand, an additional hemody- [4-27], administered as a 4 sg/kg prime and 0.5 gIkg/min continuous namic mechanism which might be operative lies in the renal infusion, and were maintained euvolemic by plasma replacement.vasodilatory properties of ANP, in particular its ability to Infusion of ANP resulted in significant natriuresis, diuresis and increase increase vasa recta blood flow [11, 10].