Humanitarian Bulletin Occupied Palestinian Territory MARCH 2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Good Samaritan Inn 55 NATIONAL PARKS and NATURE Mosaic Museum RESERVES
BUY AN ISRAEL NATURE AND PARKS AUTHORITY SUBSCRIPTION FOR UNLIMITED FREE ENTRY TO The Good Samaritan Inn 55 NATIONAL PARKS AND NATURE Mosaic Museum RESERVES. A lioness from the Gaza mosaic Rules of Conduct ■ Do not harm the antiquities: Do not carve on them, walk on them or pour water on them. ■ Do not collect “souvenirs” from remains scattered in the area. ■ Do not enter places that are off-limits for visitors. Nearby Sites: ■ Do not cross fences or roll stones. ■ Please keep the area clean. Qumran Location of the Good Samaritan Inn Mosaic Museum National Park about 25 minutes’ drive The museum is on the southern side of the Jerusalem–Jericho road (road 1) between kilometer markers 80 and 81. The interchange affords easy access from whichever direction you approach. To reserve a guided tour for a group, email: You Enot Tsukim are here Nature Reserve [email protected] about 25 minutes’ drive Hours: Daily from 8:00 to 17:00. En Prat During winter time, the site closes one hour earlier. Nature Reserve On Fridays and holiday eves, the site closes one hour earlier. about 20 minutes’ drive Entry is permitted up to one hour before closing. Text: Ya‘acov Shkolnik Translation: Miriam Feinberg Vamosh 6.18 Photos: Israel Nature and Parks Authority Archive; Ya‘acov Shkolnik; Tal Romano; Amir Aloni Production: Adi Greenbaum www.parks.org.il I *3639 I © Israel Nature and Parks Authority The Good Samaritan Inn, Tel: 02-6338230 established on the initiative of the archaeologist Dr. Yitzhak Welcome to the Magen, who served as the head of the Judea and Samaria Inn of the Good Samaritan Archaeology Unit. -

Protection of Civilians Weekly Report
U N I TOCHA E D Weekly N A Report: T I O 28N FebruaryS – 6 March 2007 N A T I O N S| 1 U N I E S OFFICE FOR THE COORDINATION OF HUMANITARIAN AFFAIRS P.O. Box 38712, East Jerusalem, Phone: (+972) 2-582 9962 / 582 5853, Fax: (+972) 2-582 5841 [email protected], www.ochaopt.org Protection of Civilians Weekly Report 28 February – 6 March 2007 Of note this week The IDF imposed a total closure on the West Bank during the Jewish holiday of Purim between 2 – 5 March. The closure prevented Palestinians, including workers, with valid permits, from accessing East Jerusalem and Israel during the four days. It is a year – the start of the 2006 Purim holiday – since Palestinian workers from the Gaza Strip have been prevented from accessing jobs in Israel. West Bank: − On 28 February, the IDF re-entered Nablus for one day to continue its largest scale operation for three years, codenamed ‘Hot Winter’. This second phase of the operation again saw a curfew imposed on the Old City, the occupation of schools and homes and house-to-house searches. The IDF also surrounded the three major hospitals in the area and checked all Palestinians entering and leaving. According to the Nablus Municipality 284 shops were damaged during the course of the operation. − Israeli Security Forces were on high alert in and around the Old city of Jerusalem in anticipation of further demonstrations and clashes following Friday Prayers at Al Aqsa mosque. Due to the Jewish holiday of Purim over the weekend, the Israeli authorities declared a blanket closure from Friday 2 March until the morning of Tuesday 6 March and all major roads leading to the Old City were blocked. -

Abuses Against Journalists by Palestinian Security Forces WATCH
Occupied Palestinian Territories HUMAN No News is Good News RIGHTS Abuses against Journalists by Palestinian Security Forces WATCH No News is Good News Abuses against Journalists by Palestinian Security Forces Copyright © 2011 Human Rights Watch All rights reserved. Printed in the United States of America ISBN: 1-56432-759-0 Cover design by Rafael Jimenez Human Rights Watch 350 Fifth Avenue, 34th floor New York, NY 10118-3299 USA Tel: +1 212 290 4700, Fax: +1 212 736 1300 [email protected] Poststraße 4-5 10178 Berlin, Germany Tel: +49 30 2593 06-10, Fax: +49 30 2593 0629 [email protected] Avenue des Gaulois, 7 1040 Brussels, Belgium Tel: + 32 (2) 732 2009, Fax: + 32 (2) 732 0471 [email protected] 64-66 Rue de Lausanne 1202 Geneva, Switzerland Tel: +41 22 738 0481, Fax: +41 22 738 1791 [email protected] 2-12 Pentonville Road, 2nd Floor London N1 9HF, UK Tel: +44 20 7713 1995, Fax: +44 20 7713 1800 [email protected] 27 Rue de Lisbonne 75008 Paris, France Tel: +33 (1)43 59 55 35, Fax: +33 (1) 43 59 55 22 [email protected] 1630 Connecticut Avenue, N.W., Suite 500 Washington, DC 20009 USA Tel: +1 202 612 4321, Fax: +1 202 612 4333 [email protected] Web Site Address: http://www.hrw.org April 2011 ISBN: 1-56432-759-0 No News is Good News Abuses against Journalists by Palestinian Security Forces Summary ........................................................................................................................... 1 Background ........................................................................................................................ 3 West Bank ....................................................................................................................... 5 Reports of Increased Harassment ............................................................................. 6 The Role of PA Security Forces ................................................................................... 7 Gaza ............................................................................................................................. -

99.8% of State Lands Allocated in the West Bank Were Given to Israelis; Palestinians Were Given Almost Nothing
State Land Allocation in the West Bank—For Israelis Only, July 2018 99.8% of state lands allocated in the West Bank were given to Israelis; Palestinians were given almost nothing Following a request under the Freedom of Information Act submitted by Peace Now and the Movement for Freedom of Information (and after refusing to give the information and a two-and-a-half year delay), the Civil Administration's response was received: 99.76% (about 674,459 dunams) of state land allocated for any use in the Occupied West Bank was allocated for the needs of Israeli settlements. The Palestinians were allocated, at most, only 0.24% (about 1,625 dunams). Some 80% of the allocations to Palestinians (1,299 dunams) were for the purpose of establishing settlements (669 dunams) and for the forced transfer of Bedouin communities (630 dunams). Only 326 dunams at most were allocated without strings for the benefit of Palestinians, and at least 121 of those dunams are currently in Area B under Palestinian control. Most of the allocations to the Palestinians (about 53%) were made prior to the 1995 Interim Agreement (the Oslo II Agreement, in which the West Bank was divided into Areas A, B and C, and transferred control over 40% of the West Bank to the Palestinian Authority). The High Court of Justice is currently facing the issue of the evacuation of the Palestinian village of Al-Khan al- Ahmar, which the state wants to demolish and expel its residents to another area. The residents of the village are asking the High Court of Justice to stop the evacuation until the Civil Administration discusses the detailed construction plan they prepared for the village's approval, which the state has refused to consider. -
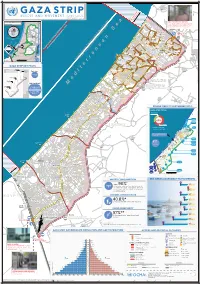
Gaza CRISIS)P H C S Ti P P I U
United Nations Office for the Coordination of Humanitarian Affairs occupied Palestinian territory Zikim e Karmiya s n e o il Z P m A g l in a AGCCESSA ANDZ AMOV EMENTSTRI (GAZA CRISIS)P h c s ti P P i u F a ¥ SEPTEMBER 2014 o nA P N .5 F 1 Yad Mordekhai EREZ CROSSING (BEIT HANOUN) occupied Palestinian territory: ID a As-Siafa OPEN, six days (daytime) a B?week4 for B?3the4 movement d Governorates e e of international workers and limited number of y h s a b R authorized Palestinians including aid workers, medical, P r 2 e A humanitarian cases, businessmen and aid workers. Jenin d 1 e 0 Netiv ha-Asara P c 2 P Tubas r Tulkarm r fo e S P Al Attarta Temporary Wastewater P n b Treatment Lagoons Qalqiliya Nablus Erez Crossing E Ghaboon m Hai Al Amal r Fado's 4 e B? (Beit Hanoun) Salfit t e P P v i Al Qaraya al Badawiya i v P! W e s t R n m (Umm An-Naser) n i o » B a n k a North Gaza º Al Jam'ia ¹¹ M E D I TER RAN EAN Hatabiyya Ramallah da Jericho d L N n r n r KJ S E A ee o Beit Lahia D P o o J g Wastewater Ed t Al Salateen Beit Lahiya h 5 Al Kur'a J a 9 P l D n Treatment Plant D D D D 9 ) D s As Sultan D 1 2 El Khamsa D " Sa D e J D D l i D 0 D s i D D 0 D D d D D m 2 9 Abedl Hamaid D D r D D l D D o s D D a t D D c Jerusalem D D c n P a D D c h D D i t D D s e P! D D A u P 0 D D D e D D D a l m d D D o i t D D l i " D D n . -

Three Conquests of Canaan
ÅA Wars in the Middle East are almost an every day part of Eero Junkkaala:of Three Canaan Conquests our lives, and undeniably the history of war in this area is very long indeed. This study examines three such wars, all of which were directed against the Land of Canaan. Two campaigns were conducted by Egyptian Pharaohs and one by the Israelites. The question considered being Eero Junkkaala whether or not these wars really took place. This study gives one methodological viewpoint to answer this ques- tion. The author studies the archaeology of all the geo- Three Conquests of Canaan graphical sites mentioned in the lists of Thutmosis III and A Comparative Study of Two Egyptian Military Campaigns and Shishak and compares them with the cities mentioned in Joshua 10-12 in the Light of Recent Archaeological Evidence the Conquest stories in the Book of Joshua. Altogether 116 sites were studied, and the com- parison between the texts and the archaeological results offered a possibility of establishing whether the cities mentioned, in the sources in question, were inhabited, and, furthermore, might have been destroyed during the time of the Pharaohs and the biblical settlement pe- riod. Despite the nature of the two written sources being so very different it was possible to make a comparative study. This study gives a fresh view on the fierce discus- sion concerning the emergence of the Israelites. It also challenges both Egyptological and biblical studies to use the written texts and the archaeological material togeth- er so that they are not so separated from each other, as is often the case. -

State of Palestine Humanitarian Situation Report
State of Palestine Humanitarian Situation Report Gaza Strip State of Palestine January – June 2018 water in her home ©UNICEF/ ©UNICEF/ waterSOP/ her in home Eyad El Baba running A her from girl hands is washing Highlights • Since the start of the demonstrations associated with the “Great March of Return” on 1,300,000 # of children affected out of total 2.5m 30th March, 135 people have been killed, including 17 children in Gaza. More than people in need (UN OCHA Humanitarian HRP 15,501 people were injured, 8,221 (53%) of them hospitalized. According to MoH, 2,947 2018) children were injured, comprising 19% of total injures as of 30 June, 2018. • The current deterioration of the situation in Gaza and rising tensions in the West Bank 2,500,000 trigger urgent funding needs for child protection, health, WASH and education # of people in need (UN OCHA Humanitarian HRP 2018) interventions to address the growing humanitarian needs. Only US$ 9.1 million or 36 per cent of the initial requirements was available as of 30 June, 2018. 652,000 • A total of 718 injured children have been supported by Child Protection/Mental Health # of children to be reached and Psychosocial Services (MHPSS) working group members through home visits, and (UNICEF Humanitarian Action for Children 2018) Psychological First Aid; children in need of more specialized care were referred to case management, utilizing the child protection referral pathways. This includes those who 729,000 # of people to be reached have parents, siblings, relatives or friends injured or killed during demonstrations. (UNICEF Humanitarian Action for Children 2018) • Prepositioned essential drugs and medical consumables were released to cover emergency medical care for 111,532 children and their families. -

Palestine About the Author
PALESTINE ABOUT THE AUTHOR Professor Nur Masalha is a Palestinian historian and a member of the Centre for Palestine Studies, SOAS, University of London. He is also editor of the Journal of Holy Land and Palestine Studies. His books include Expulsion of the Palestinians (1992); A Land Without a People (1997); The Politics of Denial (2003); The Bible and Zionism (Zed 2007) and The Pales- tine Nakba (Zed 2012). PALESTINE A FOUR THOUSAND YEAR HISTORY NUR MASALHA Palestine: A Four Thousand Year History was first published in 2018 by Zed Books Ltd, The Foundry, 17 Oval Way, London SE11 5RR, UK. www.zedbooks.net Copyright © Nur Masalha 2018. The right of Nur Masalha to be identified as the author of this work has been asserted by him in accordance with the Copyright, Designs and Patents Act, 1988. Typeset in Adobe Garamond Pro by seagulls.net Index by Nur Masalha Cover design © De Agostini Picture Library/Getty All rights reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical, photocopying or otherwise, without the prior permission of Zed Books Ltd. A catalogue record for this book is available from the British Library. ISBN 978‑1‑78699‑272‑7 hb ISBN 978‑1‑78699‑274‑1 pdf ISBN 978‑1‑78699‑275‑8 epub ISBN 978‑1‑78699‑276‑5 mobi CONTENTS Acknowledgments vii Introduction 1 1. The Philistines and Philistia as a distinct geo‑political entity: 55 Late Bronze Age to 500 BC 2. The conception of Palestine in Classical Antiquity and 71 during the Hellenistic Empires (500‒135 BC) 3. -

Greater Jerusalem” Has Jerusalem (Including the 1967 Rehavia Occupied and Annexed East Jerusalem) As Its Centre
4 B?63 B?466 ! np ! 4 B?43 m D"D" np Migron Beituniya B?457 Modi'in Bei!r Im'in Beit Sira IsraelRei'ut-proclaimed “GKharbrathae al Miasbah ter JerusaBeitl 'Uer al Famuqa ” D" Kochav Ya'akov West 'Ein as Sultan Mitzpe Danny Maccabim D" Kochav Ya'akov np Ma'ale Mikhmas A System of Settler-Colonialism and Apartheid Deir Quruntul Kochav Ya'akov East ! Kafr 'Aqab Kh. Bwerah Mikhmas ! Beit Horon Duyuk at Tahta B?443 'Ein ad D" Rafat Jericho 'Ajanjul ya At Tira np ya ! Beit Liq Qalandi Kochav Ya'akov South ! Lebanon Neve Erez ¥ ! Qalandiya Giv'at Ze'ev D" a i r Jaba' y 60 Beit Duqqu Al Judeira 60 B? a S Beit Nuba D" B? e Atarot Ind. Zone S Ar Ram Ma'ale Hagit Bir Nabala Geva Binyamin n Al Jib a Beit Nuba Beit 'Anan e ! Giv'on Hahadasha n a r Mevo Horon r Beit Ijza e t B?4 i 3 Dahiyat al Bareed np 6 Jaber d Aqbat e Neve Ya'akov 4 M Yalu B?2 Nitaf 4 !< ! ! Kharayib Umm al Lahim Qatanna Hizma Al Qubeiba ! An Nabi Samwil Ein Prat Biddu el Almon Har Shmu !< Beit Hanina al Balad Kfar Adummim ! Beit Hanina D" 436 Vered Jericho Nataf B? 20 B? gat Ze'ev D" Dayr! Ayyub Pis A 4 1 Tra Beit Surik B?37 !< in Beit Tuul dar ! Har A JLR Beit Iksa Mizpe Jericho !< kfar Adummim !< 21 Ma'ale HaHamisha B? 'Anata !< !< Jordan Shu'fat !< !< A1 Train Ramat Shlomo np Ramot Allon D" Shu'fat !< !< Neve Ilan E1 !< Egypt Abu Ghosh !< B?1 French Hill Mishor Adumim ! B?1 Beit Naqquba !< !< !< ! Beit Nekofa Mevaseret Zion Ramat Eshkol 1 Israeli Police HQ Mesilat Zion B? Al 'Isawiya Lifta a Qulunyia ! Ma'alot Dafna Sho'eva ! !< Motza Sheikh Jarrah !< Motza Illit Mishor Adummim Ind. -

JPS189 15 Chronology 1..41
Chronology 16 MAY–15 AUGUST 2018 COMPILED BY PAUL KAROLYI This is part 139 of a chronology begun in JPS 13, no. 3 (Spring 1984). Chronology dates reflect North American Eastern Standard Time. For a more comprehensive overview of regional and international developments related to Israel and the Palestinians, see the quarterly Update on Conflict and Diplomacy in JPS 48 (1). 16 MAY 2018 approximately 400 grapevines in a Palestinian Along Gaza’sborderfence, unidentified vineyard near Hebron. In East Jerusalem, Palestinians open fire on Israel Defense Israeli forces arrest 4 Palestinians during a Forces (IDF) patrols near Jabaliya refugee raid in Silwan. (WAFA 5/16; HA, JP, TOI, camp causing no injuries. Israeli tanks then YA 5/17; PCHR 5/17; PCHR 5/24) shell several Hamas posts near the border Guatemalan president Jimmy Morales and fence, causing damage. Later, Palestinians fire Israeli PM Benjamin Netanyahu attend the machinegunsacrosstheborderintoIsrael, inauguration of the new Guatemalan embassy this time causing minor damage to an Israeli in Jerusalem. “My next trip through Latin home near Sderot. The IDF then bombs America goes through Guatemala,” Netanyahu Hamas sites in northern Gaza, including an says. (HA, JP, TOI, YA 5/16) alleged weapons production facility, causing The Egyptian authorities keep the Rafah an unclear amount of damage (see Update). border crossing open for the fourth consecutive Separately, IDF troops violently disperse day, despite their initial plans to keep it closed Palestinians gathering along the border fence today (see Update). (AP 5/18) to protest and throw stones near al-Bureij refugee camp, Gaza City, and Khan Yunis; 4 Palestinians are injured. -

Emergency Humanitarian Aid Decision Budget Line – 23 02 01
EUROPEAN COMMISSION HUMANITARIAN AID OFFICE (ECHO) Emergency Humanitarian Aid Decision Budget Line – 23 02 01 Title: Commission decision concerning an emergency humanitarian aid decision in favor of the population of the occupied Palestinian territories affected by house demolitions. Location of operation: occupied Palestinian territories, Gaza Strip, Rafah. Amount of Decision: Euro 1 million. Decision reference number: ECHO/PSE/BUD/2004/01000 Explanatory Memorandum 1 - Rationale, needs and target population. 1.1. - Rationale: Between 16 and 22 January 2004 the Israeli Defence Forces (IDF) carried out extensive demolition and land levelling in the Palestinian refugee camp in Rafah, in the southern Gaza Strip. On 16 January, 17 buildings1, home to 170 people, were demolished. In the night and morning of 20 January a further 36 homes were destroyed, leaving 414 people homeless. Early morning on 22 January a third incursion resulted in another four demolished homes. This assault saw a 31-year old Palestinian woman killed and eight other Palestinians injured. The IDF states that these operations were undertaken following the “discovery of a weapon smuggling tunnel (as well as a tunnel filled with explosive)”. IDF forces “demolished a number of abandoned structures concealing tunnel entry shafts along the Israel-Egypt border, in the Rafah area. The abandoned structures were demolished to halt weapon smuggling and terrorist activity against IDF forces and Israeli civilians”. There is no information available concerning eventual action taken by the Government of Israel towards the Egyptian authorities in relation to the alleged tunnels along the border separating the Gaza Strip from Egypt. Satellite pictures taken by the European Commission’s Joint Research Centre and the European Union Satellite Centre, and made available by the United Nations Office for the Co-ordination of Humanitarian Affairs (OCHA), clearly show the magnitude of the house demolitions taking place in Rafah. -
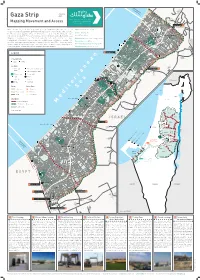
Gaza Strip 2020 As-Siafa Mapping Movement and Access Netiv Ha'asara Temporary
Zikim Karmiya No Fishing Zone 1.5 nautical miles Yad Mordekhai January Gaza Strip 2020 As-Siafa Mapping Movement and Access Netiv Ha'asara Temporary Ar-Rasheed Wastewater Treatment Lagoons Sources: OCHA, Palestinian Central Bureau of Statistics of Statistics Bureau Central OCHA, Palestinian Sources: Erez Crossing 1 Al-Qarya Beit Hanoun Al-Badawiya (Umm An-Naser) Erez What is known today as the Gaza Strip, originally a region in Mandatory Palestine, was created Width 5.7-12.5 km / 3.5 – 7.7 mi through the armistice agreements between Israel and Egypt in 1949. From that time until 1967, North Gaza Length ~40 km / 24.8 mi Al- Karama As-Sekka the Strip was under Egyptian control, cut off from Israel as well as the West Bank, which was Izbat Beit Hanoun al-Jaker Road Area 365 km2 / 141 m2 Beit Hanoun under Jordanian rule. In 1967, the connection was renewed when both the West Bank and the Gaza Madinat Beit Lahia Al-'Awda Strip were occupied by Israel. The 1993 Oslo Accords define Gaza and the West Bank as a single Sheikh Zayed Beit Hanoun Population 1,943,398 • 48% Under age 17 July 2019 Industrial Zone Ash-Shati Housing Project Jabalia Sderot territorial unit within which freedom of movement would be permitted. However, starting in the camp al-Wazeer Unemployment rate 47% 2019 Q2 Jabalia Camp Khalil early 90s, Israel began a gradual process of closing off the Strip; since 2007, it has enforced a full Ash-Sheikh closure, forbidding exit and entry except in rare cases. Israel continues to control many aspects of Percentage of population receiving aid 80% An-Naser Radwan Salah Ad-Deen 2 life in Gaza, most of its land crossings, its territorial waters and airspace.