Interim Meeting Minutes
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Northern Sights Newsletter
Northern Sights Newsletter North Dakota Vol. 30 Issue 4 August 2018 Optometric Association President’s Message ~ Dr. Darin Johnson 921 South 9th Street, Ste. 120 Bismarck, ND 58504 Phone: 701-258-6766 Wow, summer is Secondly, we are working on the health Fax: 701-258-9005 flying by. I hope eve- care trust. This could be a great option for E-mail: [email protected] ryone has had the our members to have a potential cost saving Website: www.ndeyecare.com opportunity to get out alternative for reliable health insurance. and enjoy the beauti- Nancy has been working hard to make sure 2018 NDOA OFFICERS ful North Dakota we can offer this benefit, and keep it afforda- Dr. Darin Johnson weather. I feel as if ble for our members and their employees. time is slipping by, President Lastly, I am working on a more consistent and I have not accom- 1525 31st Ave. SW, Ste. E and repeatable sponsorship form. There is plished much for the Minot, ND 58701 some stress about our questionable future of NDOA this summer, 701-857-6050 sponsorship, and support from members in but we have many irons in the fire. We [email protected] our industry. It is our obligation as optome- would like to say thank you to our members trists to make sure we recognize our spon- Dr. Nate Shilman who were able to make the NDOA spon- sors, and thank them for their continued sup- President Elect sored golf outing in Bismarck. It was a suc- port of the NDOA. Please speak to all your 2273 3rd Ave West cess as far as the number of attendees, and Dickinson, ND 58601 vendors, and always mention how much we we always have great sponsorship for this 701-225-7886 appreciate their continued support and en- event. -
~""'->" class="text-overflow-clamp2"> H~,Iassi.. ".'~ }:;Ei:U;Ii"1>~""'->
11.. _II!III'Il!!IB'!!77,,="I:7r=m·!=== ..... ~ _. • • communi ty 16 I Griggs County Courier October 26, 2018 LEGAL NOTICES October s, 2018 24513 John Deere Financial 514.64 COMMISSIONERS PROCEEDINGS 24514 Kelly Printing Supplies The Board of County 122.95 Commissioners met in regular 24515 Samantha M Larson 72.00 session on Friday, October 5.2018 24516 NAACTFOTreasurer 75.00 at 1:00 pm. 24517 Napa Auto Parts 53.47 Chairman Olson opened the 24518 NO Attorney General 465.00 meeting and asked everyone to 24519 NDACO 445.61 stand for the Pledge of Allegiance. 24520 NDLTAP/UGPTI25.00 Chairman Olson took roll call 24521 NO Secretary of State and present were Commissioners 1005.98 Wakefield, Pedersen, Urness, 24522 NetCenter Supply 285.80 Steffen, and Olso n. Also present 24523 New Century Press 76.11 were Road Superintendent/911 24524 Ottertail Power Co 1206.11 Coordinator Oien, Treasurer 24525 ROOEquipment Co 2449.12 Eslinger, Clerk of Court Vincent, 24526 Reiten Inc 50.46 Extension AgentVig, & Tax Director 24527 State Treasurer 1643.45 Lunde. 24528 T and K Sales 2678.49 Chairman Olson opened 24529 Verizon Wireless 289.66 the floor for any changes to the 24530 Madison Wallace 72.00 agenda. Motion by Pedersen to 24531-24541 CWB 36547.1 0 accept the age nda as prese nted, 24542-24543 Cities/Townships second by Steffen and called fo r 7975.23 discussion three times with all 24554-24556 Schools 7472.27 ayes, no nays, and carried. 24557 Com Medical Center Hosp Chairman Olson opened the Dist 612.20 Please join us in voting for Kevin Cramer for U.S. -

MCF Contribution Report July 1
MCF CONTRIBUTIONS JULY 1 - DECEMBER 31, 2018 Name State Candidate Amount Party Total U.S. Senate Sinema For Arizona AZ Sen. Kyrsten Sinema $2,500 DEM ARIZONA TOTAL $2,500 U.S. House Jim Costa For Congress CA Rep. Jim Costa $1,000 DEM CALIFORNIA TOTAL $1,000 U.S. House Al Lawson For Congress FL Rep. Al Lawson $2,000 DEM FLORIDA TOTAL $2,000 U.S. Senate Leadership Joni For Iowa IA Sen. Joni Ernst $2,500 REP U.S. House Loebsack For Congress IA Rep. Dave Loebsack $2,500 DEM Young For Iowa, Inc. IA David Young $1,500 REP Young For Iowa, Inc. IA David Young $2,500 REP Governor Kim Reynolds for Iowa IA Gov. Kim Reynolds $7,500 REP Agriculture Secretary Mike Naig for Iowa Agriculture IA Sec. Mike Naig $5,000 REP Mike Naig for Iowa Agriculture IA Sec. Mike Naig $5,000 REP State Senate Schneider for State Senate IA Sen. Charles Schneider $2,500 REP Citizens to Elect Bill Dotzler IA Sen. Bill Dotzler $1,000 DEM Kevin Kinney for State Senate IA Sen. Kevin Kinney $1,000 DEM Dan Zumbach for Senate IA Sen. Dan Zumbach $2,000 REP Kraayenbrink for Iowa Senate IA Sen. Tim Kraayenbrink $500 REP Tom Shipley for Iowa IA Sen. Tom Shipley $750 REP Amanda Ragan for Iowa Senate IA Sen. Amanda Ragan $750 DEM Friends of Whitver IA Sen. Jack Whitver $3,500 REP Sweeney for Senate IA Sen. Annette Sweeney $1,000 REP Kapucian for State Senate IA Sen. Tim Kapucian $750 REP Friends for Zach Nunn IA Sen. -

FORMATTING- Networker Spring 2017.Indd
The Volume 31, Issue 1 Spring 2017 Networker Newsletter of Catholic Charities North Dakota Celebrating 30 Years of Guardianship Services at Catholic Charities North Dakota The Guardianship Division at Catholic Charities North Dakota is celebrating its 30th anniversary of service. As a result of the ARC lawsuit in 1980, many people with intellectual disabilities began moving from the state institution in Grafton to community based services throughout North Dakota. It was found that a number of people were ready to move but needed the support of a guardian to help make informed decisions on their behalf. The Department of Human Services issued a Request for Proposal in the mid-1980’s asking that a program be developed which would serve as corporate guardians for individuals who Paul Griffin, former Director of Guardianship Services, and RogerSchwinghammer, did not have family or friends available former Executive Director, are shown in this file photo from 1998. Paul and Roger to be their guardian. In 1986, our agency were instrumental in the development of the Guardianship program for Adults with was awarded the contract because Roger Intellectual Disabilities. Schwinghammer, Executive Director, had the vision and belief that this program fit the mission of Catholic Charities North Dakota. Paul Griffin became the Supervisor of the Guardianship Program and he brought this vision to life. Paul started with a blank slate as there were no programs of this nature in North Dakota and he developed all of the policies and procedures. Under Paul’s leadership, a program was built that is based on integrity, advocacy, compassion and quality of service where the best interest of the person is paramount. -

House of Rep Daily Journal
Page 2285 1st DAY TUESDAY, AUGUST 2, 2016 2285 JOURNAL OF THE HOUSE - SPECIAL SESSION Sixty-fourth Legislative Assembly * * * * * Bismarck, August 2, 2016 The House convened at 9:00 a.m., with Speaker Belter presiding. The prayer was offered by Prayer by Reverend Rich Wyatt, Living Hope Church of the Nazarene. The roll was called and all members were present except Representatives Glassheim, Holman, Skarphol, and Wallman. A quorum was declared by the Speaker. OATH OF OFFICE CHIEF JUSTICE GERALD W. VANDEWALLE ADMINISTERED the Oath of Office to newly appointed Representative Greg Westlind. COMMUNICATION FROM SECRETARY OF STATE AL JAEGER I hereby certify that I have attached a true and correct copy of Executive Order 2016-03, executed by Governor Jack Dalrymple on July 13, 2016, in which he convenes the North Dakota Legislative Assembly into special session on Tuesday, August 2, 2016, at 9:00 a.m. I hereby certify that I have attached a true and correct listing of Representatives who were issued Certificates of Election by the State Canvassing Board prior to the beginning of their respective terms of office and who continue to serve, as of this date, in the legislative district to which they were elected. I hereby certify that on July 25, 2016, I issued a Certificate of Appointment to Greg Westlind for the House vacancy in Legislative District No. 15, executed according to Section 16.1-13- 10 of the North Dakota Century Code and whose name is included on the attached list. IN TESTIMONY WHEREOF, I have set my hand and affixed the Great Seal of the State of North Dakota at the Capitol in the City of Bismarck on this date. -

North Dakota United Announces 2018 Legislative Endorsements
NEWS RELEASE For Release: For More Information, Contact: Feb. 28, 2018 Kelly Hagen Communications Director North Dakota United Phone: 701-223-0450 E-mail: [email protected] North Dakota United Announces 2018 Legislative Endorsements BISMARCK, N.D. – North Dakota United is proud to endorse the following North Dakota state legislators for re-election in 2018. “Their advocacy and support of legislation to strengthen our great public schools, higher education and outstanding public service over the past two legislative sessions is something of which they can be very proud,” said NDU President Nick Archuleta. “Their willingness to work together, regardless of political persuasion, to find solutions to challenges is inspiring and much appreciated by our members and the people of North Dakota.” Representative Andy Maragos (R-3) Senator Nicole Poolman (R-7) Representative Tracy Boe (D-9) Representative Marvin Nelson (D-9) Senator Richard Marcellais (D-9) Representative Gretchen Dobervich (D-11) Representative Ron Guggisberg (D-11) Senator Tim Mathern (D-11) Senator Judy Lee (R-13) Senator Dave Oehlke (R-15) Representative Greg Westlind (R-15) Senator Ray Holmberg (R-17) Representative Kathy Hogan (D-21) for Senate Representative Mary Schneider (D-21) Senator Joan Heckaman (D-23) Representative Alisa Mitskog (D-25) Representative Tom Beadle (R-27) for Senate Representative Bob Martinson (R-35) 301 N. Fourth St., Bismarck, ND 58501 Phone: 701-223-0450 or 800-369-6332 E-mail: [email protected] Visit us online at www.ndunited.org Facebook: www.facebook.com/ndunited Twitter: www.twitter.com/ndunited Senator Erin Oban (D-35) Senator Rich Wardner (R-37) Representative Pam Anderson (D-41) Representative Mary Johnson (R-45) Senator Ron Sorvaag (R-45) These legislators received our endorsement based on their voting records during the 2015 and 2017 legislative sessions, and their proven commitment to the priorities and values of our members. -

2021 FPA-ND Legislative Scorecard
2021 NORTH DAKOTA LEGISLATIVE REPORT CARD 67th LEGISLATIVE SESSION ABOUT THE SCORECARD We are pleased to share this scorecard for the 2021 North Dakota state legislative session. This is a snapshot of how lawmakers voted on key social and moral legislation related to life, education, family, religious freedom, and similar issues. Guided by our mission of building a state where God is honored, religious freedom flourishes, families thrive, and life is cherished, the scorecard focuses on seven bills. This scorecard is not an endorsement of any candidate or political party. It does not measure any lawmakers’ integrity, commitment to their faith, work ethic, or rapport with Family Policy Alliance of North Dakota. It is only a report on how each lawmaker voted. Please continue to hold our legislators accountable for their voting records and please pray that they may always vote in ways that uphold your biblical values as they make important decisions for our state. Sincerely, Mark Jorritsma Executive Director, Family Policy Alliance of North Dakota HOW WE FIGURED THE GRADES A bill is typically passed by a simple majority in the Senate (24 votes out of 47 senators) and the House (48 votes out of 94 Representatives.) Lawmakers earned percentage grades ranging from 0% to 100%, based upon dividing the candidate’s number of good votes cast by the number of total bills he/she voted on. The higher the score, the better their ranking. Not all lawmakers voted on every bill; the number of absences on these key bills is also noted and we encourage you to review whether your legislator actually voted on these important bills. -

Directory Governor Doug Burgum North Dakota Legislative Hotline: Lt Governor Brent Sanford for 1-888-635-3447 Attorney General Wayne Stenehjem
North Dakota Elected Officials Reach Your Legislators Directory Governor Doug Burgum North Dakota Legislative Hotline: Lt Governor Brent Sanford for 1-888-635-3447 Attorney General Wayne Stenehjem Secretary of Al Jaeger Bismarck Area: 328-3373 State Legislative Web Site: Treasurer Kelly Schmidt www.legis.nd.gov 66th North Dakota Auditor Josh Gallion Legislative Assembly and Superintendent Kirsten Baesler of Public Join the North Dakota Catholic Elected Officials Instruction Conference Legislative Action Agricultural Doug Goehring Network Commissioner Sign-up at: ndcatholic.org/ Insurance Jon Godfread registration/ Commissioner Or contact the North Dakota Tax Ryan Rauschenberger Catholic Conference at: Commissioner (701) 223-2519 Public Service Brian Kroshus Commissioners Julie Fedorchak 1-888-419-1237 Randy Christmann [email protected] North Dakota Catholic Conference 103 South Third Street, No. 10 Bismarck, North Dakota 58501 U.S. Senator John Hoeven Christopher T. Dodson U.S. Senator Kevin Cramer Follow Us Executive Director U.S. Kelly Armstrong Representative (701) 223-2519 1-888-419-1237 Get contact information for all [email protected] state officials at nd.gov. www.facebook.com/ndcatholic ndcatholic.org Senate House of Representatives Howard C. Anderson, [email protected] 8 Patrick Hatlestad [email protected] 1 Dwight Kiefert [email protected] 24 JoNell A. Bakke [email protected] 43 David Richter [email protected] 1 Alisa Mitskog [email protected] 25 Brad Bekkedahl [email protected] 1 Bert Anderson [email protected] 2 Cynthia Schreiber-Beck [email protected] 25 Randy Burckhard [email protected] 5 Donald W. Longmuir [email protected] 2 Sebastian Ertelt [email protected] 26 David A. -

Nextera Energy PAC 2018 Contributions to State Candidates
NextEra Energy PAC 2018 Contributions to State Candidates Recipient 2018 Amount Chamber State Party Gretchen Whitmer for Governor $ 10,000 Governor MI D Thompson for Senate 2018$ 10,000 STATE SENATE OK R Friends of John Michael Montgomery 2018$ 8,000 STATE SENATE OK R Caldwell for State House$ 7,500 STATE HOUSE OK R Friends of Scott Fetgatter$ 7,500 STATE HOUSE OK R Ken Paxton Campaign$ 7,500 ATTORNEY GENERAL TX R Trey Caldwell for State House 2018$ 7,000 STATE HOUSE OK R Dana Murphy for Lt. Governor$ 5,000 LT. GOVERNOR OK R Friends of Charles McCall $ 5,000 STATE HOUSE OK R Friends of Larry Householder $ 5,000 STATE HOUSE OH R Friends of Todd Russ $ 5,000 STATE HOUSE OK R Stitt for Governor $ 5,000 GOVERNOR OK R Tony for Wisconsin $ 5,000 GOVERNOR WI D Tom Wolf for Governor $ 3,500 GOVERNOR PA D Charles Perry Campaign $ 3,000 STATE SENATE TX R Dawn Buckingham Campaign $ 3,000 STATE SENATE TX R Drew Darby Campaign $ 3,000 STATE HOUSE TX R Four Price Campaign $ 3,000 STATE HOUSE TX R Friends of Greg Babinec $ 3,000 STATE HOUSE OK R Kristi for Governor $ 3,000 GOVERNOR SD R Angela Paxton Campaign $ 2,500 STATE SENATE TX R Brian Birdwell Campaign $ 2,500 STATE SENATE TX R Citizens for Pat Grassley $ 2,500 STATE HOUSE IA R Dennis Bonnen Campaign $ 2,500 STATE HOUSE TX R Friends of James Leewright 2018 $ 2,500 STATE SENATE OK R Friends of John Zerwas $ 2,500 STATE HOUSE TX R Friends of Kim David $ 2,500 STATE SENATE OK R Friends of Stephanie Bice 2018 $ 2,500 STATE SENATE OK R Jacob Rosecrants for HD 46$ 2,500 STATE HOUSE OK D Ken King Campaign $ 2,500 STATE HOUSE TX R Parson for Missouri $ 2,500 GOVERNOR MO R Perryman in 2018 $ 2,500 STATE HOUSE OK D Phil King Campaign $ 2,500 STATE HOUSE TX R Robert Nichols Campaign $ 2,500 STATE SENATE TX R Texans for Kelly Hancock SPAC $ 2,500 STATE SENATE TX R William Casey Murdock 2018 $ 2,500 STATE HOUSE OK R Ana Maria Rodriguez Campaign $ 2,000 STATE HOUSE FL R Ardian Zika Campaign$ 2,000 STATE HOUSE FL R Brett Hage Campaign$ 2,000 STATE HOUSE FL R Bryan Hill for House 2018 $ 2,000 STATE HOUSE OK R Charles Clemons Sr. -
House Standing Committees
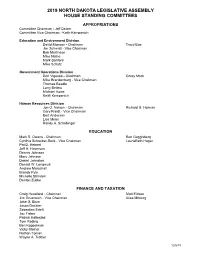
2019 NORTH DAKOTA LEGISLATIVE ASSEMBLY HOUSE STANDING COMMITTEES APPROPRIATIONS Committee Chairman - Jeff Delzer Committee Vice Chairman - Keith Kempenich Education and Environment Division David Monson - Chairman Tracy Boe Jim Schmidt - Vice Chairman Bob Martinson Mike Nathe Mark Sanford Mike Schatz Government Operations Division Don Vigesaa - Chairman Corey Mock Mike Brandenburg - Vice Chairman Thomas Beadle Larry Bellew Michael Howe Keith Kempenich Human Resources Division Jon O. Nelson - Chairman Richard G. Holman Gary Kreidt - Vice Chairman Bert Anderson Lisa Meier Randy A. Schobinger EDUCATION Mark S. Owens - Chairman Ron Guggisberg Cynthia Schreiber-Beck - Vice Chairman LaurieBeth Hager Pat D. Heinert Jeff A. Hoverson Dennis Johnson Mary Johnson Daniel Johnston Donald W. Longmuir Andrew Marschall Brandy Pyle Michelle Strinden Denton Zubke FINANCE AND TAXATION Craig Headland - Chairman Matt Eidson Jim Grueneich - Vice Chairman Alisa Mitskog Jake G. Blum Jason Dockter Sebastian Ertelt Jay Fisher Patrick Hatlestad Tom Kading Ben Koppelman Vicky Steiner Nathan Toman Wayne A. Trottier 12/6/18 HUMAN SERVICES Robin Weisz - Chairman Gretchen Dobervich Karen M. Rohr - Vice Chairman Mary Schneider Dick Anderson Chuck Damschen Bill Devlin Clayton Fegley Dwight Kiefert Todd Porter Matthew Ruby Bill Tveit Greg Westlind Kathy Skroch INDUSTRY, BUSINESS AND LABOR George Keiser - Chairman Mary Adams Mike Lefor - Vice Chairman Pamela Anderson Glenn Bosch Marvin E. Nelson Craig Johnson Jim Kasper Vernon Laning Scott Louser Emily O’Brien David Richter Dan Ruby Austen Schauer JUDICIARY Kim Koppelman - Chairman Ruth Buffalo Karen Karls - Vice Chairman Karla Rose Hanson Rick Becker Terry B. Jones Jeffery J. Magrum Aaron McWilliams Bob Paulson Gary Paur Shannon Roers Jones Bernie Satrom Luke Simons Steve Vetter AGRICULTURE Dennis Johnson - Chairman Ruth Buffalo Wayne A. -
Aicpa Fall Meeting of Council by Patrick Kautzman, AICPA Council Member
January 2019 | Volume XXXVI | No. 1 aicpa fall meeting of council By Patrick Kautzman, AICPA Council Member Since TCJA passed last December, we have heard from a multitude of professionals with varying levels of concern regarding the continued existence of the food and beverage deduction in light of the fate of entertainment expenses. Well, Notice 2018-76, issued October 3, 2018, clarifies that taxpayers generally may continue to deduct 50% of the food and beverage expenses associated with operating their trade or business. Professional Issues Update by Barry Meloncon, President and CEO of AICPA Barry’s professional issues update included his recurring reminders of the rapid pace of innovation and disruption in our world and our industry. • Since the year 2000, 41% of S&P consumer-centric companies have been acquired 2019 or gone out of business and 39% of the 5th to 85th largest firms no longer exist as standalone firms. Conference dates • The World Economic Forum’s Future of Jobs Report shows that of the top 10 de- clining jobs by 2022, #2 is Accounting, Bookkeeping, and Payroll Clerks and #7 is Accountants and Auditors. Barry’s response: They are referring to an industry that Management Conference is unwilling to change and adapt! He broke a future ready strategy down into 3 parts: May 22-23 • Technology – Master it before it masters you Fargo Holiday Inn • Trust – Build on CPAs expertise • Talent – Think broader Summer variety pack Technology – CPAs must embrace “Software as a Service” through client accounting June 17-19 services and virtual CFO services, “Big Data and Analytics”, “Artificial Intelligence” through Bismarck Ramkota machine learning and virtual assistance, and “Blockchain”. -
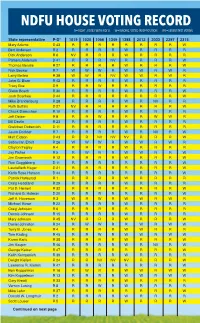
Ndfu House Voting Record for 2019 Session R=Right , Voted with Ndfu W=Wrong, Voted in Opposition Nv=Absent/Not Voting *Party-District
NDFU HOUSE VOTING RECORD FOR 2019 SESSION R=RIGHT , VOTED WITH NDFU W=WRONG, VOTED IN OPPOSITION NV=ABSENT/NOT VOTING *PARTY-DISTRICT State representative P-D* 1019 1020 1066 1349 1388 2012 2033 2297 2315 2344 2345 2360 Votes w/ NDFU % of votes w/ NDFU Mary Adams D 43 R R R R R R R R W R R R 11 91.67% Bert Anderson R 2 R R R R W R R R R R W R 10 83.33% Dick Anderson R 6 NV R R R W R R R R W NV R 8 66.67% Pamela Anderson D 41 R R R NV R R R R W R R R 10 83.33% Thomas Beadle R 27 R R R R W R R R W W W R 8 66.67% Rick Becker R 7 W W W R W W R W R R W W 4 33.33% Larry Bellew R 38 W W R NV W W R W R W W W 3 25.00% Jake G. Blum R 42 R R R R W R R R R NV W R 9 75.00% Tracy Boe D 9 R R W R R R R R R R W R 10 83.33% Glenn Bosch R 30 R R R R W R R R W W W NV 7 58.33% Josh Boschee D 44 R R R R R R R R W R R R 11 91.67% Mike Brandenburg R 28 R R R R W R NV R R W W R 8 66.67% Ruth Buffalo D 27 NV R R R R R R R W R NV R 9 75.00% Chuck Damschen R 10 R R R R W R R R R W W R 9 75.00% Jeff Delzer R 8 R R W R R R W W R W W R 7 58.33% Bill Devlin R 23 R R R R W R R R R W W R 9 75.00% Gretchen Dobervich D 11 R R R R R R R R R R R R 12 100.00% Jason Dockter R 7 R R R R W R NV R W W W R 7 58.33% Matt Eidson D 43 R R NV NV NV R R R W R R R 8 66.67% Sebastian Ertelt R 26 W W W R W W R W R R W R 5 41.67% Clayton Fegley R 4 R R R R W R R R R W W R 9 75.00% Jay Fisher R 5 R W R R W W R R W W W R 6 50.00% Jim Grueneich R 12 R R R R W R R R W W W R 8 66.67% Ron Guggisberg D 11 R R R R R R R R W R R R 11 91.67% LaurieBeth Hager D 21 R R R R R R R R W R R R 11 91.67% Karla Rose Hanson D 44 R R R R R R R R W R R R 11 91.67% Patrick Hatlestad R 1 R R R R W R R R R W W R 9 75.00% Craig Headland R 29 R R R R W R R R R W W R 9 75.00% Pat D.