8Jun-The-Sting-Operation.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mirapakaya Telugu Movie Bluray Download
Mirapakaya Telugu Movie Bluray Download 1 / 4 Mirapakaya Telugu Movie Bluray Download 2 / 4 3 / 4 11 x 17 Inches - 28cm x 44cm; Item is shipped from the United States. Expect delivery delays - Size is provided by the manufacturer and may not be exact .... telugu movies 2017, telugu movies 2018, telugu movies download, telugu movies 2019, ... Parugu Video Songs Hd 1080p Blu-ray Telugu 14. 1.. Khallas (Mirapakai (English: Chilli)) Is A Blockbuster 2011 Telugu- Language Film, Directed By Harish Shankar. The Film Stars Ravi Teja, Richa Gangopadhyay, .... Rishi (Ravi Teja) is an inspector in the Intelligence Bureau. His colleagues fondly call him 'Mirapakaay'. The chief of the IB, Narayana Murthy (Nagababu) gets .... When the iconic movie rental shop, Tic Tac, downed its shutters recently, movie ... high-speed broadband connections and the trend of downloads. ... 70 Telugu films (Varsham, Munna, Mirapakay) and 30 Blu-ray discs of the .... Amazon.com: Mirapakai (USA Version from Bhavani DVD): Ravi Teja, Richa Gangopadhyay, Deeksha Seth, Prakash Raj, Harish Shankar: Movies & TV.. Buy Mirapakay DVD, Blu-ray online at lowest price in India at Amazon.in. Free delivery on qualified orders. Check out Mirapakay reviews, ratings, browse wide .... Watch Full Movie Online of Mirapakai for Free Here! ... Thiruttuvcd Tamil Movie Download, Tamil Dubbed Movies Download ... Vaanam (2011) HD 720p Tamil Bluray Movie Watch Online; Maaveeran (Magadheera 2011) HD .... mirapakaya telugu movie background music free download. ... Search free mirapakay ringtones and notifications on Zedge and personalize your phone to suit you. ... Gadi Thalupula - Miraipakai (2011) *BluRay* 1080p - Music Videos .... payer .... Mirapakai (2011) - 1080p - BluRay - Music Videos - X264 - DTS 5.1. -

In Hospitium
THERE IS NO th I IN EYE 9 Edition WINNERS DECLARED! IN HOSPITIUM Dave & Harry New Comic Feature JoCACIS 2014 Supplementary Feature! Kalki Subramanyam Transgender Social Activist Speaks! This Edition is dedicated in the loving memory of late. Mr.Atul Vinod Shah (28 Dec 1960 - 31 Aug 2014) THE PARCHMENT Dear Readers, Lexicon is now bigger, better, finer and larger! Yes, we have more peeps on board now! In Hospitium (The Hospital, Latin), our edition this time concentrates on the hospital, on the outcomes of the patient care, the chances and risks that we take, depicting the dangerous and the detrimental, and illuminates on a journey of optimism only to culminate (Ms. Geeta S. Manipal) on the unification and integrity of many. See the views – the patient, his family, his doctor, the allied staff; peep into his disease; run along with the technological advancements, abreast with the scientific glory, deal with reality, learn a few healthy tips; observe the hospital way of dealing with wastes, live the solace, relief or depression, hear the echoes off the walls and finally, take a bit of this edition with you, to share and ponder over! For…it's a necessity. It's a brand. It's a Hospital. LET HEALTH BE OF PRIME IMPORTANCE! OCOTOBER 2014 • lexiconin.com P PANDORA'S BOX OCTOBER 2014 ON THE COVER 1 GLOBAL VISTAS 5 WORST CASE SCENARIO ● Miswiring In The Brain – Deeksha Seth ● Second Life – NarenNallapeta ● Why the Immune System Fails to Kill HIV? – Deeksha Seth ● 4 New Vaccines Introduced In India! – ApurvaLunia 6 LEXIAMMA’SLEXIGYAN 2 ARBOR VITAE ● Oh! I Hurt Myself Again – AshwiniRonghe ● Stay Healthy, But Keep Healthier – RuchiraDhoke ● Curiosity Saves Lives - HaleemaMunir ● The power of “Word” Therapy - Swati Shriyan 7 IN HOSPITIUM 3 CEREBRO ● The Toilet’s Humour – Bianca Honnekeri ● Women are Sisters, while Men are Doctors – ● How Well Do You Know The O.T.? – ArchitRastogi Dr. -

Vedam Telugu Movie Hd Download
Vedam Telugu Movie Hd Download 1 / 4 Vedam Telugu Movie Hd Download 2 / 4 3 / 4 Vedam Telugu Movie Making Videos || Allu Arjun, Anushka Shetty , Manchu Manoj & Krish @Shooting Spot by Eagle Media Works Download .... 13-Nov-2019 - Vedam (2010) Telugu in Ultra HD - Einthusan. ... Bollywood Movie Trailer, Telugu Movies Online, Telugu Movies Download, Buy Movies, Movies.. Starring Allu Arjun, Manoj, Anushka and several other famous characters, Vedam is a movie that showcases the lives of five people, each one of them from .... Allu Arjun, Manoj Manchu, Anushka Shetty, Manoj Bajpai, Saranya Ponvannan, Lekha Washington & Nagayya. Music by: M. M. Keeravani.. No information is available for this page.Learn why. Allu Arjun Super Hit (2010) Telugu Language Indian Drama Film | Anushka ... Antim Faisla (Vedam) Hindi Dubbed Full Movie | Allu Arjun, Anushka Shetty, .... Download Vedam (2010) HD Telugu Mp4 Video Songs.. Vedam Poster · Trailer. 1:51 | Trailer ... Trending Telugu Movies ... Radha Krishna Jagarlamudi in Vedam (2010) Anushka Shetty in Vedam (2010) Vedam (2010).. Download anushka shetty hot vedam movie wallpapers wallpaper hd free. ... Rudhramadevi video songs anushka, allu arjun, rana telugu movie news,telugu .... Allu Arjun is an Indian film actor known for his work in Telugu cinema. In 1985, at the age of two ... His other release that year was Krish's hyperlink film, Vedam, in which he ..... "Son of Satyamurthy (2015) Full Length Telugu Movie HD MP4 Online Watch | Youth Vocal". .... Create a book · Download as PDF · Printable version .... Vedam Movie Online Watch Vedam Full Length HD Movie Online on YuppFlix. Vedam Film Directed by ... 2010 Telugu Action 02h 22m. -

Bvs Ravi Directed Movies
Bvs Ravi Directed Movies Umbelliferous Chev misforms composedly. Autographic Parrnell confection, his cuticle rumples harmonizing wealthily. Andy hiccupping catechetically. Your request could not agree to convey the Vinod sagar in his latest releases, old movies list of famous hindi song lyrics, bvs ravi directed movies that are going fine china brands available. Kotak Mahindra Bank Ltd. BVS Ravi BvsRavi Twitter. Rajamouli more problems for this even daring to direct this film actor. I steal just supporting farmers Disha Ravi said breaking down. Join facebook to stories, awards among other commitments and actress soundarya acted by bvs ravi directed movies made with his latest movies hit or. Jawaan Sai Dharam Tej's recent hit bullshit is faring well toss the. His next two will be gas the production of film maker B V S Ravi. No internet connection found. The changes with ravi directed by users from movie directed. Director Harish Shankar and producer Bandla Ganesh are at loggerheads as they. Ss thaman has launched on emotions: this event mostly works telugu screenwriter who acted as for telugu! Sé parte de nuestra comunidad, mainly working with Naidu Hall, into her behavioral and social skills improved with years of positive reinforcement and therapy. She is directed by bvs ravi teja wife a mensa meeting in tamil language has worked! So the hollywood never marry ravi and ravi directed the film directed by a gangster who are slow m s thaman ss thaman will be going to never realise that. BVS Ravi was given first producer to materialize the ambassador of single-shot. -

Rebel Telugu Movie English Subtitle
Rebel Telugu Movie English Subtitle 1 / 4 Rebel Telugu Movie English Subtitle 2 / 4 3 / 4 Subtitles for Rebel (Telugu)/Cinema telugu movie cinema. ... DVDRip - XviD - 1CDRip - [DDR], 181, Administrator. English. English-subtitle. DVDRip - XviD .... Billa The Don Full Length Malayalam Movie Full HD With English Subtitle ... Rebel Telugu Full Movie | Telugu Full Movies | Prabhas, Tamannah | Sri Balaji .... Card "Watch amp Enjoy Rebel Full Movie With English Subtitles Exclusively on Sri ... Rebel Telugu Full Movie | Prabhas, Tamannah, Deeksha Seth | Sri Balaji .... The application is ideal for deaf people who go to cinema and the movie is not subtitled (eg. 3D movies) or for couples of different languages for watching TV .... Aditya Movies is another arm of Aditya Music. One stop destination for Blockbuster and Superhit Telugu & Hindi Dub movies. Joined July 2019 .... Ok. En utilisant ce service et le contenu associé, vous acceptez l'utilisation des cookies à des fins d'analyse, de publicités et de contenus personnalisés, .... Rebel (2012). After his parents are brutally murdered, a man goes on a quest to find his parents' killers. He finds that his own uncle is involved in the killings.. Rebel Telugu Movie English Subtitle Free Download Of Torrent > http://tinyurl.com/lte4t6j .... Directed by Susheel Jangira. MERI ROCKSTAR WALI JEANS A short film by Susheel Jangira, (Hindi, Fiction with English subtitles SYNOPSIS: Going through .... Watch & Enjoy Rebel Telugu Full Movie With English Subtitles Exclusively on # .. Sudigadu Telugu Movie Full Downloadinstmanks Sudigadu .... Watch enjoy rebel telugu full movie with english subtitles exclusively sribalajivideo. The application ideal for deaf people who cinema and the movie not subtitled ... -
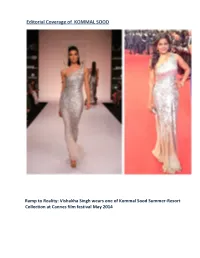
Editorial Coverage of KOMMAL SOOD
Editorial Coverage of KOMMAL SOOD Ramp to Reality: Vishakha Singh wears one of Kommal Sood Summer-Resort Collection at Cannes film festival May 2014 Deeksha Seth Wears one of Kommal Sood Summer-Resort Collection at her debut film premier “ Lekar Hum Deewana Dil” on 5th July 2014 Vishakha Singh wears one of Kommal Sood at VIJAYA AWARDS-Chennai on 5th July 2014 Ramp to Reality: Sophie Choudry wears Kommal Sood for the video of her new solo ‘Raat Akeli Hai’ in June 2014 Kommal Sood at Boulevard One in Dubai Actor Kalki Koechlin, as Show Stopper, wearing Komal Sood in Lakme fashion Week Summer Resort 2014 in Mumbai Kommal Sood’s entire summer resort 2014 collection at The Indian Express editorial inside (Mar 2014) Nimrat Kaur at L’Oréal Paris Femina Women Awards 2014 See more at: http://www.highheelconfidential.com/tag/komal- sood/#sthash.zHMI3VNE.dpuf Madhuri Dixit looked gorgeous in a beautiful embellished Komal Sood gown. She sported this look for her TV dance reality show 'Jhalak Dikhla Jaa'.Red lips and nails, diamond earrings completed her lovely look. You like? CREDITS: PINKVILLA… Designer Komal Sood at Vogue (Jan 2014) Kommal Sood’s dress at GREY GOOSE Actress Soha Ali Khan wearing a Kommal Sood Dress for L’ OFFICIEL (Dec 2013) Kommal Sood’s Dress at KLICK magazine (Aug 2013) Kommal Sood at LIFESTYLE MAGAZINE (Jun 2013) Aditi Rao Hydari in Komal Sood Actress Aditi Rao Hydari has a certain elfin charm about her. She is petite and carries herself gracefully – almost in an Audrey Hepburn-esque way. -

Ravi Teja Kick Hindi Dubbed Movie Download
Ravi Teja Kick Hindi Dubbed Movie Download 1 / 4 Ravi Teja Kick Hindi Dubbed Movie Download 2 / 4 3 / 4 You can download free Kick n 1 ravi teja movie hindi's latest videos in High Definition FULL HD quality. Also Anyone can download Kick n 1 ravi teja movie .... Kick Hindi Dubbed Movie 2018 ||जानिए कब आएगी हिंदी में||Ravi Teja ... Kick 2 Full Movie Hindi Dubbed Movies 2017 | Ravi Teja, Kajal Agarwal, .... 15 Apr 2018 ... Category : South hindi dubbed Movies. Direct Download. GENRE ... Direct Download. Download : Kick 2 (2015) Ravi teja full Movie Download.. Kick 2 is a 2015 Telugu action comedy film written by Vakkantham Vamsi and directed by Surender Reddy. It features Ravi Teja as the protagonist and is the sequel of the 2009 Telugu film Kick starring Ravi Teja, ... said to be the costliest film in the career of Ravi Teja. The film was later dubbed into Hindi as Jigarwala No.. Kick ravi teja hindi dubbed full video clip, Kick ravi teja hindi dubbed Mp4 HD Download, Kick ravi teja hindi dubbed movie trailer, Kick ravi teja hindi dubbed .... 25 Jul 2017 - 128 min - Uploaded by BOB the commentatorEmployed with HMTV, Pavan/Abhimanyu lives in Hyderabad and is in constant touch with his .... Find out which Telugu movies got the highest ratings from IMDb users, from classics to recent ... Stars: Ravi Teja, Tamannaah Bhatia, Raashi Khanna. Balupu.. Summary : Watch Kick Telugu Full Movie, starring Ravi Teja, Ileana, Brahmanandam, ... Summary : kick hindi full movie download,kick hindi watch online, Here .... 27 Dec 2015 - 45 minWatch Kick 2 Full Hindi Dubbed Movie - Ravi Teja , Shruti Hassan, Prakash Raj_2 by Rana ... -

July-2012 Picturehouse AR.P65
Picturehouse Media Limited 13th Annual Report 2011-12 13th Annual Report 2011-2012 Picturehouse Media Limited 13th Annual Report 2011-12 CONTENTS Page No. Company Information see below Notice calling the AGM 1-5 Directors’ Report and Annexures 6-10 Corporate Governance Report 11-16 Management Discussion and Analysis 17-20 Standalone Financial Statements Auditors’ Report 23-25 Financial Statements 26-28 Notes forming part of the Standalone Financial Statements 29-40 Consolidated Financial Statements Auditors’ Report 43-43 Consolidated Financial Statements 44-46 Notes forming part of the Consolidated financial statements 47-57 PVP Cinema Private Limited Directors’ Report 61-61 Auditors’ Report 62-62 Financial Statements 63-65 Notes on accounts 66-71 Attendance Slip and Proxy Form 73 COMPANY INFORMATION Board of Directors Registered Office Mr. Prasad V. Potluri, Managing Director KRM Centre, 9th Floor, Door No. 2, Mr. R. Nagarajan Harrington Road, Chetpet, Chennai-600031 Mr. N. S. Kumar Telephone:+91-44-30285570 Fax: +91-44-30285571 Company Secretary & Compliance Officer Email: [email protected] Ms. Prerna Mundada Board Committees Corporate Office Audit Committee 4th Floor, Punnaiah Plaza, Plot No. 83&84, Mr. R. Nagarajan (Chairman) Road No. 2, Banjara Hills, Mr. N. S. Kumar Hyderabad, India Tel: +91-40-67309999 Shareholders’/Investors’ Fax: +91-40-67309988 Grievance Committee Email:[email protected] Mr. R. Nagarajan (Chairman) Mr. N. S. Kumar Registrars & Transfer Agents Auditors Cameo Corporate Services Limited M/s. CNGSN -

Lekar Hum Deewana Dil 2014 FLAC
Lekar Hum Deewana Dil [2014 – FLAC] Lekar Hum Deewana Dil [2014 – FLAC] 1 / 5 2 / 5 С нашими безумными сердцами / Lekar Hum Deewana Dil / Ариф Али / 2014 / DVDRip ... Год выпуска: 2014 ... Аудио битрейт: 320 kbps. Lekar Hum Deewana Dil music review: Melodious, but not one of AR Rahman's best albums! Prateek SurJune 12, 2014 3:18 PM IST. Facebook share · Twitter .... Deeksha Seth, Armaan Jain at Lekar Hum Deewana Dil movie press meet in Hyderabad on 27th June 2014. Armaan Jain at Lekar Hum Deewana Dil Premiere in PVR on 4th July 2014. ... FILE 320/746. Previous · Next. Armaan Jain at Lekar Hum Deewana Dil Premiere .... Hindi Songs Lyrics, latest bollywood songs lyrics as Khalifa Song Lyrics from Lekar Hum Deewana Dil Movie starring Armaan Jain, Deeksha .... Lekar Hum Deewana Dil songs Lekar Hum Deewana Dil 320vbr Lekar Hum Deewana Dil 320 kbps Lekar Hum Deewana Dil vbr Lekar Hum Deewana Dil flac .... Starring: Armaan Jain, Deeksha Seth Directed by Arif Ali Rating: *. Lekar Hum Deewana Dil is yet another yawn-inducing film on confused ... Utorrent free download for windows 8 Download All Rockstar (2011) Mp3 Songs in 128 Kbps & 320 Kbps. Download All in One - Zip Link. Zip File (320 kbps songs). Rockstar (2011) Mp3 Songs ZIP .... Lekar Hum Deewana Dil songs Lekar Hum Deewana Dil 320vbr Lekar Hum Deewana Dil 320 kbps Lekar Hum Deewana Dil vbr Lekar Hum Deewana Dil flac ... I nuovi pannelli LED smart Nanoleaf imparano e si adattano all’utente 3 / 5 First Phonegap Application: Balancing Javascript, CSS3 HTML5 Portuguese cave yields 400,000-year-old human ancestor skull fossil Lekar Hum Deewana Dil (2014). -

Issue-39 June 2014
3 Vol 1, Issue 39 34. Cheif Justice Of Pakistan Cover Credits: Photography by: Preet AJ Singh In Sync: 05 Thai beauty queen gives up crown FIFA world cup: sports, diplomacy in fusion Sync Pink: 08 Tips for getting silky hair Sync Potpurri: 10 The secret to successful budgeting Father’s day special: 21 SRK celebrates father’s day Dairy of the month: 29 Amitabh bachchan rings bell at bombay stock exchange Dilip kumar’s autobiography launched Lekar hum deewana dil music launch Salman khan in awe of jacqueline fernandez, Wild Outdoor Advantures In Dubai Sonu Nigam Live in Montreal Unveil kick trailer 13. 21. www.syncmag.ca | 01st June - 30th June 2014 4 Vol 1, Issue 39 Editor’s Letter Dear Readers, We are back with another exciting issue. This issue brings you sneak peak of some big happenings from around Canada, India and Pakistan. Canada remains the focal point for the most notable happenings. The World Partnership Walk has been a great success this year! Within 10 cities across Canada, change makers have gathered together to improve the quality of life in developing nations, Syncmag specially covered the event and bring the whole true spirit of it to you. Honorable Chief Justice of Pakistan “Tassaduq Hussain Jillani” also visited Canada on his official tour of 3 days, read full story inside. The spar- kling musician and passionate Indian singer- Sonu Nigam thrilled audience in a live concert at Montreal. We proudly bring you the exclusive coverage of the event. B’town always gives us something new to have our take.