Rental Application
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Newfoundland Antique and Classic Car Club (NACCC) April – June 2008
Newfoundland Antique and Classic Car Club (NACCC) April – June 2008 Iron Wood Shopping Mall, Richmond BC (Picture compliments of Walter and Shirley LaCour) President’s Message Another cruising season has started and Classic Wheels 2008 Car show is now history. Time surely flies when we are having fun getting prepared for the show. I would like to thank all the members who participated in the show whether it was helping to plan the car show, showing your car, volunteering with ticket sales or whatever. Without your help it would be impossible to do such an event. Congratulations to all the trophy winners. It is very difficult to choose from such beautiful classic automobiles. According to the list of activities and events in the calendar it seems we will have a very busy season. We suggest you refer to the calendar for events that will interest you. Of special note is a show and shine on July 1 at the Royal Canadian Legion Branch 1 for our veterans. A large attendance will show our thanks to all the veterans from past and present for the sacrifice they made for us. There will be information in the newsletter pertaining to this. Our car club plans to visit the A&W on Cunard Crescent, in Donavans on a regular basis every second Thursday night. Owner, Scott Bartlett, promises to make our visits interesting and will give the club a percentage for A&W catalogue merchandise purchased. Please remember cruising and socializing is what our club is all about so get out and meet up with the members and enjoy our short cruising season. -

Municipal Backyard Compost Bin Program Participants 2011-Present 2018
Municipal Backyard Compost Bin Program Participants 2011-Present 2018 Baie Verte Bay St George Waste Management Committee Cape St George Channel Port au Basques City of St John's Gander Greens Habour Lourdes New-Wes-Valley Northern Peninsula Regional Service Board Paradise Pasadena Sandy Cove Trinity Bay North Twillingate 2017 Baie Verte Carbonear Corner Brook Farm and Market, Clarenville Grand Falls-Windsor Logy Bay-Middle Cove-Outer Cove Makkovik Memorial University, Grenfell Campus Paradise Pasadena Portugal Cove-St. Phillips Robert's Arm Sandy Cove St. Lawrence St. John's Twillingate 2016 2015 Brigus Baie Verte Burin Corner Brook Carmanville Discovery Regional Service Board Comfort Cove - New Stead Happy Valley - Goose Bay Fogo Island Logy Bay - Middle Cove - Outer Cove Gambo Sandy Cove Gander St. John's McIver’s Sunnyside North West River Witless Bay Point Leamington 2014 Burgeo Carbonear Conception Bay South (CBS) Lewisporte Paradise Portugal Cove - St. Phillip’s St. Alban’s St. Anthony (NorPen Regional Service Board) St. George’s St. John's Whitbourne Witless Bay 2013 Bird Cove Kippens Bishop's Falls Lark Harbour Campbellton Marystown Clarenville New Perlican Conception Bay South (CBS) NorPen Regional Service Board Conne River Old Perlican Corner Brook Paradise Deer Lake Pasadena Dover Placentia Flatrock Port au Choix Gambo Portugal Cove-St. Phillips Grand Bank Springdale Happy Valley - Goose Bay Stephenville Harbour Grace Twillingate 2011 Botwood Conception Bay South (CBS) Cape Broyle Conception Harbour Gander Conne River Glovertown Corner Brook Sunnyside Deer Lake Harbour Main – Chapel’s Cove – Gambo Lakeview Glenwood Holyrood Grand Bank Logy Bay Harbour Breton Appleton Heart’s Delight - Islington Arnold’s Cove Irishtown – Summerside Bay Roberts Kippens Baytona Labrador City Bonavista Lawn Campbellton Leading Tickles Carbonear Long Harbour & Mount Arlington Centreville Heights Channel - Port aux Basques Makkovik (Labrador) Colliers Marystown 2011 cont. -
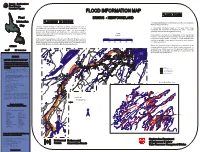
FLOOD INFORMATION MAP FLOOD ZONES Flood BRIGUS - NEWFOUNDLAND
Canada - Newfoundland Flood Damage Reduction Program FLOOD INFORMATION MAP FLOOD ZONES Flood BRIGUS - NEWFOUNDLAND Information FLOODING IN BRIGUS A "designated floodway" (1:20 flood zone) is the area subject to the most frequent flooding. Map Flooding causes damage to personal property, disrupts the lives of individuals and communities, and can be a threat to life itself. Continuing Beth A "designated floodway fringe" (1:100 year flood zone) development of flood plain increases these risks. The governments of une' constitutes the remainder of the flood risk area. This area Canada and Newfoundland and Labrador are sometimes asked to s Po generally receives less damage from flooding. compensate property owners for damage by floods or are expected to find Scale nd solutions to these problems. (metres) No building or structure should be erected in the "designated floodway" since extensive damage may result from deeper and While most of the past flood events on Lamb's Brook in Brigus have been more swiftly flowing waters. However, it is often desirable, and caused by a combination of high flows and ice jams at hydraulic structures may be acceptable, to use land in this area for agricultural or floods can occur due to heavy rainfall and snow melt. This was the case in 0 200 400 600 800 1000 recreational purposes. January 1995 when the Conception Bay Highway was flooded. Within the "floodway fringe" a building, or an alteration to an BRIGUS existing building, should receive flood proofing measures. A variety of these may be used, e.g.. the placing of a dyke around Canada Newfoundland the building, the construction of a building on raised land, or by Brigus the special design of a building. -

Proclamation Providing for the Holding of a General Election
NEWFOUNDLAND AND LABRADOR REGULATION 34/19 Prolaation Proidin for the oldin of a General lection (O.C. 2019-127) Filed April 17, 2019 ELIZABETH THE COND, b the Grae of God of the United indo, anada and er ther ealms and Territories QUEEN, ead of the omonwealth, efender of the aith JUDY M. FOOTE ANDREW PARSONS, Q.C. Lieutenant-Governor in General Attorney General TO ALL TO WHOM THESE PRESENTS SHALL COME, GREETING; A PROCLAMATION WHEREAS by Our Proclamation dated the 17th day of April, 2019, We did dissolve the Forty-Eighth General Assembly of Our Province of Newfoundland and Labrador; AND WHEREAS it is Our Will and Pleasure to summon and call a General Assembly within Our said Province and for that purpose to direct the issue of Writs of Election for a General Election of Members to serve in the House of Assembly of Our said Province; The Newfoundland and Labrador Gazette 183 April 18, 2019 Prolaation roidin for the 34/1 Holdin of a General lection AND WHEREAS under the authority of section 57 of the Elections Act, 1991 (the "Act"), We are empowered to direct the issuance of a Writ of Election for the election of Members to the House of Assembly; NOW KNOW YE that We do by this Our Proclamation direct that a Writ of Election for each of the Electoral Districts hereinafter mentioned be issued; AND WE DO further direct (1) That the last day for the nomination of candidates for the Election is Thursday, the 25th day of April, 2019, at 2:00 p.m. -

Office Allowances - Office Accommodations 01-Apr-15 to 31-Mar-16
House of Assembly Newfoundland and Labrador Member Accountability and Disclosure Report Office Allowances - Office Accommodations 01-Apr-15 to 31-Mar-16 Parsley, Betty, MHA Page: 1 of 1 Summary of Transactions Processed to Date for Fiscal 2015/16 Expenditure Limit (Net of HST): $4,834.00 Transactions Processed as of: 31-Mar-16 Expenditures Processed to Date (Net of HST): $4,833.87 Funds Available (Net of HST): $0.13 Percent of Funds Expended to Date: 100.0% Date Source Document # Vendor Name Expenditure Details Amount 01-Feb-16 HOA003482 WILLIAM JOHN FUREY Lease Payment for the Constituency Office of the MHA for the District of Harbour 1,350.00 Main located in Holyrood. 26-Feb-16 HOAJVDG-16126 Re-allocate the lease payment from December 14, 2015 to January 31, 2016 for 2,133.87 the constituency office for the District of Harbour Main 01-Mar-16 HOA003514 WILLIAM JOHN FUREY Lease Payment for the Constituency Office of the MHA for the District of Harbour 1,350.00 Main located in Holyrood. Period Activity: 4,833.87 Opening Balance: 0.00 Ending Balance: 4,833.87 ---- End of Report ---- House of Assembly Newfoundland and Labrador Member Accountability and Disclosure Report Office Allowances - Rental of Short-term Accommodations 01-Apr-15 to 31-Mar-16 Parsley, Betty, MHA Page: 1 of 1 Summary of Transactions Processed to Date for Fiscal 2015/16 Transactions Processed as of: 31-Mar-16 Expenditures Processed to Date (Net of HST): $0.00 Date Source Document # Vendor Name Expenditure Details Amount Period Activity: 0.00 Opening Balance: 0.00 Ending -

ST. MARY's the District of Placentia
PLACENTIA – ST. MARY’S The District of Placentia – St. Mary’s shall consist of and include all that part of the Province of Newfoundland and Labrador bounded as follows: Beginning at the intersection of the eastern shoreline of Chapel Arm, Trinity Bay, and the Town of Chapel Arm Municipal Boundary (2001); Thence running in a general southeasterly direction along the said Municipal Boundary to its intersection with the centre line of the Trans Canada Highway; Thence running in a general northwesterly direction along the centre line of the Trans Canada Highway to its intersection with the Meridian of 53o40’ West Longitude; Thence running due south along the Meridian of 53o40’ West Longitude to its intersection with the Parallel of 47o25’ North Latitude; Thence running due west along the Parallel of 47o25’ North Latitude to its intersection with the Town of Long Harbour-Mount Arlington Heights Municipal Boundary (2010); Thence running in a general southwesterly and northwesterly direction along the said Municipal Boundary to its intersection with the southern shoreline of Long Harbour; Thence running in a general southwesterly direction along the sinuosities of Placentia Bay to a point of land known as Point Lance; Thence running in a general northeasterly and southerly direction along the sinuosities of St. Mary’s Bay to a point of land known as Western Head; Thence running in a northeasterly direction along a line to the intersection of the centre line of the Trans Canada Highway and the centre line of Witless Bay Line, Route 13; Thence -

Thms Summary for Public Water Supplies in Newfoundland And
THMs Summary for Public Water Supplies Water Resources Management Division in Newfoundland and Labrador Community Name Serviced Area Source Name THMs Average Average Total Samples Last Sample (μg/L) Type Collected Date Anchor Point Anchor Point Well Cove Brook 154.13 Running 72 Feb 25, 2020 Appleton Appleton (+Glenwood) Gander Lake (The 68.30 Running 74 Feb 03, 2020 Outflow) Aquaforte Aquaforte Davies Pond 326.50 Running 52 Feb 05, 2020 Arnold's Cove Arnold's Cove Steve's Pond (2 142.25 Running 106 Feb 27, 2020 Intakes) Avondale Avondale Lee's Pond 197.00 Running 51 Feb 18, 2020 Badger Badger Well Field, 2 wells on 5.20 Simple 21 Sep 27, 2018 standby Baie Verte Baie Verte Southern Arm Pond 108.53 Running 25 Feb 12, 2020 Baine Harbour Baine Harbour Baine Harbour Pond 0.00 Simple 9 Dec 13, 2018 Barachois Brook Barachois Brook Drilled 0.00 Simple 8 Jun 21, 2019 Bartletts Harbour Bartletts Harbour Long Pond (same as 0.35 Simple 2 Jan 18, 2012 Castors River North) Bauline Bauline #1 Brook Path Well 94.80 Running 48 Mar 10, 2020 Bay L'Argent Bay L'Argent Sugarloaf Hill Pond 117.83 Running 68 Mar 03, 2020 Bay Roberts Bay Roberts, Rocky Pond 38.68 Running 83 Feb 11, 2020 Spaniard's Bay Bay St. George South Heatherton #1 Well Heatherton 8.35 Simple 7 Dec 03, 2013 (Home Hardware) Bay St. George South Jeffrey's #1 Well Jeffery's (Joe 0.00 Simple 5 Dec 03, 2013 Curnew) Bay St. George South Robinson's #1 Well Robinson's 3.30 Simple 4 Dec 03, 2013 (Louie MacDonald) Bay St. -

Arnnl Recognizes Nursing Excellence
Vol. XXXVI No. 3 September 2015 The Magazine of the Association of Registered Nurses of Newfoundland and Labrador IN THIS ISSUE ARNNL RECOGNIZES NURSING Council Bestows Honorary ARNNL Membership – 5 Upcoming Changes in Licensure Renewal Process – 7 EXCELLENCE ARNNL Continuing Education Teleconference Sessions – 11 PAGE 9 Technology Tips for Your Practice – 20 CONTENTS Message from the President ...........................................................................3 From the Executive Director’s Desk ................................................................4 ARNNL STAFF ARNNL Council Matters ..................................................................................5 Lynn Power, Executive Director 753-6173 I [email protected] Q & A: You Asked ............................................................................................6 Registration Update ........................................................................................7 Michelle Osmond, Director of Regulatory Services Canadian Nurses Protective Society ..............................................................8 753-6181 I [email protected] Nurses of Note ................................................................................................9 Lana Littlejohn, Director of Corporate Services Advanced Practice View ...............................................................................10 753-6197 I [email protected] ARNNL Continuing Education Teleconference Sessions ............................. 11 Trudy L. Button, Legal Counsel -

St. John's Sustainable Living Guide
St. John’s Sustainable Living Guide This sustainable living guide is the product of a class project for Geography 6250 at Memorial University, a graduate course on the conservation and sustainability of natural resources. It was designed by the class for the public of St. John’s. We would like to acknowledge Ratana Chuenpagdee (course professor) and Kelly Vodden (Geography Professor) for their guidance, comments and support. We would also like to thank the MMSB, and particularly Catherine Parsons (Marketing and Public Education Officer) for information about recycling programs in St. John’s. We would especially like to acknowledge Toby Rowe (Memorial University Sustainability Coordinator) for the interest in this work and for inviting us to display the guide on the MUN Sustainability Office Website. For more information about sustainability initiatives at Memorial University please visit www.mun.ca/sustain. Contributors: Amy Tucker Christina Goldhar Alyssa Matthew Courtney Drover Nicole Renaud Melinda Agapito Hena Alam John Norman Copyright © International Coastal Network, 2009 Recommended Citation: Tucker, A., Goldhar, C., Matthew, A., Drover, C., Renaud, N., Agapito, M., Alam, H., & Norman, J. 2009. St. John’s Sustainable Living Guide. Memorial University of Newfoundland, St. John’s, Newfoundland, Canada, 40 p. Any errors or omissions are the responsibility of the above contributors. Table of Contents Introduction………………………………………………………………………………………………………………..1 Sustainable Landscaping……………………………………………………………………………………………..2-4 Sustainable -

ARCHIVES and SPECIAL COLLECTIONS QUEEN ELIZABETH II LIBRARY MEMORIAL UNIVERSITY, ST
ARCHIVES and SPECIAL COLLECTIONS QUEEN ELIZABETH II LIBRARY MEMORIAL UNIVERSITY, ST. JOHN'S, NL Mary Schwall Photograph Collection COLL-206 Website: Archives and Special Collections Author: Bert Riggs Date: 1996 Scope and Content: This collection consists of 135 photographs taken by Mary Schwall or her companions while on excursions to Newfoundland during 1913 and 1915. They are a pictorial record of a journey by ship from Nova Scotia to Newfoundland, a train trip from Channel to St. John's, and a trip from St. John's north around the coast to St. Anthony, across the Strait of Belle Isle to Labrador and down the west coast of the Great Northern Peninsula. There is evidence that the photographs were taken during two trips to Newfoundland, as two photographs have the date 1913 on the back with the caption, while another has the date 1915. The photographs provide visual documentation of Mary Schwall's vacations, but they also provide valuable information on Newfoundland communities during the early years of the twentieth century. Vernacular architecture historians have attested to the fact that several of the photographs show buildings only previously known through oral accounts. As well there is visual documentation of people, especially children, which can provide information on lifestyle, dress, nutrition, disease, and a host of other subjects.In addition, there are 56 postcards with images covering much the same geographical area as the photographs, leading one to believe that they were purchased in larger communities during stopovers, or possibly in St. John's. Most of the postcards were produced for the St. -

Background Report City of Mount Pearl
DRAFT KENMOUNT HILL COMPREHENSIVE DEVELOPMENT SCHEME BACKGROUND REPORT CITY OF MOUNT PEARL | MARCH, 2018 | CONTACT INFORMATION: 100 LEMARCHANT ROAD | ST. JOHN’S, NL | A1C 2H2 | P. (709) 738-2500 | F. (709) 738-2499 WWW.TRACTCONSULTING.COM Kenmount Hill Comprehensive Development Scheme BACKGROUND REPORT City of Mount Pearl March 2018 Contact Information: Neil Dawe, President Tract Consulting Inc. P. 709.738.2500 F. 709.738.2499 email [email protected] www.tractconsulting.com Tract Consulting Inc. Proposed Development Plan for Lands Above the 190 Metre Contour: Kenmount Hill Comprehensive Development Scheme BACKGROUND REPORT Table of Contents 1. UNDERSTANDING THE PROJECT ............................................................................ 1 1.1. Purpose and objectives of the study ......................................................................................... 1 1.2. Study location ............................................................................................................................ 2 1.3. Land ownership patterns........................................................................................................... 3 1.4. Civic Policy Context ................................................................................................................... 3 1.5. Review of City of Mount Pearl planning documents, growth data and mapping .................... 4 1.6. Planning Methodology ............................................................................................................. -

The Hitch-Hiker Is Intended to Provide Information Which Beginning Adult Readers Can Read and Understand
CONTENTS: Foreword Acknowledgements Chapter 1: The Southwestern Corner Chapter 2: The Great Northern Peninsula Chapter 3: Labrador Chapter 4: Deer Lake to Bishop's Falls Chapter 5: Botwood to Twillingate Chapter 6: Glenwood to Gambo Chapter 7: Glovertown to Bonavista Chapter 8: The South Coast Chapter 9: Goobies to Cape St. Mary's to Whitbourne Chapter 10: Trinity-Conception Chapter 11: St. John's and the Eastern Avalon FOREWORD This book was written to give students a closer look at Newfoundland and Labrador. Learning about our own part of the earth can help us get a better understanding of the world at large. Much of the information now available about our province is aimed at young readers and people with at least a high school education. The Hitch-Hiker is intended to provide information which beginning adult readers can read and understand. This work has a special feature we hope readers will appreciate and enjoy. Many of the places written about in this book are seen through the eyes of an adult learner and other fictional characters. These characters were created to help add a touch of reality to the printed page. We hope the characters and the things they learn and talk about also give the reader a better understanding of our province. Above all, we hope this book challenges your curiosity and encourages you to search for more information about our land. Don McDonald Director of Programs and Services Newfoundland and Labrador Literacy Development Council ACKNOWLEDGMENTS I wish to thank the many people who so kindly and eagerly helped me during the production of this book.