Plasma Noradrenaline Levels
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Genl:VE 1970 © World Health Organization 1970
Nathan B. Eddy, Hans Friebel, Klaus-Jiirgen Hahn & Hans Halbach WORLD HEALTH ORGANIZATION ORGANISATION .MONDIALE DE LA SANT~ GENl:VE 1970 © World Health Organization 1970 Publications of the World Health Organization enjoy copyright protection in accordance with the provisions of Protocol 2 of the Universal Copyright Convention. Nevertheless governmental agencies or learned and professional societies may reproduce data or excerpts or illustrations from them without requesting an authorization from the World Health Organization. For rights of reproduction or translation of WHO publications in toto, application should be made to the Division of Editorial and Reference Services, World Health Organization, Geneva, Switzerland. The World Health Organization welcomes such applications. Authors alone are responsible for views expressed in signed articles. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the Director-General of the World Health Organization concerning the legal status of any country or territory or of its authorities, or concerning the delimitation of its frontiers. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. © Organisation mondiale de la Sante 1970 Les publications de l'Organisation mondiale de la Sante beneficient de la protection prevue par les dispositions du Protocole n° 2 de la Convention universelle pour la Protection du Droit d'Auteur. Les institutions gouvernementales et les societes savantes ou professionnelles peuvent, toutefois, reproduire des donnees, des extraits ou des illustrations provenant de ces publications, sans en demander l'autorisation a l'Organisation mondiale de la Sante. Pour toute reproduction ou traduction integrate, une autorisation doit etre demandee a la Division des Services d'Edition et de Documentation, Organisation mondiale de la Sante, Geneve, Suisse. -
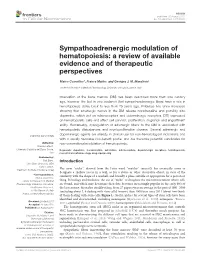
Sympathoadrenergic Modulation of Hematopoiesis: a Review of Available Evidence and of Therapeutic Perspectives
REVIEW published: 05 August 2015 doi: 10.3389/fncel.2015.00302 Sympathoadrenergic modulation of hematopoiesis: a review of available evidence and of therapeutic perspectives Marco Cosentino*, Franca Marino and Georges J. M. Maestroni Center for Research in Medical Pharmacology, University of Insubria, Varese, Italy Innervation of the bone marrow (BM) has been described more than one century ago, however the first in vivo evidence that sympathoadrenergic fibers have a role in hematopoiesis dates back to less than 25 years ago. Evidence has since increased showing that adrenergic nerves in the BM release noradrenaline and possibly also dopamine, which act on adrenoceptors and dopaminergic receptors (DR) expressed on hematopoietic cells and affect cell survival, proliferation, migration and engraftment ability. Remarkably, dysregulation of adrenergic fibers to the BM is associated with hematopoietic disturbances and myeloproliferative disease. Several adrenergic and dopaminergic agents are already in clinical use for non-hematological indications and with a usually favorable risk-benefit profile, and are therefore potential candidates for Edited by: non-conventional modulation of hematopoiesis. Wanda Lattanzi, Università Cattolica del Sacro Cuore, Keywords: dopamine, noradrenaline, adrenaline, adrenoceptors, dopaminergic receptors, hematopoiesis, Italy neuroimmune phamacology, drug repurposing Reviewed by: Sujit Basu, Introduction Ohio State University, USA Tsvee Lapidot, Weizmann Institute of Science, Israel The term ‘‘niche’’, derived from the Latin word ‘‘mytilus’’ (mussel), has eventually come to designate a shallow recess in a wall, as for a statue or other decorative object, in view of the *Correspondence: similarity with the shape of a seashell, and broadly a place suitable or appropriate for a person or Marco Cosentino, Center for Research in Medical thing. -

(12) United States Patent (10) Patent No.: US 9,376.418 B2 Haidle Et Al
USOO9376418B2 (12) United States Patent (10) Patent No.: US 9,376.418 B2 Haidle et al. (45) Date of Patent: Jun. 28, 2016 (54) SUBSTITUTED PYRIDINE SPLEEN 31/5377 (2013.01); A61K3I/5383 (2013.01); TYROSINE KINASE (SYK) INHIBITORS A61 K3I/551 (2013.01); A61K 45/06 (2013.01); C07D401/14 (2013.01); C07D (71) Applicants: Merck Sharp & Dohme Corp., 405/14 (2013.01); C07D 409/14 (2013.01); Rahway, NJ (US); Merck Canada Inc., C07D 413/14 (2013.01); C07D 417/14 Kirkland, Quebec (CA) (2013.01); C07D 471/04 (2013.01); (Continued) Inventors: (72) Andrew M. Haidle, Cambridge, MA (58) Field of Classification Search (US); Sandra Lee Knowles, Princeton, CPC ............... CO7D 401/12: CO7D 401/14: A61 K NJ (US); Solomon D. Kattar, Arlington, 31/5377; A61K31/506 MA (US); Denis Deschenes, Lachine USPC ........................ 544/122, 331; 514/235.8, 275 (CA); Jason Burch, Redwood City, CA See application file for complete search history. (US); Joel Robichaud, Dollard-des-Ormeaux (CA); Matthew (56) References Cited Christopher, Brookline, MA (US); Michael D. Altman, Needham, MA U.S. PATENT DOCUMENTS (US); James P. Jewell, Newtown, MA 5,710,129 A 1/1998 Lynch et al. (US); Alan B. Northrup, Reading, VA 6/2001 Uckun et al. (US); Marc Blouin, Saint-Lazare (CA); 6,248,790 B1 John Michael Ellis, Needham, MA (Continued) (US); Hua Zhou, Acton, MA (US); Christian Fischer, Natick, MA (US); FOREIGN PATENT DOCUMENTS Adam J. Schell, Decatur, GA (US); EP 877O2O A1 11, 1998 Michael H. Reutershan, Brookline, MA EP 2441755 A1 4/2012 (US); Brandon M. -

Marrakesh Agreement Establishing the World Trade Organization
No. 31874 Multilateral Marrakesh Agreement establishing the World Trade Organ ization (with final act, annexes and protocol). Concluded at Marrakesh on 15 April 1994 Authentic texts: English, French and Spanish. Registered by the Director-General of the World Trade Organization, acting on behalf of the Parties, on 1 June 1995. Multilat ral Accord de Marrakech instituant l©Organisation mondiale du commerce (avec acte final, annexes et protocole). Conclu Marrakech le 15 avril 1994 Textes authentiques : anglais, français et espagnol. Enregistré par le Directeur général de l'Organisation mondiale du com merce, agissant au nom des Parties, le 1er juin 1995. Vol. 1867, 1-31874 4_________United Nations — Treaty Series • Nations Unies — Recueil des Traités 1995 Table of contents Table des matières Indice [Volume 1867] FINAL ACT EMBODYING THE RESULTS OF THE URUGUAY ROUND OF MULTILATERAL TRADE NEGOTIATIONS ACTE FINAL REPRENANT LES RESULTATS DES NEGOCIATIONS COMMERCIALES MULTILATERALES DU CYCLE D©URUGUAY ACTA FINAL EN QUE SE INCORPOR N LOS RESULTADOS DE LA RONDA URUGUAY DE NEGOCIACIONES COMERCIALES MULTILATERALES SIGNATURES - SIGNATURES - FIRMAS MINISTERIAL DECISIONS, DECLARATIONS AND UNDERSTANDING DECISIONS, DECLARATIONS ET MEMORANDUM D©ACCORD MINISTERIELS DECISIONES, DECLARACIONES Y ENTEND MIENTO MINISTERIALES MARRAKESH AGREEMENT ESTABLISHING THE WORLD TRADE ORGANIZATION ACCORD DE MARRAKECH INSTITUANT L©ORGANISATION MONDIALE DU COMMERCE ACUERDO DE MARRAKECH POR EL QUE SE ESTABLECE LA ORGANIZACI N MUND1AL DEL COMERCIO ANNEX 1 ANNEXE 1 ANEXO 1 ANNEX -

Effect of Rutin on the Isolated Rat Duodenum and Comparison with the Effects of Adrenaline, Isoprenaline and Papaverine
Ankara Ezc. Fak. Der. J. Fac. Pharm. Ankara 17, 49 (1987) 17, 49 (1987) Effect of Rutin on the Isolated Rat Duodenum and Comparison with the Effects of Adrenaline, Isoprenaline and Papaverine. Rutin'in İzole Sıçan Duodenumu Üzerine Etkisi ve Adrenalin, İzo- prenalin, Papaverin ile Karşılaştırılması. Orhan ALTINKURT* Yusuf ÖZTÜRK** SUMMARY The experiments were performed by using isolated rat duodenum. Rutin, a natural flavonoid compound, caused relaxations of the rat duodenum dose-dependently. The relaxant effect of rutin on the rat duodenum was examined in comparison with that of adrenaline, iso- prenaline and papaverine. In addition, propranolol, a beta-adrener- gic blocking agent, phentolamine, an alpha-adrenergic blockingagent and nicotinic acid, an adenyl cyclase inhibitor were used as tools to investigate mechanism of the relaxant effect of rutin on the rat duo- denum in vitro. ÖZET Deneyler izole sıçan duodenumu kullanılarak sürdürüldü. Doğal bir flavonoid bileşiği olan rutin doza bağımlı biçimde sıçan duodenu- munu gevşetti. Rutin'in sıçan duodenumundaki gevşetici etkisi ad- renalin, izoprenalin ve papaverin ile karşılaştırmalı olarak incelendi. Ayrıca, rutin'in sıçan duodenumundaki gevşetici etkisinin mekaniz- masını araştırmak için beta-adrenerjik bloker olan propranolol, alfa- adrenerjik bloker olan fentolamin ve bir adenil siklaz inhibitörü olan nikotinik asid de kullanıldı. Key words: Rutin, Adrenaline, Isoprenaline, Papaverine, Phento- lamine, Propranolol, Nicotinic acid, Smooth muscle. Rutin is found in many plants, particularly extracts from Fagopyrum esculentum, Fagopyrum cymosum, Fagopyrum tataricum Redaksiyona verildiği tarih: 19.2.1987 * Dept. Pharmacol., Fac. Pharm., Univ. Ankara. ** Dept. Pharmacol., Fac. Pharm., Univ. Anatolia. SO Orhan ALTINKURT, Yusuf ÖZTÜRK (Polygonaceae), Ruta chalepensis, Ruta graveolens (Rutaceae) and Viola tricolor, Viola lutea splendens (Violaceae). -
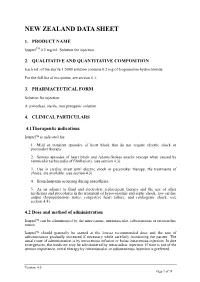
Data Sheet Template
NEW ZEALAND DATA SHEET 1. PRODUCT NAME IsuprelTM 0.2 mg/mL Solution for injection 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each mL of the sterile 1:5000 solution contains 0.2 mg of Isoprenaline hydrochloride. For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Solution for injection A colourless, sterile, non pyrogenic solution. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Isuprel is indicated for: 1. Mild or transient episodes of heart block that do not require electric shock or pacemaker therapy. 2. Serious episodes of heart block and Adams-Stokes attacks (except when caused by ventricular tachycardia of fibrillation). (see section 4.3). 3. Use in cardiac arrest until electric shock or pacemaker therapy, the treatments of choice, are available. (see section 4.3). 4. Bronchospasm occurring during anaesthesia. 5. As an adjunct to fluid and electrolyte replacement therapy and the use of other medicines and procedures in the treatment of hypovolaemic and septic shock, low cardiac output (hypoperfusion) states, congestive heart failure, and cardiogenic shock. (see section 4.4). 4.2 Dose and method of administration Isuprel can be administered by the intravenous, intramuscular, subcutaneous or intracardiac routes. Isuprel should generally be started at the lowest recommended dose and the rate of administration gradually increased if necessary while carefully monitoring the patient. The usual route of administration is by intravenous infusion or bolus intravenous injection. In dire emergencies, the medicine may be administered by intracardiac injection. If time is not of the utmost importance, initial therapy by intramuscular or subcutaneous injection is preferred. Version: 4.0 Page 1 of 11 Elderly patients may be more sensitive to the effects of sympathomimetics and lower doses may be required. -

OUH Formulary Approved for Use in Breast Surgery
Oxford University Hospitals NHS Foundation Trust Formulary FORMULARY (Y): the medicine can be used as per its licence. RESTRICTED FORMULARY (R): the medicine can be used as per the agreed restriction. NON-FORMULARY (NF): the medicine is not on the formulary and should not be used unless exceptional approval has been obtained from MMTC. UNLICENSED MEDICINE – RESTRICTED FORMULARY (UNR): the medicine is unlicensed and can be used as per the agreed restriction. SPECIAL MEDICINE – RESTRICTED FORMULARY (SR): the medicine is a “special” (unlicensed) and can be used as per the agreed restriction. EXTEMPORANEOUS PREPARATION – RESTRICTED FORMULARY (EXTR): the extemporaneous preparation (unlicensed) can be prepared and used as per the agreed restriction. UNLICENSED MEDICINE – NON-FORMULARY (UNNF): the medicine is unlicensed and is not on the formulary. It should not be used unless exceptional approval has been obtained from MMTC. SPECIAL MEDICINE – NON-FORMULARY (SNF): the medicine is a “special” (unlicensed) and is not on the formulary. It should not be used unless exceptional approval has been obtained from MMTC. EXTEMPORANEOUS PREPARATION – NON-FORMULARY (EXTNF): the extemporaneous preparation (unlicensed) cannot be prepared and used unless exceptional approval has been obtained from MMTC. CLINICAL TRIALS (C): the medicine is clinical trial material and is not for clinical use. NICE TECHNOLOGY APPRAISAL (NICETA): the medicine has received a positive appraisal from NICE. It will be available on the formulary from the day the Technology Appraisal is published. Prescribers who wish to treat patients who meet NICE criteria, will have access to these medicines from this date. However, these medicines will not be part of routine practice until a NICE TA Implementation Plan has been presented and approved by MMTC (when the drug will be given a Restricted formulary status). -

Federal Register / Vol. 60, No. 80 / Wednesday, April 26, 1995 / Notices DIX to the HTSUS—Continued
20558 Federal Register / Vol. 60, No. 80 / Wednesday, April 26, 1995 / Notices DEPARMENT OF THE TREASURY Services, U.S. Customs Service, 1301 TABLE 1.ÐPHARMACEUTICAL APPEN- Constitution Avenue NW, Washington, DIX TO THE HTSUSÐContinued Customs Service D.C. 20229 at (202) 927±1060. CAS No. Pharmaceutical [T.D. 95±33] Dated: April 14, 1995. 52±78±8 ..................... NORETHANDROLONE. A. W. Tennant, 52±86±8 ..................... HALOPERIDOL. Pharmaceutical Tables 1 and 3 of the Director, Office of Laboratories and Scientific 52±88±0 ..................... ATROPINE METHONITRATE. HTSUS 52±90±4 ..................... CYSTEINE. Services. 53±03±2 ..................... PREDNISONE. 53±06±5 ..................... CORTISONE. AGENCY: Customs Service, Department TABLE 1.ÐPHARMACEUTICAL 53±10±1 ..................... HYDROXYDIONE SODIUM SUCCI- of the Treasury. NATE. APPENDIX TO THE HTSUS 53±16±7 ..................... ESTRONE. ACTION: Listing of the products found in 53±18±9 ..................... BIETASERPINE. Table 1 and Table 3 of the CAS No. Pharmaceutical 53±19±0 ..................... MITOTANE. 53±31±6 ..................... MEDIBAZINE. Pharmaceutical Appendix to the N/A ............................. ACTAGARDIN. 53±33±8 ..................... PARAMETHASONE. Harmonized Tariff Schedule of the N/A ............................. ARDACIN. 53±34±9 ..................... FLUPREDNISOLONE. N/A ............................. BICIROMAB. 53±39±4 ..................... OXANDROLONE. United States of America in Chemical N/A ............................. CELUCLORAL. 53±43±0 -

Cannabinoid CB1 and CB2 Receptors Antagonists AM251 and AM630
Pharmacological Reports 71 (2019) 82–89 Contents lists available at ScienceDirect Pharmacological Reports journal homepage: www.elsevier.com/locate/pharep Original article Cannabinoid CB1 and CB2 receptors antagonists AM251 and AM630 differentially modulate the chronotropic and inotropic effects of isoprenaline in isolated rat atria Jolanta Weresa, Anna Pe˛dzinska-Betiuk, Rafał Kossakowski, Barbara Malinowska* Department of Experimental Physiology and Pathophysiology, Medical University of Bialystok, Białystok, Poland A R T I C L E I N F O A B S T R A C T Article history: Background: Drugs targeting CB1 and CB2 receptors have been suggested to possess therapeutic benefit in Received 28 May 2018 cardiovascular disorders associated with elevated sympathetic tone. Limited data suggest cannabinoid Received in revised form 31 July 2018 ligands interact with postsynaptic β-adrenoceptors. The aim of this study was to examine the effects of Accepted 14 September 2018 CB1 and CB2 antagonists, AM251 and AM630, respectively, at functional cardiac β-adrenoceptors. Available online 17 September 2018 Methods: Experiments were carried out in isolated spontaneously beating right atria and paced left atria where inotropic and chronotropic increases were induced by isoprenaline and selective agonists of β1 and Keywords: β -adrenergic receptors. β-Adrenoceptor 2 Results: We found four different effects of AM251 and AM630 on the cardiostimulatory action of Cannabinoid receptor m AM251 isoprenaline: (1) both CB receptor antagonists 1 M enhanced the isoprenaline-induced increase in atrial AM630 rate, and AM630 1 mM enhanced the inotropic effect of isoprenaline; (2) AM251 1 mM decreased the Atria efficacy of the inotropic effect of isoprenaline; (3) AM251 0.1 and 3 mM and AM630 3 mM reduced the isoprenaline-induced increases in atrial rate; (4) AM630 0.1 and 3 mM enhanced the inotropic effect of isoprenaline, which was not changed by the same concentrations of AM251. -

Pharmacology
STATE ESTABLISHMENT «DNIPROPETROVSK MEDICAL ACADEMY OF HEALTH MINISTRY OF UKRAINE» V.I. MAMCHUR, V.I. OPRYSHKO, А.А. NEFEDOV, A.E. LIEVYKH, E.V.KHOMIAK PHARMACOLOGY WORKBOOK FOR PRACTICAL CLASSES FOR FOREIGN STUDENTS STOMATOLOGY DEPARTMENT DNEPROPETROVSK - 2016 2 UDC: 378.180.6:61:615(075.5) Pharmacology. Workbook for practical classes for foreign stomatology students / V.Y. Mamchur, V.I. Opryshko, A.A. Nefedov. - Dnepropetrovsk, 2016. – 186 p. Reviewed by: N.I. Voloshchuk - MD, Professor of Pharmacology "Vinnitsa N.I. Pirogov National Medical University.‖ L.V. Savchenkova – Doctor of Medicine, Professor, Head of the Department of Clinical Pharmacology, State Establishment ―Lugansk state medical university‖ E.A. Podpletnyaya – Doctor of Pharmacy, Professor, Head of the Department of General and Clinical Pharmacy, State Establishment ―Dnipropetrovsk medical academy of Health Ministry of Ukraine‖ Approved and recommended for publication by the CMC of State Establishment ―Dnipropetrovsk medical academy of Health Ministry of Ukraine‖ (protocol №3 from 25.12.2012). The educational tutorial contains materials for practical classes and final module control on Pharmacology. The tutorial was prepared to improve self-learning of Pharmacology and optimization of practical classes. It contains questions for self-study for practical classes and final module control, prescription tasks, pharmacological terms that students must know in a particular topic, medical forms of main drugs, multiple choice questions (tests) for self- control, basic and additional references. This tutorial is also a student workbook that provides the entire scope of student’s work during Pharmacology course according to the credit-modular system. The tutorial was drawn up in accordance with the working program on Pharmacology approved by CMC of SE ―Dnipropetrovsk medical academy of Health Ministry of Ukraine‖ on the basis of the standard program on Pharmacology for stomatology students of III - IV levels of accreditation in the specialties Stomatology – 7.110105, Kiev 2011. -

Beta Adrenergic Receptor of Rabbit Thoracic Aorta in Relation to Age
Japan. J. Pharmacol. 23, 259-268 (1973) 259 BETA ADRENERGIC RECEPTOR OF RABBIT THORACIC AORTA IN RELATION TO AGE O.D. GULATI, B.P. METHEW, ELM. PARIKH* and V.S.R. KRISHNAMURTY** Pharmacological Research Unit, Council of Scientific and Industrial Research and Department of Pharmacology, Medical College, Baroda, India Accepted October 16, 1972 Abstract-Isolated aortic strips from rabbits older than 6 months (1.7-2.5 kg) when subjected to contraction by noradrenaline or adrenaline were relaxed by isoprenaline. The relaxation was not blocked by propranolol. When these strips were contracted by potassium chloride, isoprenaline produced a small relaxation which was sensitive to propranolol. In aortic strips from rabbits 2-3 months old (0.75-0.95 kg), the contraction produced by noradrenaline or potassium chloride was relaxed by isopre- naline; isoprenaline was equally active against both stimulants. Propranolol anta- gonised the action of isoprenaline competitively, with a pA2 value, 7.05. In strips from rabbitsfrom a lower age group, the pA2 values of phentolamine against isopre- naline and methoxamine contractions were 7.61 and 7.50 respectively. It is concluded that aortas of rabbits older than 6 months are almost devoid of beta adrenergic re- ceptors whereas those of rabbits 2-3 months old contain both alpha and beta adre- nergic receptors. Vascular smooth muscle has both alpha and beta adrenergic receptors (1). Isoprena- line, the most potent vasodilator sympathomimetic amine (2) produces both vasocon- striction and vasodilation in rabbits (1). Furchgott (3, 4) and Furchgott and Bhadrakom (5) first demonstrated that in high concentrations, isoprenaline (4 •~ 10-6 -2 •~ 10-3 M) caused contraction of isolated rabbit thoracic aorta similar to that produced by adrenaline and noradrenaline. -

1. NAME of the DRUG Isoprenaline Hydrochloride S.A.L.F. 0.2 Mg/Ml Solution for Injection
1. NAME OF THE DRUG Isoprenaline hydrochloride S.A.L.F. 0.2 mg/ml solution for injection 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each ampoule contains: Active ingredient: Isoprenaline hydrochloride 0.2 mg. For a full list of the excipients, see section 6.1. 3. PHARMACEUTICAL FORM Solution for injection. The solution is clear and colorless. 4. CLINICAL INFORMATION 4.1 Therapeutic indications Treatment for total atrioventricular block (including the Stokes-Adams syndrome) and cardiac arrest. Treatment for bronchospasm during anesthesia. In addition to a treatment for cardiogenic shock. 4.2 Posology and method of administration Treatment for total atrioventricular block (including the Stokes-Adams syndrome) and cardiac arrest. Intramuscular administration: 0.2 mg followed by 0.02 to 1.0 mg depending on the patient's response. Intravenous administration: 2-10 micrograms/min, which could be adjusted according to the patient's response. Subcutaneous administration: 0.2 mg followed by 0.15-0.2 mg depending on the patient’s response. Treatment for bronchospasm during anesthesia. Intravenous administration: initial dose 0.01-0.02 mg, repeated if necessary. In addition to a treatment for cardiogenic shock. Intravenous administration: 0.5-5 micrograms/min, depending on the patient's response. Higher doses (up to 20 micrograms/minute) can be sometimes used in severe states of shock according to the clinical conditions and the patient's response. The use of Isoprenaline is not recommended in children due to a lack of data on safety and efficacy. Instructions for use For intravenous injection Dilute 1 ml of Isoprenaline hydrochloride 0.2 mg/ml solution for injection with 10 ml of 0.9% sodium chloride or 5% glucose to obtain a solution with a concentration of 0.02 mg/ml.