Studies of Sweating
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

1 Structure and Function of the Skin
Go Back to the Top To Order, Visit the Purchasing Page for Details 1 Chapter 1 Structure and Function of the Skin The skin is the human body’s its largest organ, covering 1.6 m2 of surface area and accounting for approximate- ly 16% of an adult’s body weight. In direct contact with the outside environment, the skin helps to maintain four essential bodily functions: ① retention of moisture and prevention of permeation or loss of other molecules, ② regulation of body temperature, ③ protection of the body from microbes and harmful external influences, and ④ sensation. To understand cutaneous biology and skin diseases, it is very important to learn the structure and functions of normal human skin. A. Skin surface The skin surface is not smooth, but is laced with multiple net- works of fine grooves called sulci cutis. These can be deep or shallow. The slightly elevated areas that are surrounded by shal- lower areas of sulci cutis are called cristae cutis. Sweat pores fed crista cutis by the sweat glands open to the cristae cutis (Fig. 1.1). The orientation of the sulci cutis, which differs depending on body location, is called the dermal ridge pattern. Fingerprints and sulcus cutis patterns on the palms and soles, which are unique to each person, are formed by the sulci cutis. Elastic fibers also run in specific directions in deeper parts of the skin, with the direction depend- aabcdefg h i j klmnopqr ing on the site. Some skin diseases, such as epidermal nevus, are known to occur along specific lines distributed over the body, the Blaschko lines (Fig. -

Dermoscopy of Aplasia Cutis Congenita: a Case Report and Review of the Literature
Dermatology Practical & Conceptual Dermoscopy of Aplasia Cutis Congenita: A Case Report and Review of the Literature Rasna Neelam1, Mio Nakamura2, Trilokraj Tejasvi2 1 University of Michigan Medical School, Ann Arbor, MI, USA 2 Department of Dermatology, University of Michigan, Ann Arbor, MI, USA Key words: aplasia cutis congenita, alopecia, dermoscopy, trichoscopy Citation: Neelam R, Nakamura M, Tejasvi T. Dermoscopy of aplasia cutis congenita: a case report and review of the literature. Dermatol Pract Concept. 2021;11(1):e2021154. DOI: https://doi.org/10.5826/dpc.1101a154 Accepted: September 28, 2020; Published: January 29, 2021 Copyright: ©2021 Neelam et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License BY-NC-4.0, which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited. Funding: None. Competing interests: The authors have no conflicts of interest to disclose. Authorship: All authors have contributed significantly to this publication. Corresponding author: Trilokraj Tejasvi, MD, Department of Dermatology, University of Michigan, 1910 Taubman Center, 1500 E. Medical Center Dr, Ann Arbor, MI 48109, USA Email: [email protected] Introduction throbbing, and point tenderness in one of the patches of alo- pecia. The alopecic patch had been present on the right pari- Aplasia cutis congenita (ACC) is a rare heterogeneous con- etal-occipital scalp since birth and has been stable in size and genital disorder characterized by focal or widespread absence appearance for years. Three other round patches of alopecia of the skin. had also been present since birth and remained asymptomatic. -

A Case of Acquired Smooth Muscle Hamartoma on the Sole
Ann Dermatol (Seoul) Vol. 21, No. 1, 2009 CASE REPORT A Case of Acquired Smooth Muscle Hamartoma on the Sole Deborah Lee, M.D., Sang-Hyun Kim, M.D., Soon-Kwon Hong, M.D., Ho-Suk Sung, M.D., Seon-Wook Hwang, M.D. Department of Dermatology, Busan Paik Hospital, College of Medicine, Inje University, Busan, Korea A smooth muscle hamartoma is a benign proliferation of INTRODUCTION smooth muscle bundles within the dermis. It arises from smooth muscle cells that are located in arrector pili muscles, Smooth muscle hamartomas (SMH) are a result of benign dartos muscles, vascular smooth muscles, muscularis proliferation of smooth muscle bundles in the dermis. SMH- mammillae and the areolae. Acquired smooth muscle associated smooth muscle cells originate from arrector hamartoma (ASMH) is rare, with only 10 such cases having pili-, dartos-, vulvar-, mammillary- and vascular wall- been reported in the English medical literature to date. Most muscles1-3. SMH is characterized by slightly pigmented of these cases of ASMH were shown to have originated from plaques that contain vellus hairs, and SMH is subdivided arrector pili and dartos muscles. Only one case was reported into two types: congenital smooth muscle hamartoma to have originated from vascular smooth muscle cells. A 21 (CSMH) and acquired smooth muscle hamartoma (ASMH)1-3. year-old woman presented with a tender pigmented nodule, ASMH is a very rare form of SMH that was first described with numbness, on the sole of her foot, and this lesion had by Wong and Solomon1 in 1985, with only such 10 cases developed over the previous 18 months. -

Atypical Variants of Mycosis Fungoides
Altınışık et al. Atypical Variants of Mycosis Fungoides REVIEW DOI: 10.4274/jtad.galenos.2021.09719 J Turk Acad Dermatol 2021;15(2):30-33 Atypical Variants of Mycosis Fungoides Dursun Dorukhan Altınışık, Özge Aşkın, Tuğba Kevser Uzunçakmak, Burhan Engin Istanbul University-Cerrahpasa, Cerrahpasa Faculty of Medicine, Department of Dermatology, Istanbul, Turkey ABSTRACT Mycosis fungoides (MF) is the most common type of cutaneous T-cell lymphoma (CTCL) and it is characterised by specific histological features. MF is in a spectrum of disorders which includes Sezary syndrome and other CTCL subtypes. Clinically and histopathologically it can imitate other T-cell mediated dermatosis hence making its diagnosis difficult. Due to different prognosis and difference in treatment strategies other subtypes of CTCL must be differentiated from MF. MF is a clinically indolent low-grade lymphoma which is seen in people aged between 55- 60 and it’s seen more commonly in men (2:1 ratio). Meanwhile other subtypes of MF like folliculotropic variant may show relatively a more aggressive course and our treatment strategy may differ. Keywords: Mycosis fungoides, Cutaneous T-cell lymphoma, Phototherapy, PUVA Introduction follicles frequently causing alopecia and in the paediatric population Mycosis fungoides (MF) is the most common type of cutaneous T-cell it tends to accompany hypopigmented patches and plaques. FMF lymphoma (CTCL) and it is characterised by specific histological preferentially involves the head and neck region however it can features [1]. MF is in a spectrum of disorders which includes Sezary sometimes involve the trunk or the extremities [6]. Patients with syndrome and other CTCL subtypes. Clinically and histopathologically FMF have significant pruritus which may be overlapped by S. -

Gen Anat-Skin
SKIN • Cutis,integument • External covering • Skin+its appendages-- -integumentary system • Largest organ---15 to 20% body mass. LAYERS • Epidermis •Dermis Types • Thick and thin(1-5 mm thick) • Hairy and non hairy Thick skin EXAMPLES • THICK---PALMS AND SOLES BUT ANATOMICALLY THE BACK HAS THICK SKIN. REST OF BODY HAS THIN SKIN • NON HAIRY----PALMS AND SOLES,DORSAL SURFACE OF DISTAL PHALANX,GLANS PENIS,LABIA MINORA,LABIA MAJORA AND UMBLICUS FUNCTIONS • Barrier • Immunologic • Homeostasis •Sensory • Endocrine • excretory EPIDERMIS(layers) • Stratum basale or stratum germinativum • Stratum spinosum • Stratum granulosum • Stratum lucidum • Stratum corneum Type of cells in epidermis and keratinization • Keratinocytes • Melanocytes • Langerhans • Merkels cells DERMIS LAYERS---- 1.PAPILLARY • Dermal papillae • Complementary epidermal ridges or rete ridges • Dermal ridges in thick skin • Hemidesmosomes present both in dermis and epidermis RETICULAR LAYER •DENSE IRREGULAR CONNECTIVE TIISUE Sensory receptors • Free nerve endings • Ruffini end organs • Pacinian and • Meissners corpuscles Blood supply • Fasciocutaneous A • Musculocutaneous A • Direct cutaneous A APPENDAGES • Hair follicle producing hair • Sweat glands(sudoriferous) • Sebaceous glands • Nails Hair follicle • Invagination of epidermis • Parts---infundibulum, isthmus, inferior part having bulb and invagination HAIR follicle layers • Outer and inner root sheath • Types of hair vellus, terminal, club • Phases of growth— anagen, catagen and telogen Hair shaft • Cuticle •Cortex • Medulla -

Lichen Spinulosus: Case Report and Review of Literatures
Journal of Health Science 2015, 5(3A): 20-22 DOI: 10.5923/s.health.201501.07 Lichen Spinulosus: Case Report and Review of Literatures Khalid Al Hawsawi1,*, Kholood Almehmadi2, Bushra Alraddadi3, Ohood Aljuhani2 1Dermatology Consultant, Head of Dermatology Department, King Abdul Aziz Hospital, Makkah, Saudi Arabia 2Medical intern, King Abdul Aziz Hospital, Makkah, Saudi Arabia 3Dermatology Resident, King Abdul Aziz Hospital, Makkah, Saudi Arabia Abstract Lichen Spinulosus is a rare childhood disease. It is characterized by follicular hyperkeratotic papules that may coalesce into plaques. Individual lesion shows conical projection, hair like horny spine. The etiology is unknown but genetic predisposition has been suggested as a possible cause. It has a tendency to disappear spontaneously at puberty. Herein we present a 12-year-old boy presented with 6- month- history of persistent asymptomatic skin lesions. Skin examinations revealed multiple grouped scaly, hypopigmented tiny follicular papules with horny spines on his back. Soles showed planter keratoderma. Skin biopsy showed dilated hair follicle filled with keratin plugging. Diagnosis of LS associated with planter keratoderma was made. The patient responded well to topical lactic acid (12%), urea (20-30%), and betamethasone valerate (0.1%) preparations. Keywords Lichen spinulosa, Lichen Spinulosus 1. Introduction appearance. LS usually involves extensor surfaces of arms, trochanteric regions, neck, abdomen, buttocks, thigh, Lichen spinulosus (LS) is a genetic disorder of popliteal fossae, and knees. The histopathology of the lesion is not specific showing dilated hair follicle with keratin keratinization of hair follicles. LS was first described by Adamson in 1908. [1] It is a member of the family of plugging. -

Differentiating Keratosis Follicularis Spinulosa Decalvans from Monilithrix : Two Rare Causes of Scarring Alopecia in Young Male Siblings
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 18, Issue 5 Ser. 7 (May. 2019), PP 01-03 www.iosrjournals.org Differentiating Keratosis Follicularis Spinulosa Decalvans From Monilithrix : Two Rare Causes Of Scarring Alopecia In Young Male Siblings. 1 2 3 4 5 Heena Singdia , Rohit Garg , Sinni Jain , Vijay Paliwal , Puneet Bhargava , Deepak Mathur6 1,2,3,4,5,6(Department of dermatology, venereology and leprology, SMS Medical College, India) Corresponding Author: Heena Singdia Abstract: Keratosis follicularis spinulosa decalvans (KFSD) is a rare disorder affecting the hair follicles characterized by progressive cicatricial alopecia of the scalp and eyebrows, with usually X-linked recessive mode of transmission hence predominantly affecting Males.[1] Monilethrix is a rare structural Hair shaft disorder with autosomal dominant mode of transmission, characterized by short, fragile, brittle hair that breaks spontaneously resulting in patchy dystrophic alopecia.[2] Key words: Keratosis Follicularis Spinulosa Decalvans, Monilithrix, Hereditary Scarring Alopecias --------------------------------------------------------------------------------------------------------------------------------------- Date of Submission: 02-05-2019 Date of acceptance: 16-05-2019 --------------------------------------------------------------------------------------------------------------------------------------------------- I. Introduction KFSD is a rare type of primary scarring alopecia with lymphocytic predominance. -

5 Allergic Diseases (And Differential Diagnoses)
Chapter 5 5 Allergic Diseases (and Differential Diagnoses) 5.1 Diseases with Possible IgE Involve- tions (combination of type I and type IVb reac- ment (“Immediate-Type Allergies”) tions). Atopic eczema will be discussed in a separate section (see Sect. 5.5.3). There are many allergic diseases manifesting in The maximal manifestation of IgE-mediated different organs and on the basis of different immediate-type allergic reaction is anaphylax- pathomechanisms (see Sect. 1.3). The most is. In the development of clinical symptoms, common allergies develop via IgE antibodies different organs may be involved and symp- and manifest within minutes to hours after al- toms of well-known allergic diseases of skin lergen contact (“immediate-type reactions”). and mucous membranes [also called “shock Not infrequently, there are biphasic (dual) re- fragments” (Karl Hansen)] may occur accord- action patterns when after a strong immediate ing to the severity (see Sect. 5.1.4). reactioninthecourseof6–12harenewedhy- persensitivity reaction (late-phase reaction, LPR) occurs which is triggered by IgE, but am- 5.1.1 Allergic Rhinitis plified by recruitment of additional cells and 5.1.1.1 Introduction mediators.TheseLPRshavetobedistin- guished from classic delayed-type hypersensi- Apart from being an aesthetic organ, the nose tivity (DTH) reactions (type IV reactions) (see has several very interesting functions (Ta- Sect. 5.5). ble 5.1). It is true that people can live without What may be confusing for the inexperi- breathing through the nose, but disturbance of enced physician is familiar to the allergist: The this function can lead to disease. Here we are same symptoms of immediate-type reactions interested mostly in defense functions against are observed without immune phenomena particles and irritants (physical or chemical) (skin tests or IgE antibodies) being detectable. -

Disseminate and Recurrent Infundibulo-Folliculitis
Letters to the Editor 75 Disseminate and Recurrent Infundibulo-folliculitis Mar´õ a Isabel Longo1, Manuel Lecona2 and Pablo La´zaro1 Departments of 1Dermatology and 2Pathology, Hospital Grogorio Maran˜on, C/Dr. Esquerdo 46, ES-28007 Madrid, Spain. E-mail: [email protected] Accepted December 17, 2001. Sir, Disseminate and recurrent infundibulo-folliculitis is an infrequent entity of unknown etiology rst described in 1968 by Hitch & Lund (1). Most patients are young Black male adults, although it has also been described in Whites and in women (2, 3). Lesions are usually esh-coloured, small follicular papules with smooth surface and that do not coalesce. They predominate in the trunk and the proximal part of extremities. Symptoms are highly variable, but mild pruritus is commonly referred. The majority of patients lack any personal or family history of skin diseases such as atopic dermatitis. We here describe a case of disseminate and recurrent infundibulo-folliculitis in a Black woman. CASE REPORT A 25-year-old Black woman was referred for evaluation of a slightly pruritic, recurrent eruption of 7 months’ duration. She had no personal or family history of skin diseases. Physical examination revealed multiple small follicular papules symmetrically distributed over the chest, abdomen and back. In some areas the lesions were arranged following the lines of cleavage (Fig. 1). A biopsy specimen showed follicular spongiosis, exocytosis of lymphocytes and a subtle lymphocytic in ammatory in ltrate around follicles and blood vessels in the super cial dermis (Fig. 2). DISCUSSION Fig. 2. Follicular spongiosis with exocytosis of lymphocytes and a Disseminate and recurrent infundibulo-folliculitis is a perifollicular and perivascular lymphocytic in ltrate. -
Aafp Fmx 2020
Challenging Pediatric Rashes Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery University of Texas Health, San Antonio 1 ACTIVITY DISCLAIMER The material presented here is being made available by the American Academy of Family Physicians for educational purposes only. Please note that medical information is constantly changing; the information contained in this activity was accurate at the time of publication. This material is not intended to represent the only, nor necessarily best, methods or procedures appropriate for the medical situations discussed. Rather, it is intended to present an approach, view, statement, or opinion of the faculty, which may be helpful to others who face similar situations. The AAFP disclaims any and all liability for injury or other damages resulting to any individual using this material and for all claims that might arise out of the use of the techniques demonstrated therein by such individuals, whether these claims shall be asserted by a physician or any other person. Physicians may care to check specific details such as drug doses and contraindications, etc., in standard sources prior to clinical application. This material 2 might contain recommendations/guidelines developed by other organizations. Please note that although these guidelines might be included, this does not necessarily imply the endorsement by the AAFP. 2 1 Disclosure Statement It is the policy of the AAFP that all individuals in a position to control content disclose any relationships with commercial interests upon nomination/invitation of participation. Disclosure documents are reviewed for potential conflicts of interest. If conflicts are identified, they are resolved prior to confirmation of participation. -
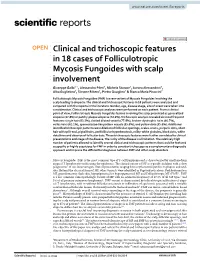
Clinical and Trichoscopic Features in 18 Cases of Folliculotropic Mycosis Fungoides with Scalp Involvement
www.nature.com/scientificreports OPEN Clinical and trichoscopic features in 18 cases of Folliculotropic Mycosis Fungoides with scalp involvement Giuseppe Gallo1*, Alessandro Pileri2, Michela Starace2, Aurora Alessandrini2, Alba Guglielmo2, Simone Ribero1, Pietro Quaglino1 & Bianca Maria Piraccini2 Folliculotropic Mycosis Fungoides (FMF) is a rare variant of Mycosis Fungoides involving the scalp leading to alopecia. The clinical and trichoscopic features in 18 patients were analyzed and compared with the reports in the literature. Gender, age, disease stage, site of onset were taken into consideration. Clinical and trichoscopic analyses were performed on each patient. From a clinical point of view, Folliculotropic Mycosis Fungoides lesions involving the scalp presented as generalized alopecia (27.8%) or patchy-plaque alopecia (72.2%). Trichoscopic analysis revealed six most frequent features: single hair (83.3%), dotted dilated vessels (77.8%), broken-dystrophic hairs (66.7%), vellus hairs (61.1%), spermatozoa-like pattern vessels (55.6%), and yellow dots (55.6%). Additional identifed trichoscopic patterns were dilation of follicular openings, scales-crusts, purpuric dots, short hair with split-end, pigtail hairs, perifollicular hyperkeratosis, milky-white globules, black dots, white dots/lines and absence of follicular dots. These trichoscopic features were further correlated to clinical presentations and stage of the disease. The rarity of the disease is a limitation. The relatively high number of patients allowed to identify several clinical and trichoscopic patterns that could be featured as specifc or highly suspicious for FMF in order to consider trichoscopy as a complementary diagnostic approach and improve the diferential diagnoses between FMF and other scalp disorders. Mycosis Fungoides (MF) is the most common type of T-cell lymphoma and is characterized by small-medium atypical T lymphocytes infltrating the epidermis. -

Nails in Systemic Disease
CME: DERMATOLOGY Clinical Medicine 2021 Vol 21, No 3: 166–9 Nails in systemic disease Authors: Charlotte E GollinsA and David de BerkerB A change in colour, size, shape or texture of finger- and MatrixCuticle toenails can be an indicator of underlying systemic disease. Nail plate An appreciation of these nail signs, and an ability to interpret them when found, can help guide diagnosis and management Nail bed of a general medical patient. This article discusses some ABSTRACT common, and some more rare, nail changes associated with systemic disease. Proximal nail fold Introduction Cuticle Examination of nails is a skill that, although emphasised when Matrix (lunula) revising for general medical exams, can be overlooked in day- Nail plate Lateral nail fold to-day practice. The value of noticing, understanding and Onychocorneal interpreting nail changes can positively add to clinical practice as band these signs can provide valuable clues to a diagnosis. Here we present a brief overview of selected common and rarer Fig 1. Anatomy of the nail plate. nail abnormalities associated with systemic conditions, as well as a limited explanation of the pathophysiology of some of the changes. Anatomy of the nail unit located in the distal third of the nail plate. They are caused The nail unit (Fig 1) is an epithelial skin appendage composed by damage to capillaries within the nail bed, which have a of the hardened nail plate surrounded by specialised epithelial longitudinal orientation, leading to their linear appearance. In the surfaces that contribute to its growth and maintenance.1 The nail case of bacterial endocarditis, this damage is likely to be caused by plate is formed of keratinised epithelial cells.