Gastrointestinal Microbiota Community Composition Has Significant Effects on Systemic Immune Responses
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The 2014 Golden Gate National Parks Bioblitz - Data Management and the Event Species List Achieving a Quality Dataset from a Large Scale Event
National Park Service U.S. Department of the Interior Natural Resource Stewardship and Science The 2014 Golden Gate National Parks BioBlitz - Data Management and the Event Species List Achieving a Quality Dataset from a Large Scale Event Natural Resource Report NPS/GOGA/NRR—2016/1147 ON THIS PAGE Photograph of BioBlitz participants conducting data entry into iNaturalist. Photograph courtesy of the National Park Service. ON THE COVER Photograph of BioBlitz participants collecting aquatic species data in the Presidio of San Francisco. Photograph courtesy of National Park Service. The 2014 Golden Gate National Parks BioBlitz - Data Management and the Event Species List Achieving a Quality Dataset from a Large Scale Event Natural Resource Report NPS/GOGA/NRR—2016/1147 Elizabeth Edson1, Michelle O’Herron1, Alison Forrestel2, Daniel George3 1Golden Gate Parks Conservancy Building 201 Fort Mason San Francisco, CA 94129 2National Park Service. Golden Gate National Recreation Area Fort Cronkhite, Bldg. 1061 Sausalito, CA 94965 3National Park Service. San Francisco Bay Area Network Inventory & Monitoring Program Manager Fort Cronkhite, Bldg. 1063 Sausalito, CA 94965 March 2016 U.S. Department of the Interior National Park Service Natural Resource Stewardship and Science Fort Collins, Colorado The National Park Service, Natural Resource Stewardship and Science office in Fort Collins, Colorado, publishes a range of reports that address natural resource topics. These reports are of interest and applicability to a broad audience in the National Park Service and others in natural resource management, including scientists, conservation and environmental constituencies, and the public. The Natural Resource Report Series is used to disseminate comprehensive information and analysis about natural resources and related topics concerning lands managed by the National Park Service. -
Metaproteogenomic Insights Beyond Bacterial Response to Naphthalene
ORIGINAL ARTICLE ISME Journal – Original article Metaproteogenomic insights beyond bacterial response to 5 naphthalene exposure and bio-stimulation María-Eugenia Guazzaroni, Florian-Alexander Herbst, Iván Lores, Javier Tamames, Ana Isabel Peláez, Nieves López-Cortés, María Alcaide, Mercedes V. del Pozo, José María Vieites, Martin von Bergen, José Luis R. Gallego, Rafael Bargiela, Arantxa López-López, Dietmar H. Pieper, Ramón Rosselló-Móra, Jesús Sánchez, Jana Seifert and Manuel Ferrer 10 Supporting Online Material includes Text (Supporting Materials and Methods) Tables S1 to S9 Figures S1 to S7 1 SUPPORTING TEXT Supporting Materials and Methods Soil characterisation Soil pH was measured in a suspension of soil and water (1:2.5) with a glass electrode, and 5 electrical conductivity was measured in the same extract (diluted 1:5). Primary soil characteristics were determined using standard techniques, such as dichromate oxidation (organic matter content), the Kjeldahl method (nitrogen content), the Olsen method (phosphorus content) and a Bernard calcimeter (carbonate content). The Bouyoucos Densimetry method was used to establish textural data. Exchangeable cations (Ca, Mg, K and 10 Na) extracted with 1 M NH 4Cl and exchangeable aluminium extracted with 1 M KCl were determined using atomic absorption/emission spectrophotometry with an AA200 PerkinElmer analyser. The effective cation exchange capacity (ECEC) was calculated as the sum of the values of the last two measurements (sum of the exchangeable cations and the exchangeable Al). Analyses were performed immediately after sampling. 15 Hydrocarbon analysis Extraction (5 g of sample N and Nbs) was performed with dichloromethane:acetone (1:1) using a Soxtherm extraction apparatus (Gerhardt GmbH & Co. -

Extremozymes of the Hot and Salty Halothermothrix Orenii
Extremozymes of the Hot and Salty Halothermothrix orenii Author Kori, Lokesh D Published 2012 Thesis Type Thesis (PhD Doctorate) School School of Biomolecular and Physical Sciences DOI https://doi.org/10.25904/1912/2191 Copyright Statement The author owns the copyright in this thesis, unless stated otherwise. Downloaded from http://hdl.handle.net/10072/366220 Griffith Research Online https://research-repository.griffith.edu.au Extremozymes of the hot and salty Halothermothrix orenii LOKESH D. KORI (M.Sc. Biotechnology) School of Biomolecular and Physical Sciences Science, Environment, Engineering and Technology Griffith University, Australia Submitted in fulfillment of the requirements of the degree of Doctor of Philosophy December 2011 STATEMENT OF ORIGINALITY STATEMENT OF ORIGINALITY This work has not previously been submitted for a degree or diploma in any university. To the best of my knowledge and belief, the thesis contains no material previously published or written by another person except where due reference is made in the thesis itself. LOKESH DULICHAND KORI II ACKNOWLEDGEMENTS ACKNOWLEDGEMENTS I owe my deepest gratitude to my supervisor Prof. Bharat Patel, for offering me an opportunity for being his postgraduate. His boundless knowledge motivates me for keep going and enjoy the essence of science. Without his guidance, great patience and advice, I could not finish my PhD program successfully. I take this opportunity to give my heartiest thanks to Assoc. Prof. Andreas Hofmann, (Structural Chemistry, Eskitis Institute for Cell & Molecular Therapies, Griffith University) for his support and encouragement for crystallographic work. I am grateful to him for teaching me about the protein structures, in silico analysis and their hidden chemistry. -

Tessaracoccus Arenae Sp. Nov., Isolated from Sea Sand
TAXONOMIC DESCRIPTION Thongphrom et al., Int J Syst Evol Microbiol 2017;67:2008–2013 DOI 10.1099/ijsem.0.001907 Tessaracoccus arenae sp. nov., isolated from sea sand Chutimon Thongphrom,1 Jong-Hwa Kim,1 Nagamani Bora2,* and Wonyong Kim1,* Abstract A Gram-stain positive, non-spore-forming, non-motile, facultatively anaerobic bacterial strain, designated CAU 1319T, was isolated from sea sand and the strain’s taxonomic position was investigated using a polyphasic approach. Strain CAU 1319T grew optimally at 30 C and at pH 7.5 in the presence of 2 % (w/v) NaCl. Phylogenetic analysis, based on the 16S rRNA gene sequence, revealed that strain CAU 1319T belongs to the genus Tessaracoccus, and is closely related to Tessaracoccus lapidicaptus IPBSL-7T (similarity 97.69 %), Tessaracoccus bendigoensis Ben 106T (similarity 95.64 %) and Tessaracoccus T T flavescens SST-39 (similarity 95.84 %). Strain CAU 1319 had LL-diaminopimelic acid as the diagnostic diamino acid in the cell-wall peptidoglycan, MK-9 (H4) as the predominant menaquinone, and anteiso-C15 : 0 as the major fatty acid. The polar lipids consisted of phosphatidylglycerol, phosphatidylinositol, two unidentified aminolipids, three unidentified phospholipids and one unidentified glycolipid. Predominant polyamines were spermine and spermidine. The DNA–DNA hybridization value between strain CAU 1319T and T. lapidicaptus IPBSL-7T was 24 %±0.2. The DNA G+C content of the novel strain was 69.5 mol %. On the basis of phenotypic and chemotaxonomic properties, as well as phylogenetic relatedness, strain CAU 1319Tshould be classified as a novel species of the genus Tessaracoccus, for which the name Tessaracoccus arenae sp. -
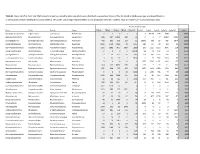
Table S1. Bacterial Otus from 16S Rrna
Table S1. Bacterial OTUs from 16S rRNA sequencing analysis including only taxa which were identified to genus level (those OTUs identified as Ambiguous taxa, uncultured bacteria or without genus-level identifications were omitted). OTUs with only a single representative across all samples were also omitted. Taxa are listed from most to least abundant. Pitcher Plant Sample Class Order Family Genus CB1p1 CB1p2 CB1p3 CB1p4 CB5p234 Sp3p2 Sp3p4 Sp3p5 Sp5p23 Sp9p234 sum Gammaproteobacteria Legionellales Coxiellaceae Rickettsiella 1 2 0 1 2 3 60194 497 1038 2 61740 Alphaproteobacteria Rhodospirillales Rhodospirillaceae Azospirillum 686 527 10513 485 11 3 2 7 16494 8201 36929 Sphingobacteriia Sphingobacteriales Sphingobacteriaceae Pedobacter 455 302 873 103 16 19242 279 55 760 1077 23162 Betaproteobacteria Burkholderiales Oxalobacteraceae Duganella 9060 5734 2660 40 1357 280 117 29 129 35 19441 Gammaproteobacteria Pseudomonadales Pseudomonadaceae Pseudomonas 3336 1991 3475 1309 2819 233 1335 1666 3046 218 19428 Betaproteobacteria Burkholderiales Burkholderiaceae Paraburkholderia 0 1 0 1 16051 98 41 140 23 17 16372 Sphingobacteriia Sphingobacteriales Sphingobacteriaceae Mucilaginibacter 77 39 3123 20 2006 324 982 5764 408 21 12764 Gammaproteobacteria Pseudomonadales Moraxellaceae Alkanindiges 9 10 14 7 9632 6 79 518 1183 65 11523 Betaproteobacteria Neisseriales Neisseriaceae Aquitalea 0 0 0 0 1 1577 5715 1471 2141 177 11082 Flavobacteriia Flavobacteriales Flavobacteriaceae Flavobacterium 324 219 8432 533 24 123 7 15 111 324 10112 Alphaproteobacteria -

UCC Library and UCC Researchers Have Made This Item Openly Available. Please Let Us Know How This Has Helped You. Thanks! Downlo
UCC Library and UCC researchers have made this item openly available. Please let us know how this has helped you. Thanks! Title Bacterial inhabitants of tumours: methods for exploration and exploitation Author(s) Walker, Sidney P. Publication date 2020-05-04 Original citation Walker, S. P. 2020. Bacterial inhabitants of tumours: methods for exploration and exploitation. PhD Thesis, University College Cork. Type of publication Doctoral thesis Rights © 2020, Sidney P. Walker. https://creativecommons.org/licenses/by-nc-nd/4.0/ Item downloaded http://hdl.handle.net/10468/10055 from Downloaded on 2021-10-08T08:21:36Z Coláiste na hOllscoile, Corcaigh THE NATIONAL UNIVERSITY OF IRELAND, CORK School of Microbiology Bacterial inhabitants of tumours: Methods for exploration and exploitation Thesis presented by Sidney Walker Under the supervision of Dr. Mark Tangney and Dr. Marcus Claesson For the degree of Doctor of Philosophy 2016-2020 1 Contents Abstract .................................................................................................................................................. 3 Chapter I: Literature Review .............................................................................................................. 7 Section 1: Sequencing and the Microbiome ........................................................................ 7 The Microbiome ............................................................................................................... 8 Sequencing .................................................................................................................... -

Effect of Vertical Flow Exchange on Microbial Community Dis- Tributions in Hyporheic Zones
Article 1 by Heejung Kim and Kang-Kun Lee* Effect of vertical flow exchange on microbial community dis- tributions in hyporheic zones School of Earth and Environmental Sciences, Seoul National University, Seoul 08826, Republic of Korea; *Corresponding author, E-mail: [email protected] (Received: November 2, 2018; Revised accepted: January 6, 2019) https://doi.org/10.18814/epiiugs/2019/019001 The effect of the vertical flow direction of hyporheic flux advance of hydrodynamic modeling has improved research of hydro- on the bacterial community is examined. Vertical velocity logical exchange processes at the hyporheic zone (Cardenas and Wil- change of the hyporheic zone was examined by installing son, 2007; Fleckenstein et al., 2010; Endreny et al., 2011). Also, this a piezometer on the site, and a total of 20,242 reads were zone has plentiful micro-organisms. The hyporheic zone constituents analyzed using a pyrosequencing assay to investigate the a dynamic hotspot (ecotone) where groundwater and surface water diversity of bacterial communities. Proteobacteria (55.1%) mix (Smith et al., 2008). were dominant in the hyporheic zone, and Bacteroidetes This area constitutes a flow path along which surface water down wells into the streambed sediment and groundwater up wells in the (16.5%), Actinobacteria (7.1%) and other bacteria phylum stream, travels for some distance before eventually mixing with (Firmicutes, Cyanobacteria, Chloroflexi, Planctomycetesm groundwater returns to the stream channel (Hassan et al., 2015). Sur- and unclassified phylum OD1) were identified. Also, the face water enters the hyporheic zone when the vertical hydraulic head hyporheic zone was divided into 3 points – down welling of surface water is greater than the groundwater (down welling). -

The Mysterious Orphans of Mycoplasmataceae
The mysterious orphans of Mycoplasmataceae Tatiana V. Tatarinova1,2*, Inna Lysnyansky3, Yuri V. Nikolsky4,5,6, and Alexander Bolshoy7* 1 Children’s Hospital Los Angeles, Keck School of Medicine, University of Southern California, Los Angeles, 90027, California, USA 2 Spatial Science Institute, University of Southern California, Los Angeles, 90089, California, USA 3 Mycoplasma Unit, Division of Avian and Aquatic Diseases, Kimron Veterinary Institute, POB 12, Beit Dagan, 50250, Israel 4 School of Systems Biology, George Mason University, 10900 University Blvd, MSN 5B3, Manassas, VA 20110, USA 5 Biomedical Cluster, Skolkovo Foundation, 4 Lugovaya str., Skolkovo Innovation Centre, Mozhajskij region, Moscow, 143026, Russian Federation 6 Vavilov Institute of General Genetics, Moscow, Russian Federation 7 Department of Evolutionary and Environmental Biology and Institute of Evolution, University of Haifa, Israel 1,2 [email protected] 3 [email protected] 4-6 [email protected] 7 [email protected] 1 Abstract Background: The length of a protein sequence is largely determined by its function, i.e. each functional group is associated with an optimal size. However, comparative genomics revealed that proteins’ length may be affected by additional factors. In 2002 it was shown that in bacterium Escherichia coli and the archaeon Archaeoglobus fulgidus, protein sequences with no homologs are, on average, shorter than those with homologs [1]. Most experts now agree that the length distributions are distinctly different between protein sequences with and without homologs in bacterial and archaeal genomes. In this study, we examine this postulate by a comprehensive analysis of all annotated prokaryotic genomes and focusing on certain exceptions. -
Identification of Pasteurella Species and Morphologically Similar Organisms
UK Standards for Microbiology Investigations Identification of Pasteurella species and Morphologically Similar Organisms Issued by the Standards Unit, Microbiology Services, PHE Bacteriology – Identification | ID 13 | Issue no: 3 | Issue date: 04.02.15 | Page: 1 of 28 © Crown copyright 2015 Identification of Pasteurella species and Morphologically Similar Organisms Acknowledgments UK Standards for Microbiology Investigations (SMIs) are developed under the auspices of Public Health England (PHE) working in partnership with the National Health Service (NHS), Public Health Wales and with the professional organisations whose logos are displayed below and listed on the website https://www.gov.uk/uk- standards-for-microbiology-investigations-smi-quality-and-consistency-in-clinical- laboratories. SMIs are developed, reviewed and revised by various working groups which are overseen by a steering committee (see https://www.gov.uk/government/groups/standards-for-microbiology-investigations- steering-committee). The contributions of many individuals in clinical, specialist and reference laboratories who have provided information and comments during the development of this document are acknowledged. We are grateful to the Medical Editors for editing the medical content. For further information please contact us at: Standards Unit Microbiology Services Public Health England 61 Colindale Avenue London NW9 5EQ E-mail: [email protected] Website: https://www.gov.uk/uk-standards-for-microbiology-investigations-smi-quality- and-consistency-in-clinical-laboratories UK Standards for Microbiology Investigations are produced in association with: Logos correct at time of publishing. Bacteriology – Identification | ID 13 | Issue no: 3 | Issue date: 04.02.15 | Page: 2 of 28 UK Standards for Microbiology Investigations | Issued by the Standards Unit, Public Health England Identification of Pasteurella species and Morphologically Similar Organisms Contents ACKNOWLEDGMENTS ......................................................................................................... -

Role of Protein Phosphorylation in Mycoplasma Pneumoniae
Pathogenicity of a minimal organism: Role of protein phosphorylation in Mycoplasma pneumoniae Dissertation zur Erlangung des mathematisch-naturwissenschaftlichen Doktorgrades „Doctor rerum naturalium“ der Georg-August-Universität Göttingen vorgelegt von Sebastian Schmidl aus Bad Hersfeld Göttingen 2010 Mitglieder des Betreuungsausschusses: Referent: Prof. Dr. Jörg Stülke Koreferent: PD Dr. Michael Hoppert Tag der mündlichen Prüfung: 02.11.2010 “Everything should be made as simple as possible, but not simpler.” (Albert Einstein) Danksagung Zunächst möchte ich mich bei Prof. Dr. Jörg Stülke für die Ermöglichung dieser Doktorarbeit bedanken. Nicht zuletzt durch seine freundliche und engagierte Betreuung hat mir die Zeit viel Freude bereitet. Des Weiteren hat er mir alle Freiheiten zur Verwirklichung meiner eigenen Ideen gelassen, was ich sehr zu schätzen weiß. Für die Übernahme des Korreferates danke ich PD Dr. Michael Hoppert sowie Prof. Dr. Heinz Neumann, PD Dr. Boris Görke, PD Dr. Rolf Daniel und Prof. Dr. Botho Bowien für das Mitwirken im Thesis-Komitee. Der Studienstiftung des deutschen Volkes gilt ein besonderer Dank für die finanzielle Unterstützung dieser Arbeit, durch die es mir unter anderem auch möglich war, an Tagungen in fernen Ländern teilzunehmen. Prof. Dr. Michael Hecker und der Gruppe von Dr. Dörte Becher (Universität Greifswald) danke ich für die freundliche Zusammenarbeit bei der Durchführung von zahlreichen Proteomics-Experimenten. Ein ganz besonderer Dank geht dabei an Katrin Gronau, die mich in die Feinheiten der 2D-Gelelektrophorese eingeführt hat. Außerdem möchte ich mich bei Andreas Otto für die zahlreichen Proteinidentifikationen in den letzten Monaten bedanken. Nicht zu vergessen ist auch meine zweite Außenstelle an der Universität in Barcelona. Dr. Maria Lluch-Senar und Dr. -

Extensive Microbial Diversity Within the Chicken Gut Microbiome Revealed by Metagenomics and Culture
Extensive microbial diversity within the chicken gut microbiome revealed by metagenomics and culture Rachel Gilroy1, Anuradha Ravi1, Maria Getino2, Isabella Pursley2, Daniel L. Horton2, Nabil-Fareed Alikhan1, Dave Baker1, Karim Gharbi3, Neil Hall3,4, Mick Watson5, Evelien M. Adriaenssens1, Ebenezer Foster-Nyarko1, Sheikh Jarju6, Arss Secka7, Martin Antonio6, Aharon Oren8, Roy R. Chaudhuri9, Roberto La Ragione2, Falk Hildebrand1,3 and Mark J. Pallen1,2,4 1 Quadram Institute Bioscience, Norwich, UK 2 School of Veterinary Medicine, University of Surrey, Guildford, UK 3 Earlham Institute, Norwich Research Park, Norwich, UK 4 University of East Anglia, Norwich, UK 5 Roslin Institute, University of Edinburgh, Edinburgh, UK 6 Medical Research Council Unit The Gambia at the London School of Hygiene and Tropical Medicine, Atlantic Boulevard, Banjul, The Gambia 7 West Africa Livestock Innovation Centre, Banjul, The Gambia 8 Department of Plant and Environmental Sciences, The Alexander Silberman Institute of Life Sciences, Edmond J. Safra Campus, Hebrew University of Jerusalem, Jerusalem, Israel 9 Department of Molecular Biology and Biotechnology, University of Sheffield, Sheffield, UK ABSTRACT Background: The chicken is the most abundant food animal in the world. However, despite its importance, the chicken gut microbiome remains largely undefined. Here, we exploit culture-independent and culture-dependent approaches to reveal extensive taxonomic diversity within this complex microbial community. Results: We performed metagenomic sequencing of fifty chicken faecal samples from Submitted 4 December 2020 two breeds and analysed these, alongside all (n = 582) relevant publicly available Accepted 22 January 2021 chicken metagenomes, to cluster over 20 million non-redundant genes and to Published 6 April 2021 construct over 5,500 metagenome-assembled bacterial genomes. -
Metal Transformation by a Novel Pelosinus Isolate from a Subsurface Environment
INL/JOU-08-14091-Revision-0 Metal Transformation by a Novel Pelosinus Isolate From a Subsurface Environment Allison E. Ray, Peter P. Sheridan, Andrew L. Neal, Yoshiko Fujita, David E. Cummings, Timothy S. Magnuson August 2018 The INL is a U.S. Department of Energy National Laboratory operated by Battelle Energy Alliance INL/JOU-08-14091-Revision-0 Metal Transformation by a Novel Pelosinus Isolate From a Subsurface Environment Allison E. Ray, Peter P. Sheridan, Andrew L. Neal, Yoshiko Fujita, David E. Cummings, Timothy S. Magnuson August 2018 Idaho National Laboratory Idaho Falls, Idaho 83415 http://www.inl.gov Prepared for the U.S. Department of Energy Office of Nuclear Energy Under DOE Idaho Operations Office Contract DE-AC07-05ID14517 fmicb-09-01689 July 25, 2018 Time: 20:42 # 1 ORIGINAL RESEARCH published: xx July 2018 doi: 10.3389/fmicb.2018.01689 1 58 2 59 3 60 4 61 5 62 6 63 7 64 8 65 9 Metal Transformation by a Novel 66 10 67 11 Pelosinus Isolate From a Subsurface 68 12 69 13 Environment 70 14 71 15 Allison E. Ray1,2, Stephanie A. Connon1,3, Andrew L. Neal4†, Yoshiko Fujita2, 72 5 2† 1 16 David E. Cummings , Jani C. Ingram and Timothy S. Magnuson * 73 17 74 1 Department of Biological Sciences, Idaho State University, Pocatello, ID, United States, 2 Bioenergy Technologies, Idaho 18 3 75 Edited by: National Laboratory, Idaho Falls, ID, United States, California Institute of Technology, Pasadena, CA, United States, 19 4 5 76 Pankaj Kumar Arora, Savannah River Ecology Laboratory, University of Georgia, Aiken, SC, United States, Department of Biology, Point Loma 20 77 Babasaheb Bhimrao Ambedkar Nazarene University, San Diego, CA, United States 21 University, India 78 22 79 Reviewed by: The capability of microorganisms to alter metal speciation offers potential for 23 80 Ramprasad E.V.V., the development of new strategies for immobilization of toxic metals in the 24 University of Hyderabad, India 81 25 Bärbel Ulrike Fösel, environment.