Application of Logistic Regression and Principal Component Analysis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Webinar Report On
1 Report on National Webinar on “Role of IQAC in Higher Education Institutions” Organized by IQAC, B N College, Dhubri, Assam Convener : Dr. Susmita Sen Gupta, Coordinator-IQAC B N College, Dhubri, Assam Platform : Video conferencing through Google Meet Date : 7th July, 2020 (10.30 am to 1.00 pm) 2 The National Webinar on “Role of IQAC in Higher Education Institutions” was organized by Internal Quality Assurance Cell, B N College, Dhubri, Assam on 02/07/2020, through video conferencing using Google Meet platform along with live streaming in facebook and college website. The Webinar was organised with the aim of taking initiatives to reach out the Higher Education Institutions (HEIs) of India for quality enhancements and quality sustenance. A total of 150 participants comprising Principals of affiliated colleges, IQAC coordinators, faculty members of affiliated colleges and universities attended the Webinar through Google Meet and many more through facebook and college website. The Webinar started at 10.30 am with the Welcome Address delivered by Dr. Dhruba Chakrabortty, Principal, B N College, Dhubri, Assam. He briefed about the purpose and necessity of such webinar. Dr Chakrabortty gave an introduction of the college to the participants. He extended a warm welcome to the resource person, Dr Ganesh A. Hedge, advisor, NAAC, the inaugurator, Prof Bhaben Tanti, Director, IQAC, Gauhati University and all the participants of the Webinar. In his inaugural speech, Prof. Bhaben Tanti greeted the resource person and all the participants and mentioned that the establishment of IQAC is prerequisite for achieving quality in a higher education institution. Followed by the inaugural address, Dr. -

Dr. Somnath Paul Curriculum Vitae
Dr. Somnath Paul Curriculum vitae j CONTACT Assistant Professor Mobile: j INFORMATION Department of Applied Sciences (Mathematics) 9854581311/8876230579 Tezpur University, Napaam, Sonitpur j E-mail: [email protected] PO Box 784028 j [email protected] Assam, India. j EDUCATION Ph.D., Mathematical Sciences, 2014. • Tezpur University, Assam, India. • Thesis Title: On distance spectral radius and Laplacian matrices of graphs. • Supervisor: Dr. Milan Nath, Professor, Department of Mathematical Sciences, Tezpur University, Assam, India. • Area of Study: Spectral Graph Theory. M.Sc., Mathematics, 2008. • 1st class 1st position with 85% marks. • Department of Mathematics, Gauhati University, Guwahati, Assam, India. B.Sc., Mathematics (Honors), Physics and Statistics, 2006. • 1st class 11th position with distinction and 63.4% marks in Honors. • Bholanath College (Under Gauhati University), Dhubri, Assam, India. H.S., Physics, Chemistry, Mathematics, 2003. • 2nd division with 54.6% marks. • Sishupathsala H.S. School (Under AHSEC), Dhubri, Assam, India. H.S.L.C., 2001. • 1st division with 70% marks. • Vivekananda Vidyapith High School (Under SEBA), Dhubri, Assam, India. PROFESSIONAL EXPERIENCE 1. Assistant Professor- Department of Applied Sciences (Mathematics), Tezpur University, Assam, from 16/12/2019 till date. 2. Assistant Professor-Department of Mathematics, Pandit Deendayal Upadhyaya Adarsha Mahavidyalaya, Behali, Biswanath, Assam, from 09/08/2017 to 15/12/2019. 3. Assistant Professor (contractual) - Department of Mathematical Sciences, Tezpur University, Assam, from 17/12/2015 to 08/08/2017. 4. Assistant Professor (ad-hoc) - Department of Mathematical Sciences, Tezpur University, Assam, from 05/02/2014 to 15/12/2015. 1 of 7 5. Assistant Professor (contractual) - Department of Mathematics, NIT Silchar, Assam, from August 2013 to January 2014. -

Merit-List-Bsc-1St-Year-2019-20.Pdf
Merit List for Admission into B.Sc. 1st Year, Gossaigaon College, Gossaigaon Session: 2019-20 List of candidates of Gossaigaon College Year(Passed / Sl. No.Application No Candiate Name Course Type Gender Caste Institute Board % Appeared) 1 BSc/2019/93 MANASH PRATIM BARMAN Honours Male OBC GOSSAIGAON COLLEGE AHSEC 78.6 2017 2 BSc/2019/31 MD JAKIR HOSSAIN Honours Male General GOSSAIGAON COLLEGE AHSEC 71.6 2019 3 BSc/2019/91 MANIK SARKAR Honours Male SC GOSSAIGAON COLLEGE AHSEC 65.8 2019 4 BSc/2019/50 BISHNU DAS Regular Male SC GOSSAIGAON COLLEGE AHSEC 64.2 2016 5 BSc/2019/21 THOMAS KUMAR BASKEY Honours Male OBC GOSSAIGAON COLLEGE AHSEC 63.4 2019 6 BSc/2019/26 NIKESH MAJUMDAR Honours Male OBC GOSSAIGAON COLLEGE AHSEC 60.2 2019 7 BSc/2019/101 ANANTA ROY Regular Male OBC GOSSAIGAON COLLEGE AHSEC 58.8 2018 8 BSc/2019/3 NABANITA ROY SARKAR Honours Female OBC GOSSAIGAON COLLEGE AHSEC 56.4 2019 9 BSc/2019/27 SANDAN BASUMATARY Honours Male ST (P) GOSSAIGAON COLLEGE AHSEC 55.4 2019 10 BSc/2019/111 ADISONMARDI Honours Male OBC GOSSAIGAON COLLEGE AHSEC 55.4 2019 11 BSc/2019/71 UMANANDA KISKU Honours Male OBC GOSSAIGAON COLLEGE AHSEC 52.6 2019 12 BSc/2019/22 KAMESWARI DEVI BRAHMA Honours Female ST (P) GOSSAIGAON COLLEGE AHSEC 52 2019 13 BSc/2019/56 SURANJIT BARMAN Honours Male OBC GOSSAIGAON COLLEGE AHSEC 52 2019 14 BSc/2019/86 RAHUL MAHATO Honours Male OBC GOSSAIGAON COLLEGE AHSEC 50.4 2019 15 BSc/2019/100 AKWRANG NARZARY Honours Male ST (P) GOSSAIGAON COLLEGE AHSEC 49.8 2019 16 BSc/2019/97 AMIT KUMAR SAH Honours Male OBC GOSSAIGAON COLLEGE AHSEC -

Report on Two Day International Webinar on Impact of Covid-19
Report on ‘Two Day International Webinar on ‘Impact of Covid-19 Pandemic on Global Economy’ 22-23 June, 2020 Organised by Centre for Development Studies Department of Economics Rajiv Gandhi University, Arunachal Pradesh Part – I Organising Committee Chief Patron Prof. Saket Kushwaha, Vice-Chancellor, Rajiv Gandhi University Patrons Prof. Amitava Mitra, Pro Vice-Chancellor, Rajiv Gandhi University Prof. Tomo Riba, Registrar, Rajiv Gandhi University Advisors Prof. Tana Showren, Dean, Faculty of Social Sciences Prof. N.C. Roy, Professor, Department of Economics Prof. S.K. Nayak, Professor, Department of Economics Organising Chairperson/Convener Prof. Vandana Upadhyay, Head, Professor, Department of Economics Coordinator Dr. Maila Lama, Sr. Assistant Professor, Department of Economics Deputy Coordinator Dr. Dil. B. Gurung Assistant Professor, Department of Economics Assistant Coordinators Dr. Lijum Nochi, Sr. Assistant Professor, Department of Economics Dr. Anup Kr. Das, Sr. Assistant Professor, Department of Economics Dr. Prasenjit B. Baruah, Sr. Assistant Professor, Department of Economics 1 Part – II Seminar/ Workshop / Webinar / FDP /STPs etc. 2.1: Background / Concept Notes and Objectives The world has been affected by the novel coronavirus (Covid-19) pandemic since November 2019. The virus causes respiratory diseases in human beings from common cold to more rare and serious diseases such as the Severe Acute Respiratory Syndrome (SARS) and the Middle East Respiratory Syndrome (MERS), both of which have high mortality rates (WHO 2020). The UN Secretary General described it as the worst crisis being faced by mankind since World War-II. It may lead to enhanced instability, unrest and enhanced conflict (The Economic Times, April 1, 2020). There is a high risk associated with this disease as it is highly fatal and contagious. -
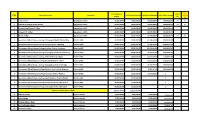
Sl NO Name of Institution Component Total Approved Amount Total Received Amount Total Released Amount Total Utilised Amount Ut
Non- Total Approved Utilised Sl NO Name of Institution Component Total Received amount Total Released Amount Total Utilised amount utilised amount (%) (%) 1 Tangla College Upgradation to MDC 40,000,000.00 40,000,000.00 40,000,000.00 40,000,000.00 100 NIL 2 Pub Kamrup College, Baihata Chariali Upgradation to MDC 40,000,000.00 40,000,000.00 40,000,000.00 40,000,000.00 100 NIL 3 Dergaon Kamal Dowerah College Upgradation to MDC 40,000,000.00 40,000,000.00 40,000,000.00 38,002,023.00 4 Sibsagar Girls’ College Upgradation to MDC 40,000,000.00 40,000,000.00 40,000,000.00 38,700,000.00 5 Dhemaji College Upgradation to MDC 40,000,000.00 40,000,000.00 40,000,000.00 40,000,000.00 100 NIL 6 Government Model Degree College Abhayapuri (North) District Bng Erstwhile MDC 90,000,000.00 83,000,000.00 111,399,629.00 80,000,000.00 7 Government Model Degree College Dalgaon District Darrang Erstwhile MDC 90,000,000.00 83,000,000.00 96,139,660.00 80,000,000.00 8 Government Model Degree College Dudhnoi District Goalpara Erstwhile MDC 90,000,000.00 83,000,000.00 101,666,684.00 80,000,000.00 9 Government Model Degree College Karimganj (South) District Krmg Erstwhile MDC 90,000,000.00 83,000,000.00 79,293,813.00 80,000,000.00 10 Government Model Degree College Bihali District Sonitpur Erstwhile MDC 90,000,000.00 83,000,000.00 61,217,889.00 71,679,572.00 11 Government Model Degree College Borkhola District Cachar Erstwhile MDC 90,000,000.00 53,000,000.00 49,450,809.00 50,000,000.00 12 Government Model Degree College Kakopothar District Tinsukia Erstwhile MDC 90,000,000.00 -

Behavioral Remodeling for Enhancing the Classroom Delivery of Teachers
Registration Form Course Coordinators from Academy Name of the Applicant (first, last): . Prof. Ratnajit Bhattacharjee ……………………………………………………. Affix passport Principal Investigator, E&ICT Academy, IIT Guwahati. …………………………………………………… size . Dr. Gaurav Trivedi Gender:…...……...……………………………..… An Initiative of photograph Co-Principal Investigator, E&ICT Academy, IIT Guwahati. Father’s Name:…...……...………………………… Ministry of Electronics & Information Technology . Dr. Dhruba Chakrabortty Mother’s Name :…...……...……………………… (MeitY), Government of India Designation: ……………………………………........................................... Principal, Bholanath College, Dhubri Highest Qualification: . Dr. Susmita Sengupta Electronics & ICT Academy ……………………………………………………………............................. Associate Professor, Dept. of Chemistry, IIT Guwahati, Assam Name and Address of the Bholanath College, Dhubri Organization/Institute:…………………………………………………….... A Faculty Development Programme on …………………………………………………………………………..….. Expert from Academy Category : Behavioral Remodeling for (GEN/OBC/SC/ST/Others)…………………………………………….….. Mr. Anjan Chowdhury enhancing the classroom Delivery City/town:………………………………………………...………………… CEO, Indian Skill Academy, & Empanelled member, of Teachers Email:…………………………………………………………….................. E&ICT Academy, IIT Guwahati Phone Number:…………………………………………………………………….. Course Objective Mobile To impart Soft Skill Development training to a level where Number:…………………………………………………......................... .... faculties will be benefitted in terms of the -

Gauhati University List of Applicants & Relevant Data As Submitted for Online Admission Into Traditonal Courses (G.U.), 2015 - 2016 36 Course : M.A
Gauhati University List of Applicants & relevant Data as submitted for Online Admission into Traditonal Courses (G.U.), 2015 - 2016 36 Course : M.A. POLITICAL SCIENCE Page 1 of 50 Pol Sci Relevant Gen.Obt Roll. No. C Name Gender Category District HSLC% Maj. Maj.Marks Fee Degree Year of Pass Sub Gen. Out Sr.No. App.No. F Name DOB Quota Assam Resi Mobile HSSLC Maj. Out OfMaj. % Gen.% Agr.% niversity Inst. Name 1 ADITYA AGARWALA MALE GENERAL KAMRUP METR 9864315731 92.83 YES 1410 82.94 B.A. 2015 15103452 ATMA RAM AGARWALA 17/09/1993 7-None YES 87 1700 GAUHATI COTTON COLLEGE, GUWAHATI 2 NIHARIKA SAIKIA FEMALE OBC TINSUKIA 7577951028 75.67 YES 8.5 80 B.A. 2015 15100182 ANANDA RAM SAIKIA 07/01/1994 7-None YES 85 10 GAUHATI COTTON COLLEGE 3 SABINA YESMIN FEMALE GENERAL MORIGAON 9864722729 63.67 YES 1352 79.53 B.A. 2015 15103706 KHALILUR RAHMAN 13/06/1994 7-None YES 75.6 1700 GAUHATI MOIRABARI COLLEGE, MOIRABARI 4 MANISHA KALITA FEMALE GENERAL MORIGAON 9864882585 85.5 YES 1349 79.35 B.A. 2015 15101801 KESHAB KALITA 16/12/1993 7-None YES 83.8 1700 GAUHATI MORIGAON COLLEGE 5 NABAJIT DEKA MALE GENERAL NALBARI 8011222109 51.67 YES 1340 78.82 B.A. 2015 15100900 DIPAK DEKA 02/05/1993 7-None YES 80.6 1700 GAUHATI KAMRUP COLLEGE CHAMATA 6 SUSHILA TAMANG FEMALE OBC KAMRUP RURA 7399377477 43.33 YES 1330 78.24 B.A. 2015 15100977 BIR BAHADUR TAMANG 19/11/1993 7-None YES 61.6 1700 GAUHATI SARAIGHAT COLLEGE 7 GITIKA BORAH FEMALE OBC SONITPUR 7399866732 85.33 YES 1316 77.41 B.A. -

Sanction List of Educational Assistance Extended to the Beneficiaries of the District Dhubri for the Year 2020 List:2
Page No.1 of 16 Sanction list of Educational Assistance extended to the beneficiaries of the District Dhubri for the year 2020 List:2 Sl. Student/ Beneficiary Address Registration Name of the Institute/ College Class A/c Holder Bank Detail Amount No. Applicant Name Village P.O No. & Registration Name Name Bank A/c Number IFSC Branch Name Date Office Name L.I. Mankachar (Resubmitted Application) 1 Sayed Zamal Nal Miah Puran Diara Puran Diara DHB/MCR/42 L.I. Puran Diara Jatiya VIII Sayed Zamal SBI 38371966832 SBIN0008267 Hatsingimari 4000 Sk dt.29.11.2016 Mankachar Vidyalaya Sk 2 Khairul Islam Abdul Khalek Chengur Puran Diara DHB/MCR/22 L.I. Janata HS School IX Khairul SBI 36081830804 SBIN0008267 Hatsingimari 4000 SK Char dt.09.02.2016 Mankachar Islam 3 Prokash Paul Lakhi Kanta Paul Para Mankachar DHB/MCR/51 L.I. Vivekananda ME VIII Prokash Paul SBI 36275137934 SBIN0014257 Mankachar 4000 Paul dt.02.06.2018 Mankachar School 4 Sumi Barman Sunil Barman Barman Para Mankachar DHB/MCR/48 L.I. 1926 No. Bapuji IV Sumi SBI 32896405023 SBIN0014257 Mankachar 1500 dt.02.06.2018 Mankachar Girls LP School Barman 5 Shekh Forid Ishadul Bhat Jhagrar Kakri Para DHB/MCR/62 L.I. Gyandeep Jatio IV Ishadul SBI 38464906232 SBIN0014257 Mankachar 1500 Hoque Char dt.02.06.2018 Mankachar Vidyalaya Hoque 6 Ashik Ekbal Abdul Matin Baliabil Kalapani DHB/MCR/19 L.I. All Ameen Ismail VIII Ashik Ekbal UCO 26383211001799 UCBA0002638 Jhawdanga Pt 4000 Mollah Mollah dt.09.02.2016 Mankachar Hussain Ideal Mollah III School 7 Rakesh Ch Sanjay Kr Kukur Mara Radha DHB/MCR/67 L.I. -

2020-2021 (As on 31 July, 2020)
NATIONAL ASSESSMENT AND ACCREDITATION COUNCIL (NAAC) Universities accredited by NAAC having valid accreditations during the period 01.07.2020 to 30.06.2021 ACCREDITATION VALID S. NO. STATE NAME UPTO 1 Andhra Pradesh Acharya Nagarjuna University, Guntur – 522510 (Third Cycle) 12/15/2021 2 Andhra Pradesh Andhra University,Visakhapatnam–530003 (Third Cycle) 2/18/2023 Gandhi Institute of Technology and Management [GITAM] (Deemed-to-be-University u/s 3 of the UGC Act 1956), 3 Andhra Pradesh 3/27/2022 Rushikonda, Visakhapatnam – 530045 (Second Cycle) 4 Andhra Pradesh Jawaharlal Nehru Technological University Kakinada, East Godavari, Kakinada – 533003 (First Cycle) 5/1/2022 Rashtriya Sanskrit Vidyapeetha (Deemed-to-be-University u/s 3 of the UGC Act 1956), Tirupati – 517507 (Second 5 Andhra Pradesh 11/14/2020 Cycle) 6 Andhra Pradesh Sri Krishnadevaraya University Anantapur – 515003 (Third Cycle) 5/24/2021 7 Andhra Pradesh Sri Padmavati Mahila Visvavidyalayam, Tirupati – 517502 (Third Cycle) 9/15/2021 8 Andhra Pradesh Sri Venkateswara University, Tirupati, Chittoor - 517502 (Third Cycle) 6/8/2022 9 Andhra Pradesh Vignan's Foundation for Science Technology and Research Vadlamudi (First Cycle) 11/15/2020 10 Andhra Pradesh Yogi Vemana University Kadapa (Cuddapah) – 516003 (First Cycle) 1/18/2021 11 Andhra Pradesh Dravidian University ,Srinivasavanam, Kuppam,Chittoor - 517426 (First Cycle) 9/25/2023 Koneru Lakshmaiah Education Foundation (Deemed-to-be-University u/s 3 of the UGC Act 1956),Green Fields, 12 Andhra Pradesh 11/1/2023 Vaddeswaram,Guntur -
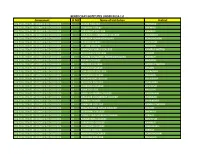
Component Sl NO Name of Institution District BENEFICIARY INSTITUTES
BENEFICIARY INSTITUTES UNDER RUSA 1.0 Component Sl NO Name of Institution District INFRASTRUCTURE GRANTS TO COLLEGES 1 DIGBOI COLLEGE TINSUKIA INFRASTRUCTURE GRANTS TO COLLEGES 2 Silapathar College DHEMAJI INFRASTRUCTURE GRANTS TO COLLEGES 3 SARAIGHAT COLLEGE KAMRUP INFRASTRUCTURE GRANTS TO COLLEGES 4 GOLAGHAT COMMERCE COLLEGE GOLAGHAT INFRASTRUCTURE GRANTS TO COLLEGES 5 BIRJHORA MAHAVIDYALAYA BONGAIGAON INFRASTRUCTURE GRANTS TO COLLEGES 6 TEZPUR COLLEGE SONITPUR INFRASTRUCTURE GRANTS TO COLLEGES 7 DR. BKB COLLEGE NAGAON INFRASTRUCTURE GRANTS TO COLLEGES 8 HANDIQUE GIRLS' COLLEGE KAMRUP METRO INFRASTRUCTURE GRANTS TO COLLEGES 9 BHOLANATH COLLEGE DHUBRI INFRASTRUCTURE GRANTS TO COLLEGES 10 PACHIM GUWAHATI MAHAVIDYALAYA KAMRUP INFRASTRUCTURE GRANTS TO COLLEGES 11 RUPAHI COLLEGE NAGAON INFRASTRUCTURE GRANTS TO COLLEGES 12 DIMORIA COLLEGE KAMRUP METRO INFRASTRUCTURE GRANTS TO COLLEGES 13 CHILARAI COLLEGE DHUBRI INFRASTRUCTURE GRANTS TO COLLEGES 14 JOYA GOGOI COLLEGE GOLAGHAT INFRASTRUCTURE GRANTS TO COLLEGES 15 KALIABOR COLLEGE NAGAON INFRASTRUCTURE GRANTS TO COLLEGES 16 KAMARGAON COLLEGE GOLAGHAT INFRASTRUCTURE GRANTS TO COLLEGES 17 DUDHNOI COLLEGE GOALPARA INFRASTRUCTURE GRANTS TO COLLEGES 18 DARRANG COLLEGE SONITPUR INFRASTRUCTURE GRANTS TO COLLEGES 19 RAHA COLLEGE NAGAON INFRASTRUCTURE GRANTS TO COLLEGES 20 NABIN CHANDRA COLLEGE KARIMGANJ INFRASTRUCTURE GRANTS TO COLLEGES 21 SIBSAGAR COMMERCE COLLEGE SIBSAGAR INFRASTRUCTURE GRANTS TO COLLEGES 22 SONARI COLLEGE CHARAIDEO INFRASTRUCTURE GRANTS TO COLLEGES 23 SONAPUR COLLEGE KAMRUP METRO -

1 Diversity of Culturable Endophytic Bacteria from Wild and Cultivated Rice Showed 2 Potential Plant Growth Promoting Activities
bioRxiv preprint doi: https://doi.org/10.1101/310797; this version posted April 30, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 1 1 Diversity of Culturable Endophytic bacteria from Wild and Cultivated Rice showed 2 potential Plant Growth Promoting activities 3 Madhusmita Borah, Saurav Das, Himangshu Baruah, Robin C. Boro, Madhumita Barooah* 4 Department of Agricultural Biotechnology, Assam Agricultural University, Jorhat, Assam 5 6 Authors Affiliations: 7 8 Madhusmita Borah: Department of Agricultural Biotechnology, Assam Agricultural 9 University, Jorhat, Assam. Email Id: [email protected] 10 11 Saurav Das: Department of Agricultural Biotechnology, Assam Agricultural University, 12 Jorhat, Assam. Email Id: [email protected] 13 14 Himangshu Baruah: Department of Agricultural Biotechnology, Assam Agricultural 15 University, Jorhat, Assam. Email Id: [email protected] 16 17 Robin Ch. Boro: Department of Agricultural Biotechnology, Assam Agricultural University, 18 Jorhat, Assam. Email Id: [email protected] 19 20 *Corresponding Author: 21 Madhumita Barooah: Professor, Department of Agricultural Biotechnology, Assam 22 Agricultural University, Jorhat, Assam. Emil Id: [email protected] 23 24 Present Address: 25 1. Saurav Das: DBT- Advanced Institutional Biotech Hub, Bholanath College, Dhubri, 26 Assam. 27 2. Himangshu Baruah: Department of Environmental Science, Cotton College State 28 University, Guwahati, Assam. 29 30 Abstract 31 In this paper, we report the endophytic microbial diversity of cultivated and wild Oryza 32 sativa plants including their functional traits related to multiple traits that promote plant 33 growth and development. -
AQAR: (Previous Academic Year) 17-18.Pdf
Yearly Status Report - 2018-2019 Part A Data of the Institution 1. Name of the Institution KOKRAJHAR GOVT. COLLEGE Name of the head of the Institution DR.BANABINA BRAHMA Designation Principal(in-charge) Does the Institution function from own campus Yes Phone no/Alternate Phone no. +913661270245 Mobile no. 8638471995 Registered Email [email protected] Alternate Email [email protected] Address W/NO-6, KOKRAJHAR TOWN City/Town Kokrajhar State/UT Assam Pincode 783370 2. Institutional Status Affiliated / Constituent Affiliated Type of Institution Co-education Location Urban Financial Status state Name of the IQAC co-ordinator/Director MRS. ANJALEE BASUMATARY Phone no/Alternate Phone no. +913661270245 Mobile no. 9435020624 Registered Email [email protected] Alternate Email [email protected] 3. Website Address Web-link of the AQAR: (Previous Academic Year) http://www.kgc.edu.in/Documents/AQAR_20 17-18.pdf 4. Whether Academic Calendar prepared during Yes the year if yes,whether it is uploaded in the institutional website: Weblink : http://www.kgc.edu.in/Documents/Academi c%20calender%202018-19.pdf 5. Accrediation Details Cycle Grade CGPA Year of Validity Accrediation Period From Period To 1 B 71.05 2004 03-May-2004 02-May-2009 2 B 2.23 2015 15-Nov-2015 14-Nov-2020 6. Date of Establishment of IQAC 19-Aug-2002 7. Internal Quality Assurance System Quality initiatives by IQAC during the year for promoting quality culture Item /Title of the quality initiative by Date & Duration Number of participants/ beneficiaries IQAC Workshop on Personality 09-Apr-2019 89 Development & Mind Power 1 Workshop on Teaching 10-Apr-2019 45 Methodology 1 A workshop on CBCS-GU 15-May-2019 99 1 How to face NAAC 16-May-2019 65 inspection 1 View File 8.