Postpartum Nursing Care Pathway
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Department of Obstetrics and Gynecology
97 21 1 15,000 240 20 2011 21 30 24 115 80 30 770 UT SOUTHWESTERN 424 2,200 Department of Obstetrics and Gynecology 15 1974 15 1 314,000 NUMBERS2011 DISTINGUISH US PEOPLE75 SET US APART 71,299 14,000 240 3.8 600,000 10 17 770 3 1943 97 50 12 22,900 4 800 5,894 200 1.3 10 0 10,000 1 24 6,500 Numbers Distinguish Us People Set Us Apart Dear Friends, I am proud—and humbled—to introduce you to the Department of Obstetrics and Gynecology at UT Southwestern Medical Center. For more than 50 years, our department has been acknowledged for its contributions to women’s health care— both in obstetrics and gynecology. Our mission has remained unchanged since the department’s founding in 1943. Daily we strive for excellence in patient care, teaching, and research. In the clinical care realm, we provide comprehensive services in dual arenas—a private practice through the UT Southwestern Medical Center University Hospitals and Clinics and a public practice at Parkland Health and Hospital System. This blend not only maximizes our services throughout different segments of the community in which we live and work, but also provides an invigorating environment for our students, residents, fellows, and faculty. On the educational front, our faculty members are recognized as the authors of three major OB/GYN textbooks—Williams Obstetrics, Williams Gynecology, and Essential Reproductive Medicine. They are also responsible for the largest obstetrics and gynecology training program in the nation, with a combined total of 100 available residency positions in Dallas and Austin. -

Sex-Selective Abortions, Fertility, and Birth Spacing*
Sex-Selective Abortions, Fertility, and Birth Spacing* Claus C Portner¨ Department of Economics Albers School of Business and Economics Seattle University, P.O. Box 222000 Seattle, WA 98122 [email protected] www.clausportner.com & Center for Studies in Demography and Ecology University of Washington November 2016 *I am grateful to Andrew Foster and Darryl Holman for discussions about the method. I owe thanks to Shelly Lundberg, Daniel Rees, David Ribar, Hendrik Wolff, seminar participants at University of Copenhagen, University of Michigan, University of Washington, University of Arhus,˚ the Fourth Annual Conference on Population, Repro- ductive Health, and Economic Development, and the Economic Demography Workshop for helpful suggestions and comments. I would also like to thank Nalina Varanasi for research assistance. Support from the University of Wash- ington Royalty Research Fund and the Development Research Group of the World Bank is gratefully acknowledged. The views and findings expressed here are those of the author and should not be attributed to the World Bank or any of its member countries. Partial support for this research came from a Eunice Kennedy Shriver National Institute of Child Health and Human Development research infrastructure grant, 5R24HD042828, to the Center for Studies in Demography and Ecology at the University of Washington. Prior versions of this paper were presented under the title “The Determinants of sex-selective Abortions.” Abstract This paper addresses two main questions: what is the relationship between fertility and sex se- lection and how does birth spacing interact with the use of sex-selective abortions? I introduce a statistical method that incorporates how sex-selective abortions affect both the likelihood of a son and spacing between births. -

Nutrition in Andrology, Gynaecology and Obstetrics
Appendix No. 2 to the procedure of development and periodical review of syllabuses Nutrition in Andrology, Gynaecology and Obstetrics 1. Imprint Faculty name: English Division Syllabus (field of study, level and educational profile, form of studies, Medicine, 1st level studies, practical profile, full time e.g., Public Health, 1st level studies, practical profile, full time): Academic year: 2019/2020 Nutrition in Andrology, Gynaecology and Module/subject name: Obstetrics Subject code (from the Pensum system): Educational units: Department of Social Medicine and Public Health Head of the unit/s: Dr hab. n. med. Aneta Nitsch - Osuch Study year (the year during which the 1st-6th respective subject is taught): Study semester (the semester during which the respective subject is Winter and Summer semesters taught): Module/subject type (basic, corresponding to the field of study, Optional optional): Teachers (names and surnames and Anna Jagielska, MD degrees of all academic teachers of Aleksandra Kozłowska, BSc respective subjects): ERASMUS YES/NO (Is the subject available for students under the YES ERASMUS programme?): A person responsible for the syllabus (a person to which all comments to Anna Jagielska, MD the syllabus should be reported) Number of ECTS credits: 2 Page 1 of 4 Appendix No. 2 to the procedure of development and periodical review of syllabuses 2. Educational goals and aims The aim of the course is to provide students with: 1. The principles of nutrition during adolescence, adulthood and eldery. 2. The relationship between nutrition and fertility, fetal status and communicable diseases in the adults life. 3. Basics of dietary advices for men and women in the reproductive years. -

Womens Perception of Their Childbirth Expereinces: an Integrated Literature Review
University of Central Florida STARS Honors Undergraduate Theses UCF Theses and Dissertations 2019 Womens Perception of Their Childbirth Expereinces: An Integrated Literature Review Nancy M. Farmer University of Central Florida Part of the Maternal, Child Health and Neonatal Nursing Commons Find similar works at: https://stars.library.ucf.edu/honorstheses University of Central Florida Libraries http://library.ucf.edu This Open Access is brought to you for free and open access by the UCF Theses and Dissertations at STARS. It has been accepted for inclusion in Honors Undergraduate Theses by an authorized administrator of STARS. For more information, please contact [email protected]. Recommended Citation Farmer, Nancy M., "Womens Perception of Their Childbirth Expereinces: An Integrated Literature Review" (2019). Honors Undergraduate Theses. 565. https://stars.library.ucf.edu/honorstheses/565 WOMEN’S PERCEPTION OF THEIR CHILDBIRTH EXPERIENCES: AN INTEGRATIVE REVIEW OF THE LITERATURE by NANCY M. FARMER A thesis submitted in partial fulfillment of the requirements for the Honors in the Major Program in Nursing in the College of Nursing and in The Burnett Honors College at the University of Central Florida: Orlando, Florida Summer Term 2019 Thesis Chair: Angeline Bushy, PhD, RN, FAAN © 2019 Nancy Farmer ii Abstract Pregnancy and childbirth are a unique and sacred time in many womens’ lives and the process of giving birth often leaves women and families in a vulnerable position. This integrated literature review examined birthing experiences from the maternal perspective and focused on the short-term and long- term implications of negatively perceived maternal experiences. While there are several international studies, only a few have published studies from the United States. -

Medicaid Payment Initiatives to Improve Maternal and Birth Outcomes
April 2019 Advising Congress on Medicaid and CHIP Policy Medicaid Payment Initiatives to Improve Maternal and Birth Outcomes Pregnant women in the United States experience delivery via cesarean and early elective deliveries at higher rates than medically recommended for positive outcomes (ACOG 2019, WHO 2015). Delivery via cesarean or induction may be desirable for complicated births, but when not medically indicated, such procedures pose health risks for both the woman and child, and may increase the length of a hospital stay and admissions to neonatal intensive care units, thereby increasing the cost of care (NCSL 2018, Ashton 2010, Kamath et al. 2009). The use of unnecessary interventions during delivery has significant implications for Medicaid, which is the nation’s largest payer of maternity care, paying for nearly half of all births (NGA 2014). State Medicaid programs are implementing payment initiatives to reduce unnecessary or potentially harmful procedures, such as non-medically indicated cesarean sections and early elective deliveries, as well as to improve access to prenatal and postpartum care. In this brief, we look at how state Medicaid programs are using payment incentives to improve maternal and birth outcomes. The brief first describes practices in maternity care that are known to influence maternal and birth outcomes. It then describes Medicaid payment models such as bundled payments, blended payments for delivery, pay for performance, and medical homes.1 The federal government, the states, and other stakeholders are undertaking many other initiatives to improve maternal and neonatal outcomes that are not payment based, but these are beyond the scope of this brief. -

Let's Talk Motherhood. a Postpartum Guide
Let’s talk motherhood A postpartum guide Adapted from the American College of Obstetricians and Gynecologists Contents 02 Contents 03 Introduction 06 Healthy baby information 12 Healing after labor and delivery 19 Exercise and nutrition 22 Resources Congratulations on your new baby! You are about to enter an exciting new phase of life. There will be plenty of sleepless nights, heartwarming cuddles and new challenges. This guide is intended to help keep you on track as your baby’s health progresses, make you feel less alone as your body changes after pregnancy and provide resources for further help. GEHA is proud to be your partner in this new life chapter. Adapted from Your Pregnancy and Childbirth Month to Month 02 geha.com/Maternity | HDHP, Standard and High plans by the American College of Obstetricians and Gynecologists Introduction Your first well-child visit should be two or three days after coming home from the hospital. Schedule of well-baby visits As a parent, you want your child to be healthy and develop normally. That’s why well-child doctor visits are so important, particularly in the first 15 months of life. Your child’s doctor can help you identify developmental milestones in your child’s physical, mental, language and social skills. Each well-child visit will include a complete physical examination. The doctor will check your baby’s growth and development and record your child’s height, weight and other important information. Tests for hearing, vision and other functions will be part of some visits. First year visits Second year visits Visits occur at ages one, two, four, six and Visits occur at ages 12, 15, 18 and 24 months. -

Archives of Women's Health & Gynecology
Archives of Women’s Health & Gynecology doi: 10.39127/2677-7124/AWHG:1000103 Tawfik W. Arch Women Heal Gyn: 103. Research Article Clinical Outcomes of Laparoscopic Repair of Paravaginal Defects Waleed Tawfik* Department of Obstetrics and Gynecology, Faculty of Medicine, Benha University, Benha, Egypt. *Corresponding author: Waleed Tawfik: Lecturer of Obstetrics and Gynecology, Faculty of Medicine, Benha University, Benha, Egypt. Citation: Tawfik W (2020) Clinical Outcomes of Laparoscopic Repair of Paravaginal Defects. Arch Women Heal Gyn: AWHG-103. Received Date: 31 March, 2020; Accepted Date: 03 April, 2020; Published Date: 08 April, 2020 Abstract In the era of minimally invasive surgeries, laparoscopic approach has been adopted in many surgical procedures as a successful alternative. Laparoscopic paravaginal repair is a good approach for surgical treatment of lateral type cystoceles. This prospective study was done to investigate whether laparoscopic paravaginal repair might be a reasonable alternative to open or vaginal routes in terms of success rate, operative and postoperative outcomes. Fifty patients with clinically diagnosed paravaginal defect were included in this study. The overall success rate in our study was 88 % after one year according to prolapse staging. This is nearly comparable to the results of most studies. Dividing the overall outcome into favorable and unfavorable, we reported that the unfavorable outcome was 22%. Unfavorable outcome includes cases of recurrence, persistent symptoms or appearance of new complaints. Conclusion: Although laparoscopic paravaginal repair offers an alternative method with shorter hospital stay, less postoperative pain and quicker recovery, but it still has its drawbacks. It needs long learning curve and has prolonged operative time. -

Pre and Interconception Health, Intentionality and Birth Spacing: Emerging Issues
PRE AND INTERCONCEPTION HEALTH, INTENTIONALITY AND BIRTH SPACING: EMERGING ISSUES Monday, May 21 1:30 PM - 3:00 PM #prematuritycollab Pre- and Interconception Health, Intentionality, and Birth Spacing: Emerging Approaches Prematurity Prevention Summit Building a Birth Equity Movement Welcome • Co-chairing the Prematurity Collaborative Clinical and Public Health Practice Workgroup ‣ With Vanessa Lee, MPH (HRSA) • Great group of people; very dedicated • Focus on 3 main topics: ‣ 17-P ‣ LDASA ‣ Intentionality and birth spacing Background • Approximately half of pregnancies in US are unintended ‣ Better in teens, but still unacceptably high • Intentionality is important ‣ Unintended pregnancy associated with adverse maternal and child outcomes ‣ Negative impact on physical and mental health ‣ Disproportionate impact › Higher rates in lower SES and lower levels of achieved education ‣ Expensive… › 2010 estimate: $21 billion in public expenditure for unintended pregnancy Background – Birth Spacing • Based on data suggesting short interpregnancy intervals associated with worse outcomes ‣ Including prematurity ‣ Others: fetal growth restriction, NICU admission, perinatal death • Intervals “debated”…. ‣ < 24 months, especially < 18 months • “Recommendations” to avoid short intervals ‣ Healthy People 2020 objective: 10% reduction in pregnancies within 18 months ‣ WHO: minimum birth-to-pregnancy spacing of 2 years ‣ ACOG: short intervals mentioned as a risk factor for preterm delivery and adverse neonatal outcomes • Widespread emphasis ‣ Made sense -

Postpartum Care of Taiwanese and Chinese Immigrant Women
City University of New York (CUNY) CUNY Academic Works All Dissertations, Theses, and Capstone Projects Dissertations, Theses, and Capstone Projects 2-2017 Retelling an Old Wife’s Tale: Postpartum Care of Taiwanese and Chinese Immigrant Women Kuan-Yi Chen The Graduate Center, City University of New York How does access to this work benefit ou?y Let us know! More information about this work at: https://academicworks.cuny.edu/gc_etds/1872 Discover additional works at: https://academicworks.cuny.edu This work is made publicly available by the City University of New York (CUNY). Contact: [email protected] RETELLING AN OLD WIFE’S TALE: POSTPARTUM CARE OF TAIWANESE AND CHINESE IMMIGRANT WOMEN by KUAN-YI CHEN A dissertation submitted to the Graduate Faculty in Sociology in partial fulfillment of the requirements for the degree of Doctor of Philosophy, The City University of New York 2017 © 2017 Kuan-Yi Chen All Rights Reserved ii Retelling an old wife’s tale: Postpartum care of Taiwanese and Chinese immigrant women by Kuan-Yi Chen This manuscript has been read and accepted for the Graduate Faculty in Sociology in satisfaction of the dissertation requirement for the degree of Doctor of Philosophy ______________________ _____________________________________ Date Barbara Katz Rothman Chair of Examining Committee ______________________ _____________________________________ Date Philip Kasinitz Executive Officer Supervisory Committee: Barbara Katz Rothman Margaret M. Chin Robert Courtney Smith THE CITY UNIVERSITY OF NEW YORK iii ABSTRACT Retelling an old wife’s tale: Postpartum care of Taiwanese and Chinese immigrant women by Kuan-Yi Chen Advisor: Barbara Katz Rothman The focus of this dissertation is the Chinese postpartum tradition zuoyuezi, often translated into English as doing-the-month. -
Turning Your Breech Baby to a Head-Down Position (External Cephalic Version)
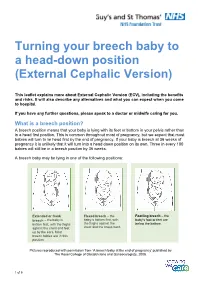
Turning your breech baby to a head-down position (External Cephalic Version) This leaflet explains more about External Cephalic Version (ECV), including the benefits and risks. It will also describe any alternatives and what you can expect when you come to hospital. If you have any further questions, please speak to a doctor or midwife caring for you. What is a breech position? A breech position means that your baby is lying with its feet or bottom in your pelvis rather than in a head first position. This is common throughout most of pregnancy, but we expect that most babies will turn to lie head first by the end of pregnancy. If your baby is breech at 36 weeks of pregnancy it is unlikely that it will turn into a head down position on its own. Three in every 100 babies will still be in a breech position by 36 weeks. A breech baby may be lying in one of the following positions: Extended or frank Flexed breech – the Footling breech – the breech – the baby is baby is bottom first, with baby’s foot or feet are bottom first, with the thighs the thighs against the below the bottom. against the chest and feet chest and the knees bent. up by the ears. Most breech babies are in this position. Pictures reproduced with permission from ‘A breech baby at the end of pregnancy’ published by The Royal College of Obstetricians and Gynaecologists, 2008. 1 of 5 What causes breech? Breech is more common in women who are expecting twins, or in women who have a differently-shaped womb (uterus). -
Presentation • on • Normal Puerperium •
• PRESENTATION • ON • NORMAL PUERPERIUM • • • Presented by: Ms. Uma Chandel • Nursing Lecturer, NIU • Subject: Obstetrics & Gynecology Definition Period following childbirth during which the body tissues ,specially the pelvic organs revert back approximately to the pre-pregnant state both anatomically and physiologically. Chapter. 17 Puerperium DURATION Includes 6 subsequent weeks postpartum during which normal pregnancy involution occurs This period is divided into :- Immediate period – within 24hours Early period- upto 7 days Remote period- upto6weeks Chapter. 17 Puerperium Physiological Aspects of the Puerperium Involution of the uterus Lochia Involution of other pelvic structures Breasts Menstruation & ovulation General physiological changes • INVOLUTION OF THE ANATOMICALUTERUS CONSIDERATIONS • uterus • lower uterine segment • cervix Uterus The uterus becomes firm with alternate hardening and softening. The uterus measures about 20 * 12 * 7.5 cm (Length, breadth and thickness) and weighs about 1000 gm. At the end of the 6 weeks it’s measurement is about 60 gm Lower Uterine Segment Immediately following delivery the lower segment become thin, flabby, collapsed structure. It takes few weeks to revert back to the normal shape and size Cervix It may be bruised and edematous. The cervix contract slowly, the external os admits 2 fingers for few days but by the end of the first week, narrows down to admit the tip of finger only. The Contour of cervix take a longer time to regain 6 week and the external os never revert back to the nulliparous state Chapter. 17 Puerperium LOCHIA It is the vaginal discharge of the first fortnight during puerperium lochia rubra : It is red in colour 1-4 days lochia serosa : yellowish or pale brownish in colour 5-9 days lochia alba : scantier and appears pale white 10-15 days The average amount of discharge for the first 5 -6 days ,is estimated to be 250ml. -

Glossary of Common MCH Terms and Acronyms
Glossary of Common MCH Terms and Acronyms General Terms and Definitions Term/Acronym Definition Accountable Care Organizations that coordinate and provide the full range of health care services for Organization individuals. The ACA provides incentives for providers who join together to form such ACO organizations and who agree to be accountable for the quality, cost, and overall care of their patients. Adolescence Stage of physical and psychological development that occurs between puberty and adulthood. The age range associated with adolescence includes the teen age years but sometimes includes ages younger than 13 or older than 19 years of age. Antepartum fetal Fetal death occurring before the initiation of labor. death Authorization An act of a legislative body that establishes government programs, defines the scope of programs, and sets a ceiling for how much can be spent on them. Birth defect A structural abnormality present at birth, irrespective of whether the defect is caused by a genetic factor or by prenatal events that are not genetic. Cost Sharing The amount an individual pays for health services above and beyond the cost of the insurance coverage premium. This includes co-pays, co-insurance, and deductibles. Crude birth rate Number of live births per 1000 population in a given year. Birth spacing The time interval from one child’s birth until the next child’s birth. It is generally recommended that at least a two-year interval between births is important for maternal and child health and survival. BMI Body mass index (BMI) is a measure of body weight that takes into account height.