Transportation Safety Board Railroad Accident/Incident
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Review of the Taylorville Energy Center's Facility
REVIEW OF THE TAYLORVILLE ENERGY CENTER’S FACILITY COST REPORT PRESENTED TO THE ILLINOIS COMMERCE COMMISSION BY BOSTON PACIFIC COMPANY, INC. AND MPR ASSOCIATES, INC. Boston Pacific Company, Inc. MPR Associates, Inc. Craig R. Roach, Ph.D. Jim Bubb, P.E. [email protected] [email protected] 1100 New York Avenue, NW, Suite 490 East 320 King Street, Suite 400 Washington, DC 20005 Alexandria, VA 22314 (202) 296-5520 (703) 519-0200 June 8, 2010 BOSTON PACIFIC COMPANY, INC. TABLE OF CONTENTS EXECUTIVE SUMMARY ....................................................................................................TAB 1 TASK 1 REPORT – A BACKGROUND REVIEW OF IGCC AND CARBON CAPTURE AND SEQUESTRATION PROJECTS TO DATE .............................................TAB 2 TASK 2 REPORT – AN ASSESSMENT OF TAYLORVILLE’S COMPLIANCE WITH THE ILLINOIS CLEAN COAL PORTFOLIO STANDARD LAW .........................TAB 3 TASK 3 REPORT – ASSESSMENT OF REASONABLENESS OF CAPITAL COSTS AND OPERATION COSTS FOR THE PROPOSED TAYLORVILLE ENERGY CENTER ................................................................................................................TAB 4 TASK 4 REPORT – ASSESSMENT OF POTENTIAL FOR THE TAYLORVILLE ENERGY CENTER TO COME ON-LINE AS PLANNED AND WITHIN THE PROPOSED TIMEFRAME ...................................................................................................TAB 5 TASK 5 REPORT – AN ASSESSMENT OF THE ABILITY TO FINANCE THE TAYLORVILLE FACILITY ..................................................................................................TAB -
St. Johns River Blueway by Dean Campbell River Overview
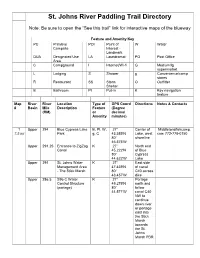
St. Johns River Paddling Trail Directory Note: Be sure to open the “See this trail” link for interactive maps of the blueway Feature and Amenity Key PC Primitive POI Point of W Water Campsite Interest - Landmark DUA Designated Use LA Laundromat PO Post Office Area C Campground I Internet/Wi-fi G Medium/lg supermarket L Lodging S Shower g Convenience/camp stores R Restaurant SS Storm O Outfitter Shelter B Bathroom PI Put-in K Key navigation feature Map River River Location Type of GPS Coord Directions Notes & Contacts # Basin Mile Description Feature (Degree (RM) or decimal Amenity minutes) 1 Upper 294 Blue Cypress Lake B, PI, W, 27° Center of Middletonsfishcamp. 7.5 mi Park g, C 43.589'N Lake, west com 772-778-0150 80° shoreline 46.575'W Upper 291.25 Entrance to ZigZag K 27° North end Canal 45.222'N of Blue 80° Cypress 44.622'W Lake Upper 291 St. Johns Water K 27° East side Management Area 47.439'N of canal - The Stick Marsh 80° C40 across 43.457'W dike Upper 286.5 S96 C Water K 27° Portage Control Structure 49.279'N north and (portage) 80° follow 44.571'W canal C40 NW to continue down river or portage east into the Stick Marsh towards the St. Johns Marsh PBR Upper 286.5 St. Johns Marsh – B, PI, W 27° East side Barney Green 49.393'N of canal PBR* 80° C40 across 42.537'W dike 2 Upper 286.5 St. Johns Marsh – B, PI, W 27° East side 22 mi Barney Green 49.393'N of canal *2 PBR* 80° C40 across day 42.537'W dike trip Upper 279.5 Great Egret PC 27° East shore Campsite 54.627'N of canal 80° C40 46.177'W Upper 277 Canal Plug in C40 K 27° In canal -
Recreation & Open Space Element
Putnam County COMPREHENSIVE PLAN RECREATION AND OPEN SPACE ELEMENT EAR-based Amendments Putnam County 2509 Crill Avenue, Suite 300 Palatka, FL 32178 Putnam County Recreation & Open Space Element Data & Analysis Recreation & Open Space Element Putnam County Table of Contents Section Page A. Introduction 2 B. Inventory of Facilities 2 1. County – owned Recreation Facilities 2 2. Public Access to Waterways 3 3. Facilities Owned and Operated by Other Agencies 4 4. Privately – owned Facilities 7 5. Open Spaces 8 6. Trails Master Plan 9 C. Analysis 9 1. Level – of – Service Standards 9 2. Recreation and Open Space Needs 10 List of Tables Table Page Table F-1: Inventory of Putnam County Parks and Recreation Facilities 2 Table F-2: Public Boat Ramps and Facilities 3 List of Maps Map Page Figure F-1: Existing Recreational Facilities: Community Parks 11 Figure F-2: Existing Recreational Facilities: Neighborhood Parks 12 Figure F-3: Putnam County Boat Ramp Locations 13 Figure F-4: Location of Existing Trails 14 Figure F-5: Location of Planned and Proposed Multi-Use Trails 15 Figure F-6: Location of Proposed Bike Routes 16 Figure F-7: Location of Proposed Equestrian and Hiking Trails 17 Figure F-8: Location of Proposed Paddling Trails 18 EAR-based Amendments 10/26/10 F - 1 Putnam County Recreation & Open Space Element Data & Analysis A. Introduction Putnam County adopted its Evaluation and Appraisal Report (EAR) in 2009. The data and analysis for the Recreation & Open Space Element is being updated to address the recommendations of the EAR and to extend the short term and long range planning timeframes to 2015 and 2025, respectively. -

Putnam County
Putnam County August 28, 2013 • Volume 69, No. 15 (2 sections) Crescent City, Florida 50¢ (Includes 7% FL Sales Tax) Serving Satsuma • Pomona Park • Lake Como • Crescent City • Seville • Pierson • Welaka • Fruitland • Georgetown • East Palatka • Palatka • Interlachen since 1898 Coaching the Mature Driver The Putnam Safety Association will conduct Another Successful Fundraiser a “Coaching the Mature Driver” course which Mike Jones Staff Writer Bob Martin meets Florida requirements for the auto lia- President bility insurance discount for licensed drivers The second fund- Putnam Family Fitness aged 55 and above. The course will be held on raiser for William “BJ’ Center Wednesday, August 28, from 9 a.m. to 4 p.m. Laurie held this past at Putnam Safety Association, 218 St. John’s Saturday at Merrill Avenue, Palatka. The cost is $10. Call 386-328- Hancock & Turner In- 8007 to make your reservation. surance in Palatka was a success. A steady stream of bargain seek- Gem City Shrimp Blast ers turned out for the Celebrate the running of shrimp on the St. Stuff and Things Sale, Johns River! Downtown Palatka, Inc. announc- helping Laurie and es a new event at the City of Palatka’s River- his family move closer front Park. This new yearly event will be held to their goal of rais- on Labor Day weekend, with Saturday, August ing $50,000. All pro- 31, being the focus this year. The event will ceeds from the fund- include many different activities throughout raiser will go toward the day. Music and food will begin at 11 a.m., stem cell treatment Photos by Mike Jones and continue through 10 p.m. -
Heroes Rescue Horses P.M
Putnam’s only Locally Owned, Independent, Community Newspaper • Established in 1898. 2020 Only Serving Satsuma ● Pomona Park ● Lake Como ● Crescent City ● Seville ● Pierson ● Welaka ● Fruitland ● Georgetown ● East Palatka ● Palatka ● Interlachen ● Melrose ● San Mateo 50 ¢ January 1, 2020 • Vol. 78, No. 41 (2 sections) Crescent City, FL Firefighters Receive Rubbing Elbows Scout Report Hoods Palatka native who’s Scouts camp Local firefighters receive specialty worked with Tim at St. John’s hoods. Tebow and others. Landing. Page B3 Page B1 Page A4 Genealogy for Beginners The Spark Genealogy Workshop for absolute beginners will be held on Mon., Jan. 13 at 5 Heroes Rescue Horses p.m. at the Palatka Library at 601 College Rd., Horses rescued from over turned trailer near Putnam/ St. Johns County line. Palatka. Learn some of the absolute basics about how to get started on your genealogy journey with the Putnam County Archives. No technical jargon, judgment or pressure just a fun and friendly learning atmosphere! Life is Art gallery exhibit The Arts Council of Greater Palatka is pleased to invite you to their next Gallery Exhibit “Life is Art” by Judi Cain. Join them on Fri., Jan. 10 at the Larimer Arts Center Located at 216 Reid St., Palatka from 5:30 to 7:30 p.m. The show is free and open to the public with light refreshments available. For more information email to [email protected] or call 386- 328-8998. Woman’s Club Bingo The GFWC Woman’s Club of Welaka invites the public to Bingo Night on Fri., Jan. 24 starting at 5 p.m. -

Putnam County River
30 4 25 Fishing in Putnam County 1 The St. Johns River flows north for 310 miles from Indian County to the Atlantic Ocean, and is divided into three basins - upper, middle and lower. Putnam County is in the lower basin and centrally located to the river’s best fishing. Not 6 only has it earned the title of “Bass Capital of the World”, but it offers a list of other freshwater, saltwater, and brackish-water fishing. Freshwater species include the largemouth bass, black crappie (speckled perch), bluegill, WESTSIDE BAIT & TACKLE Bartram Paddling Routes in shellcracker, warmouth and catfish. Saltwater 33 MESSER STORES, INC. species include red fish, flounder, sea trout and 934 S. HWY. 19, PALATKA, FL 32177 Putnam County tarpon. Shrimp migrate up the brackish water ONE STOP SHOPPING FOR THE OUTDOORS SPORTSMAN during the summer months. Striped bass can be HUNTING * FISHING * LIVE BAIT 7 caught mostly during the fall and winter months. CUSTOM RODS 1. Grey’s Creek with Forrester Point ROD AND REEL REPAIRS (5.8 mi.) (386) 328-4035 From downtown Palatka south to Lake George, PROUD SPONSOR MBT TOURNAMENT TRAIL 2. Palatka to Rollestown Outbound some 42 nautical miles, the St. Johns tree- JAMES (JIMMY) A. DARBY, JR., VP/GEN MGR lined shores and extensive vegetation provide and Return (8.2 mi.) FACEBOOK-MESSERS BAIT 3. Murphy Creek Loop (6 mi.) excellent habitat for fish. Lake George is a 46,000 acre natural impoundment of the St. 4. Dunn’s Creek (5.47 mi. one-way) Johns. It is the second largest lake in the state, 5. -

Putnamdestination
PutnamPutnamDestination Your Complete Guide to Putnam County & 2019 Chamber Membership Directory A publication produced by PALATKA DAILY NEWS Moving Families Forward Putnam County School District 2018-19 he Putnam County School District serves a diverse population of students. We offer a broad selection of Topportunities for all students including AVID, career and technical programs, Advanced Placement classes, and dual enrollment. Students in grades K-12 can apply to participate in our Cambridge program of advanced studies and incoming 9th grade students can apply for the Collegiate High School program in partnership with St. Johns River State College. We are partnering with local businesses and community organizations to provide our students with more opportunities for real world and practical career experiences through our career and technical programs. The Putnam County School District is committed to the education of the whole child; our mission is to “inspire every student to think, to learn, to achieve, to care and to become a successful and responsible citizen”. We thank the community for its support. As we move forward together, we will continue to work hard every day to give your children every opportunity for success. Rick Surrency Putnam County Superintendent of Schools HEDSTROM & HARRIS, P.A. 601 St. Johns Ave., Palatka • www.hehalaw.com Family Law • Wills & Trusts • Probate • Real Estate Closings 386-385-3101 Moving Families Forward HEDSTROM & HARRIS, P.A. 601 St. Johns Ave., Palatka • www.hehalaw.com Family Law • Wills & Trusts • Probate • Real Estate Closings 386-385-3101 ontents 6C Putnam County 10 Our Communities: Palatka, Crescent City, Interlachen, About the cover… Welaka, Pomona Park, Melrose and Bostwick The St.